
Abstract
We conducted a study to validate the expression of PLUNC (palate, lung, and nasal epithelial clone) protein in nasal polyp and chronic sinusitis tissue by immunohistochemistry. We also explored the relationship between the intensity of positive immunohistochemical staining for PLUNC protein and postoperative therapeutic efficacy. Our study population consisted of 34 patients with nasal polyps and 30 with chronic sinusitis who had undergone surgical treatment, along with 18 healthy controls who did not undergo surgery. All samples were stained according to the streptavidin-peroxidase immunohistochemical method to examine PLUNC protein expression. The surgical patients were evaluated for clinical therapeutic efficacy 6 months postoperatively. The association between efficacy and the intensity of PLUNC protein positivity was examined by the Spearman rank correlation analysis. Intensity was rated as either +++ (>50% positive cells), ++ (26 to 50% positive cells), + (≤25% positive cells), or - (no positive cells). We found that the most common levels of PLUNC positivity were + in the patients with nasalpolyps, +++ in the patients with chronic sinusitis, and ++ in the controls (p < 0.01). Analysis of the Spearman rank correlation indicated that the intensity of PLUNC protein expression was significantly correlated with postoperative therapeutic efficacy (p < 0.001). We conclude that PLUNC protein is an essential factor in the innate defense mechanism of the nasal mucosa. The immunohistochemical staining of PLUNC protein could have clinical benefit in terms of predicting therapeutic efficacy and outcomes in patients with nasalpolyps or chronic sinusitis.
Introduction
From 2004 to 2006, we performed pH 3-10 and pH 4-7 gradient two-dimensional electrophoresis (2-DE) on tissue samples of nasal polyps, chronic sinusitis, and normal nasal mucosa. We found that some proteins were differentially expressed in these tissues. In pH 4-7 gradient 2-DE, various antimicrobial proteins—including PLUNC (palate, lung, and nasal epithelial clone), SOD, NKEF-B, PACAP, glutathione S-transferase pi, and DJ-1 proteins—were highly expressed in chronic sinusitis but expressed at low levels in nasal polyps. 1
We selected the novel secretory PLUNC protein for immunohistochemical analysis in paraffin-embedded tissue samples to validate the differential expression among nasal polyps, chronic sinusitis, and normal nasal mucosal tissue, and to observe the localization of its expression in tissues and cells. The protein must be validated repeatedly to ensure reliable and stable results. Furthermore, proteins showing differential expression only correlated with clinical therapeutic efficacy may be of clinical value.
Patients and Methods
We conducted ongoing follow-up observations of 64 patients who had undergone functional endoscopic sinus surgery to treat either nasal polyps (n = 34) or chronic sinusitis (n = 30). The 34 patients with nasal polyps included 19 men and 15 women, aged 18 to 54 years (mean: 40), and the 30 patients with chronic sinusitis included 16 men and 14 women, aged 22 to 58 years (mean: 41).
Paraffin-embedded tissue samples were obtained from the 34 patients who had had nasal polyps and the 30 patients who had had chronic sinusitis, as well as from the nasal mucosa of 18 normal controls; the control group was made up of 10 men and 8 women, aged 16 to 30 years (mean: 21). The nasal polyp and sinusitis tissues were obtained from the ethmoid sinus in the 64 patients. For control purposes, normal mucosal tissue was obtained from the middle turbinates of patients with a simple deviated nasal septum. The nasal polyp tissue was clearly different from the chronic sinusitis tissue as seen during the preoperative nasal endoscopic examination, on computed tomography (CT), and at the final pathologic diagnosis.
None of the patients had allergic rhinitis, aspirin intolerance triad, asthma, or ciliary dyskinesia, and none had used a corticosteroid or antibiotic during the 2 weeks before their operation. All of the samples had been confirmed as nasal polyps, chronic sinusitis, or normal nasal mucosa by pathologic diagnosis.
To ascertain the intensity of PLUNC protein expression, we cut the paraffin-embedded tissue blocks into 4-μm-thick sections, which were then deparaffinized, dehydrated through a graded alcohol series, rehydrated, and subjected to antigen recovery by autoclaving. All samples were then stained using the streptavidin-peroxidase immunohistochemical method (Maxim Biotech; Rockville, Md.).
After nonspecific binding sites were blocked with 0.3% H2O2 in methanol for 30 minutes, the sections were incubated with normal nonimmune serum for 1 hour. The sections were then incubated for 30 minutes with goat polyclonal antibody against PLUNC protein (1:200 dilution; R&D Systems, Minneapolis), followed by a biotin-conjugated secondary antibody (Maxim Biotech) for 10 minutes. The sections were then colorized with diaminobenzidine/hydrogen peroxide and counterstained with Harris modified hematoxylin. For control analyses, the primary antibody was replaced by phosphate-buffered saline. Finally, the sections were examined under a BX60 microscope (Olympus; Tokyo).
The intensity of PLUNC protein positivity was rated as either +++ (>50% positive cells), ++ (26 to 50% positive cells), + (≤25% positive cells), or - (no positive cells). Statistical analyses were performed using the chi-square (χ 2 ) test with the Statistical Package for the Social Sciences software (v. 10.0; SPSS; Chicago).
At 6 months postoperatively, the 64 patients were evaluated for therapeutic efficacy according to criteria that are generally accepted as objective and realistic in China. Therapeutic efficacy was classified into two categories, recurrence and no recurrence, which were defined thus:
Recurrence: Patients had undergone no less than two functional endoscopic sinus surgeries or symptoms were not relieved; the nasal mucosa showed adherence; the paranasal sinus ostia showed stenosis or atresia; nasal polyps recurred with purulent secretions as determined by nasal endoscopy.
No recurrence: Symptoms resolved or decreased; the paranasal sinus ostia were open; epithelialization of the nasal mucosa occurred with little or no purulent secretions as determined by nasal endoscopy.
Next, we examined the correlation between clinical efficacy and the intensity of immunohistochemical positivity for PLUNC protein using the Spearman rank correlation analysis.
Our study protocol was approved by ethics committee of the Xiangya Hospital of Central South University in Changsha, China.
Results
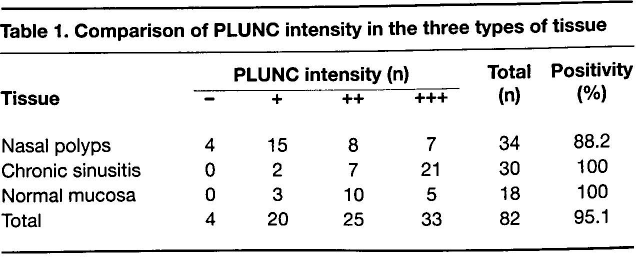
Immunohistochemistry revealed that the PLUNC-positive cells were mainly expressed in nasal mucosa epithelium, in goblet cells, and especially in glandular epithelium. In addition, these cells exhibited a brown color in the cytoplasm and glandular organ lumina. The most common levels of intensity of PLUNC protein expression were + in the nasal polyp samples, +++ in the chronic sinusitis samples, and ++ in the normal nasal mucosal tissue (figure, table 1). The differences in the degree of positivity of PLUNC protein expression among the three kinds of tissue were statistically significant (χ 2 = 28.834; p < 0.01).
Comparison of PLUNC intensity in the three types of tissue
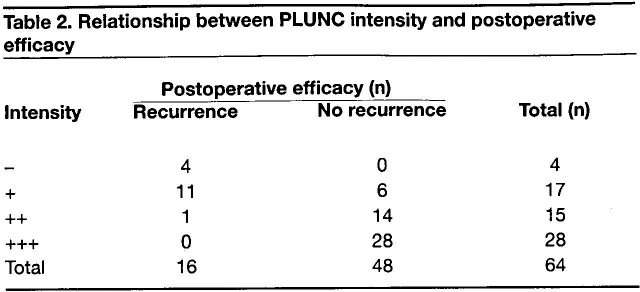
Analysis of the Spearman rank correlation indicated that the intensity of PLUNC protein expression was significantly correlated with postoperative therapeutic efficacy (correlation coefficient = 0.702; p < 0.001 [2-tailed]). Patients whose intensity of PLUNC protein positivity was +++ or ++ were categorized in the no recurrence group, while those whose PLUNC protein intensity was + or - were categorized in the recurrence group (table 2).
Relationship between PLUNC intensity and postoperative efficacy
Discussion
Using pH 4-7 gradient 2-DE, we found that the novel secretory protein PLUNC is differentially expressed among nasal polyps, chronic sinusitis, and normal nasal mucosal tissue. PLUNC protein, which is encoded by a gene on chromosome 20, is expressed in regions of the mouth, nose, and lung.2–4 Ghafouri et al demonstrated that of all the proteins present in human nasal lavage fluid, only PLUNC protein was adsorbed onto a lipopolysaccharide-coated surface, which is central to host defenses against gram-negative bacteria. 5
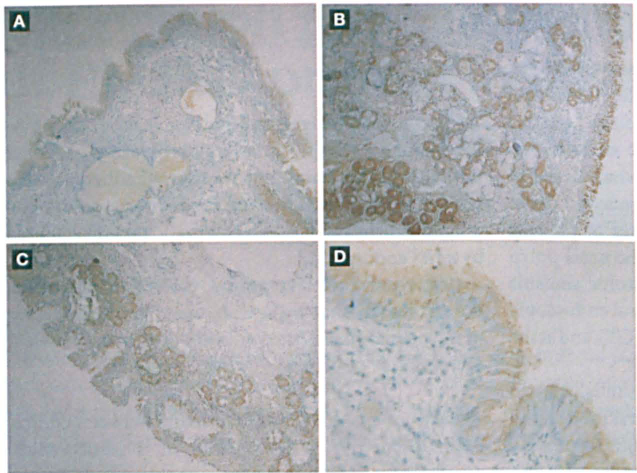
Immunohistochemistry (original magnification × 100) shows that the
intensity of PLUNC protein expression is primarily + in the nasal
polyp samples (
Sung et al detected upregulation of PLUNC protein expression after bulbectomy in the respiratory epithelium and suggested that PLUNC protein may provide protection against infection after injury. 6 Bingle and Gorr suggested that PLUNC protein may play a role in the innate immune response of the upper airways. 7
In our study, both proteomics and immunohistochemical analyses indicated that the highest levels of PLUNC protein expression occurred in chronic sinusitis and the lowest levels in nasal polyps. Our immunohistochemical analyses demonstrated that PLUNC-positive cells were mainly present in nasal mucosal epithelium, in goblet cells, and particularly in glandular epithelium. In addition, PLUNC-positive cells showed a brown color in the cytoplasm and glandular organ lumina, confirming that it is a secretory protein.8,9 These observations suggest that in response to irritation by infectious agents or chemical factors, the nasal mucosal epithelium, goblet cells, and glandular epithelium will proliferate reactively and produce anti-inflammatory agents, including PLUNC protein, as a defense against the irritant.
Recent studies have detected the expression of antimicrobial proteins—such as lysozymes, lactoferrin, secretory IgA, defensins, and Toll-like receptors—in the respiratory mucosal epithelium, goblet cells, and glandular epithelium. These molecules are important components of the respiratory mucosal immune defense system, as well as the respiratory mucus cilia transmission system.10–16 On irritation of the respiratory mucosa by infectious agents or chemical factors, production of such anti-inflammatory agents are upregulated as a defense mechanism. This indicates that inflammation is essentially a defensive reaction against irritants. PLUNC protein is also an important component of the innate defense system of the nasal mucosa. In cases of congenital defects or destruction of the immune defense function of the respiratory mucosa, inflammation would fall into a vicious circle, and nasal polyps may easily recur.
In our study of 64 patients who had undergone functional endoscopic sinus surgery to treat nasal polyps or chronic sinusitis, statistical analysis indicated that the intensity of PLUNC protein expression was significantly correlated with postoperative therapeutic efficacy (p < 0.001). Our results suggest, therefore, that the immunohistochemical staining of PLUNC protein could have clinical benefit for predicting prognosis and therapeutic efficacy in patients with chronic sinusitis and nasal polyps.
Therapeutic efficacy is generally accepted to be poorer in patients with nasal polyps or chronic sinusitis whose affected tissue contains large numbers of eosinophils and elevated levels of leukotrienes and IgE. In our study, we found that therapeutic efficacy was poorer in patients whose levels of PLUNC protein in affected tissue were lower. Therefore, it stands to reason that these objective indices can be used to determine prognosis and therapeutic efficacy. Certainly our findings should encourage further study of larger samples. For our own future studies, we will use high-throughput experimental techniques such as proteomics and microarray analyses to identify additional objective indices for quantitatively monitoring the progression of disease states and responses to therapy.