
Abstract
Extramedullary plasmacytomas are rare malignancies. Most cases (80%) are seen in the head and neck region, where they represent 1 % of all head and neck malignancies. We report a case of an extramedullary plasmacytoma of the tongue that was treated successfully with three-dimensional conformal radiotherapy. The patient was a 50-year-old woman who was admitted to our hospital with bilateral pain and ulceration on the sides of her tongue. Findings on magnetic resonance imaging and positron-emission tomography did not demonstrate any mass within the tongue or any lymphatic or distant metastasis. A tissue biopsy identified a plasma cell neoplasm. The patient was treated with a total dose of 50 Gy delivered in 2-Gy daily fractions. After 54 months of post-treatment follow-up, she exhibited no sign of systemic myeloma or local recurrence. This case is presented not only for the rarity of the tumor type, but also for its unusual location.
Introduction
Solitary plasmacytomas and extramedullary plasmacytomas are rare malignancies, accounting for less than 5% of all plasma cell neoplasms.1,2 While they can originate at any extramedullary site, most cases (80%) are seen in the head and neck region, where they represent 1% of all head and neck malignancies.3,4 Plasmacytomas have a predilection for men (male-to-female ratio: 3:1), and most patients are aged 50 to 70 years at presentation.5,6 The diagnosis is made by excluding multiple myeloma and by the absence of monoclonal protein in the serum or urine in conjunction with normal findings on both skeletal survey and bone marrow biopsy. Both the risk of lymph node involvement and the incidence of progression to multiple myeloma are less than 10%.7,8
Radiotherapy plays a pivotal role in the treatment of extramedullary plasmacytomas, even though the role of elective lymphatic irradiation is still a matter of debate. 9 Although the optimal dose of radiotherapy is not well defined, the currently recommended dose is more than 40 Gy10,11 Unlike multiple myeloma, extramedullary plasmacytoma responds well to local treatment. Reported 5-year local control rates after radical treatment range between 80 and 95%; overall survival at 10 years ranges widely—from 45 to 100% depending on whether transformation to multiple myeloma occurs.8,9
Solitary plasmacytoma of the tongue is extremely rare, with only a few cases reported in the literature.12–15 We report a new case.
Case Report
A 50-year-old woman presented with a 2-year history of recurrent pain in both sides of her tongue and an associated loss of taste sensation. During the previous 3 months, she developed tongue ulcerations, mild to moderate bleeding, and a small amount of swelling. She had a 10-year history of treatment for asthma and a 1 -year history of treatment for lichen planus. Her family history was unremarkable.
Physical examination revealed a tender, superficial, erosive ulceration covered with white plaques on both sides of the tongue (figure 1). Her tongue movements were normal. No tongue mass was palpated, nor was any cervical lymphadenopathy. Findings on the remainder of the physical examination were normal.
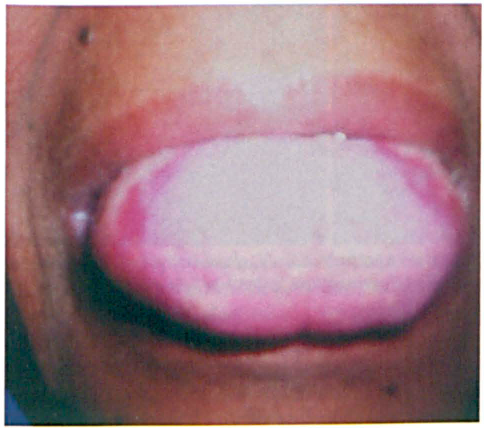
At presentation, the superficial, erosive ulcerations are seen on both sides of the tongue.
An incisional biopsy and histopathologic examination revealed a diffuse infiltration of the tongue by plasma cells with atypical nuclei (figure 2). Immunohistochemistry demonstrated light-chain restriction. The tumor cells were negative for CD20 (figure 3, A), positive for kappa light chains (figure 3, B), and slightly positive for both lambda light chains (figure 3, C) and CD38. These findings were consistent with a diagnosis of a plasma cell neoplasm.
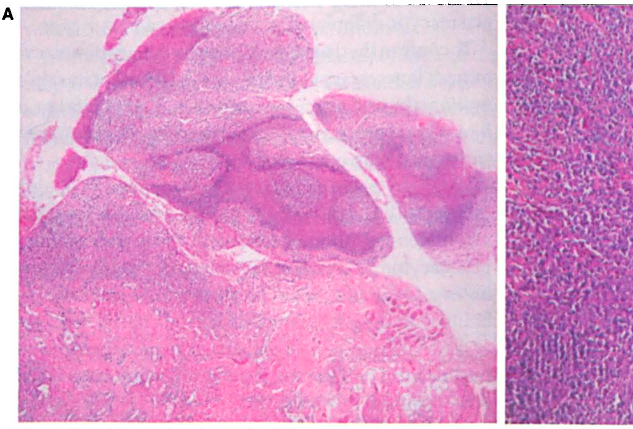
H&E staining shows the diffuse atypical plasma cell infiltration of
the subepithelial tongue mucosa at × 40 (

Findings on immunohistochemistry (original magnification × 400) are
consistent with a diagnosis of a plasma cell neoplasm. Tumor cells are
negative for CD20 (
A complete workup for systemic myeloma was carried out. The investigation included a skeletal survey, bone marrow biopsy, serum and urine protein electrophoresis, and measurements of the erythrocyte sedimentation rate and levels of β2-microglobulin, quantitative immunoglobulins, and Bence Jones proteins in the urine. Magnetic resonance imaging (MRI) and positron-emission tomography (PET) did not detect any lesion in the tongue or any lymphatic or distant metastasis.
The patient was initially treated with one cycle of chemotherapy (melphalan with prednisone), but no response was observed. Two weeks after chemotherapy, she was referred to radiation oncology. She was treated with three-dimensional conformal radiotherapy with a total dose of 50 Gy in daily fractions of 2 Gy 5 days a week for a total of 5 weeks. Since no lymph node metastasis had been found, we did not perform elective nodal irradiation. At the end of treatment, the patient exhibited acute Radiation Therapy OncologyGroup(RTOG) grade 2 mucositis with edema of the tongue and grade 1 dry desquamation of the cheeks; these conditions resolved with appropriate medication.
After 20 months of follow-up, the ulcerations on both sides of the tongue had disappeared (figure 4) and a biopsy was negative. At 54 months post-treatment, the patient showed no sign of systemic myeloma or local recurrence.

Follow-up examination 20 months after radiotherapy shows that the erosive ulcerations have disappeared.
Discussion
Plasma cell neoplasms account for approximately 1 to 2% of human malignancies, and they occur at a rate of 3.5 cases per 100,000 population per year.1,16 They may be either extramedullary or osseous. Less than 10% of patients with plasma cell neoplasms present with a solitary plasmacytoma.7,8 Liebross et al studied 1,354 patients who were treated for plasma cell neoplasms; of this group, 1,272 patients (93.9%) had multiple myeloma, 60 patients (4.4%) had a solitary plasmacytoma of bone, and only 22 patients (1.6%) had an extramedullary plasmacytoma. 17
Most patients with extramedullary plasmacytoma of the head and neck region present with local symptoms, which can include nasal obstruction, bleeding, discharge, and pain. The typical clinical sign is a well-localized submucosal mass or swelling. The extent of extramedullary plasmacytoma is often difficult to assess. In view of the limitations of physical examination, MRI and computed tomography may be useful in delineating the extent of the lesion, and PET can be helpful in demonstrating lymphatic or distant metastasis. 13 Although all these radiologic tests are useful for demonstrating a mass and local infiltration in the case of superficial lesions, MRI and PET are not always practical.
The diagnosis of plasmacytoma is based on the results of histology and immunohistochemistry. Histology demonstrates a dense, homogeneous infiltrate of plasma cells. Amyloid deposition has been seen in 15 to 38% of cases of extramedullary plasmacytoma. 18 Since reactive plasma cell infiltration has a histologically similar appearance to plasmacytoma, immunohistochemical findings are important in making the distinction.
Polyclonal kappa and lambda light-chain expression indicates a reactive process. The most common immunoglobulin expressed by the plasmacytoma tumor cells is IgG with kappa light-chain restriction. Our case revealed monotypic light-chain restriction with positive kappa light chains and slightly positive lambda light chains, indicating extramedullary plasmacytoma rather than reactive plasma cell infiltration.
Most cases of extramedullary plasmacytoma lack the pan-B-cell antigens such as CD20; conversely, in most cases, CD38 and CD79a (Ig-associated antigen) are expressed. Some cases of extramedullary plasmacytoma may represent extranodal marginal-zone B-cell lymphoma of the mucosa-associated lymphoid tissue (MALT) type with extreme plasmacytic differentiation. In this respect, CD20 negativity is a helpful feature in diagnosing extramedullary plasmacytoma, particularly in distinguishing it from B-cell lymphoma with extreme plasmacytic differentiation, as occurred in our case.
To confirm the diagnosis of extramedullary plasmacytoma, it is necessary to exclude the diagnosis of multiple myeloma by performing serum protein electrophoresis, a Bence Jones protein analysis in the urine, a bone survey, and a bone marrow biopsy.
Localized extramedullary plasmacytoma is highly radiosensitive. According to published guidelines, the recommended primary treatment for extramedullary plasmacytomas is radical radiotherapy. 19 Radiotherapy doses and portals should be chosen to minimize morbidity with the goal of obtaining local control. Because of the small numbers of patients in reported series and the low local failure rate, there is no firmly established dose-response relationship.
Tsang et al achieved local control in 13 of 14 patients (92.9%) with 35 Gy; the 1 patient in whom radiotherapy failed had a primary tumor larger than 5 cm. 20 Jyothirmayi et al achieved local control in 6 of 7 patients (85.7%) with doses of 35 to 45 Gy (median: 40) delivered in 20 fractions. 21 Holland et al also reported worse local control in patients whose tumors were larger than 5 cm, and they observed no evidence of a radiation dose-response effect over a dose range of 16 to 62 Gy (median: 46). 8
Several series reported local control in 100% of patients.2,11,15,16,21 For example, Bolek et al reported local control in all 10 patients with a median dose of 45 Gy; they recommended a dose of 40 Gy in 20 fractions. 16 Since 100% of their patients achieved local control, it is possible that local control could have been achieved with lower doses. Still, the optimal radiation dose seems to be in the range of 40 to 50 Gy.
The optimal radiotherapy target volume is similarly controversial. Extramedullary plasmacytomas arising in the upper aerodigestive system (>80% of cases) metastasize to the cervical lymph nodes in 10 to 40% of cases.1,11,17 The inclusion of draining cervical nodes in the radiation fields significantly adds to acute and late morbidity, especially xerostomia, which may not fully resolve. However, excellent local control has been reported when the cervical nodes were electively included. 16 On the other hand, similarly good results were reported in series in which the cervical nodes were included only if clinically involved. 20
Since there is a negligible risk (≤4%) of regional failure, it is not recommended that the regional lymphatics be treated electively.6,19 Because our patient had no apparent lymph node metastasis, we did not irradiate the regional lymphatics, and she experienced good local control without any late toxicity such as xerostomia.
In conclusion, extramedullary plasmacytoma of the tongue is rare. It maybe misdiagnosed as either a benign reactive process or a lymphoma. Awareness of this entity may help prevent misdiagnosis and avoid its progression to multiple myeloma and consequent loss of curability. In our patient, irradiation to the primary site achieved local control without causing significant morbidity.