
Abstract
A lingual thyroid is a mass of ectopic thyroid tissue located in the midline of the base of the tongue. Its estimated prevalence ranges from 1 in 3,000 to 1 in 10,000 population. We report the interesting case of a 28-year-old woman who presented with a primary papillary carcinoma in a lingual thyroid and a histologically normal thyroid gland. To the best of our knowledge, this case probably represents only the second reported case of a follicular variant of a papillary carcinoma arising in a lingual thyroid.
Introduction
Lingual thyroid is the term applied to a mass of ectopic thyroid tissue that is located in the base of the tongue at the midline. Its prevalence is variably estimated at 1 in 3,000 to 1 in 10,000 population. 1 The primary thyroid tissue is absent in 70% of cases. 2 Lingual thyroids usually contain histologically normal tissue; reports of a carcinoma arising within this form of ectopic thyroid are rare. In this article, we report an extremely rare case of a follicular variant of a papillary carcinoma arising in a lingual thyroid.
Case Report
A 28-year-old woman presented to our outpatient unit with a complaint of blood-tinged saliva for the previous 2 weeks. She said that she had experienced a similar episode 3 years earlier; the previous episode had lasted 3 days and subsided without any treatment. She also reported that she had felt a lump in her throat for the previous 2 weeks. She had no associated dysphagia or dyspnea, and no other relevant history.
A general physical examination revealed no abnormalities. However, the oropharyngeal examination revealed the presence of a globular, fleshy, 2-cm mass arising from the midline on the base of the tongue. On intraoral palpation, the mass was limited to the oropharynx without supraglottic extension. The mass was firm and sensitive to touch, but it did not bleed on touch. No other swelling was found in the upper aerodigestive tract.
External examination of the neck revealed bilateral 0.5 × 1.0-cm level IB nodes that were nontender, mobile, and firm. On further palpation, a firm, nontender, solitary, 1,0 × 1.0-cm nodule was found in the superior pole of the left thyroid lobe. This mass moved with deglutition but not with protrusion of the tongue.
Findings on computed tomography (CT) of the oropharynx were suggestive of a vascular malformation (figure). The mass measured 2.5 × 2.3 × 3.6 cm. Fine-needle aspiration cytology (FNAC) of the oropharyngeal mass revealed only blood and skeletal muscle bundles, which suggested a hemangioma of the tongue base. FNAC of the solitary thyroid mass demonstrated evidence of colloid changes in the nodule.
Laboratory testing revealed a total triiodothyronine (T3) level of 104 ng/dl, a total thyroxine (T4) level of 6.3 μg/dl, and a thyroid-stimulating hormone (TSH) level of 2.09 mIU/L, all of which were within the normal reference range. The patient's hemoglobin concentration was low at 10.2 g/dl, and she therefore received a transfusion of 3 units of O-positive, cross-matched whole blood.
Following preoperative preparation, the lesion was excised via a median pharyngotomy approach. Complete exposure of the tongue base was achieved by entering the pre-epiglottic space and vallecula. Intraoperatively, the globular vascular mass was found to be arising from the left side of the tongue base on a stalk. The pedicled fleshy mass extended anteriorly up to the circumvallate line; posteriorly, it stopped short of the vallecula and crossed the midline to the right. The mass was removed in toto, and a wedge excision of the tongue base was made. The patient's recovery was uneventful, and she was discharged on postoperative day 7.
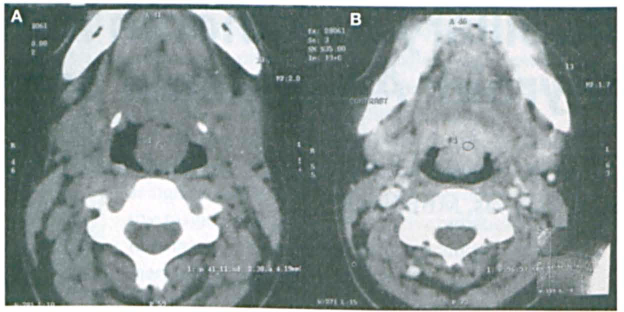
The pedunculated lingual mass is seen on pre- (
On histopathology, we were surprised to learn that the specimen contained ulcerated squamous epithelium with underlying infiltrating thyroid papillary tumor cells within the lingual thyroid. On repeat sectioning and microscopic evaluation by experienced pathologists, the lesion was confirmed as the follicular variant of papillary thyroid cancer within a lingual thyroid.
In light of the pathology findings, the patient was counseled on the need for thyroid surgery. Within 15 days of the first surgery, she underwent a total thyroidectomy with central neck node clearance. Intraoperatively, nodular tissues were found in the superior pole of the left lobe and the inferior pole of the right lobe. Her postoperative recovery was aided by levothyroxine and calcium supplementation. The cervical thyroid specimen showed no histologic evidence of papillary carcinoma, and it was reported as benign, even after multiplanar sections were studied.
The patient underwent a whole-body radioiodine scan, and she was discharged with advice for regular follow-up every 3 months with clinical evaluation, thyroglobulin assays, and nuclear scintigraphy. Three years later, the patient was asymptomatic and disease-free.
Discussion
The origin of a lingual thyroid is the result of a failure of the thyroid primordium to descend into the neck. As a consequence, a focus of thyroid tissue remains at the foramen cecum. Sometimes a lingual thyroid is the only functioning thyroid tissue in the body. On the other hand, an overdescent of the thyroid primordium can result in the formation of ectopic thyroid tissue in the mediastinal area or even within the cardiac endothelium. 3
Lingual thyroid tissue has been well documented by many independent reports in the literature.1,4,5 These reports include a series of 4 cases in our city of Mangalore, India. 1 Lingual thyroid is known to present as an asymptomatic, smooth-surfaced lump in the midline of the posterior one-third of the tongue between the sulcus terminalis and the epiglottis. In most cases it is detected incidentally on radioiodine scanning, or it presents with dysphagia or airway compromise in infancy or childhood.6,7 In rare cases it presents with acute bleeding.
Our patient presented with chief complaints of blood-tinged saliva and a feeling of a lump in the throat. She had not experienced any dysphagia or dyspnea, even though the size of her lingual thyroid on CT was measured as 2.5 × 2.3 × 3.6 cm. The most logical explanation for her clinical picture is that the attachment of the mass by a pedicle made it more susceptible to bleeding and that the mass's overt mobility might not have caused any static obstruction significant enough to cause dysphagia.
Lingual thyroid tissue is known to be associated with an absence of cervical thyroid tissue in 70% of patients. 2 It has also been reported that hypothyroidism is more common than hyperthyroidism in patients with a lingual thyroid as a consequence of the failure of the lateral lobes to fuse to the median lobes, which results in an insufficient number of cells being made available to adequately produce thyroid hormones. 8 However our patient had a fully developed thyroid gland in the euthyroid state.
Standard CT has been found to adequately demonstrate a lingual thyroid in the oropharynx. However, the lesion in our patient was mistakenly believed to be a vascular malformation because the precontrast scan showed a homogeneous, well-defined soft-tissue attenuation of 40 Hounsfield units (HU) with intense postcontrast enhancement of 80 to 100 HU.
In light of the fact that our patient presented with a bleeding mass in the base of the tongue, a conventional diagnosis of a malignancy or a benign lesion such as a hemangioma was suggested. The intraoral FNAC had failed to reveal any definitive diagnosis. Therefore, surgical exploration was planned, with adequate precautions being taken for airway and hemodynamic support.
In our group's limited experience with lingual thyroid (5 cases), the present case is the first that involved a carcinoma. Our review of the literature found fewer than 50 cases of a malignant change in an ectopic lingual thyroid, with follicular cancer being the dominant variety.9–14 In only 5 of these reported cases11–15 did the patient develop papillary cancer, and in only 1 case 15 was it the follicular variant of papillary carcinoma. To the best of our knowledge, our case is probably only the second reported case of the follicular variant of a papillary carcinoma arising in a lingual thyroid.
Patients with a lingual thyroid and a nonfunctioning primary thyroid can be treated with levothyroxine to keep their TSH level between 0.2 and 0.6 mIU/L, which should result in shrinkage of the tissue and a return of. general health to normal. When a lingual mass does not shrink or when it bleeds or becomes ulcerated, a biopsy is advisable. In the event that ectopic thyroid tissue harbors a malignancy, surgery at the base of the tongue followed by a total thyroidectomy is advisable, provided that the cervical thyroid gland is present on preoperative ultrasonography.
In terms of the surgical approach to a lingual tumor, an oral, lateral cervical, or even a transhyoid incision may be best. A temporary tracheotomy may be advisable in anticipation of postoperative edema in the base of the tongue and upper pharynx. In cases of advanced and invasive cancer, substantial damage to the tongue can be expected.
Following surgical clearance, radioiodine scanning is necessary; iodine-131 ablation should be performed only when the pathologic characteristics so demand. The patient should then receive adequate doses of lifelong levothyroxine and should be followed for intrathyroidal cancer by scanning and serial assays of thyroglobulin.
In conclusion, we emphasize the importance of thoroughly investigating all patients who present with a midline tongue swelling. The diagnosis of a malignant lingual thyroid may be easily missed, as it initially was in our patient.