
Abstract

Extramedullary involvement of recurrent pre-B-cell acute lymphoblastic leukemia (ALL) is a rare entity seen only in a handful of cases reported during the past several decades. Since this form of recurrent leukemia of the middle ear is rare and the clinical manifestations can mimic acute otitis media and Bell palsy, it may not be readily recognized.1–4
A 4-year-old boy with a history of pre-B-cell ALL, status post-chemotherapy, presented with left-sided Bell palsy that improved with acyclovir and prednisone. A month later, after an additional round of chemotherapy, the Bell palsy worsened. A concomitant middle ear effusion resistant to antibiotic therapy was treated with tympanostomy tubes to no avail. Initial computed tomography (CT) imaging of the left temporal bone was consistent with chronic otomastoiditis (figure). Subsequent biopsy of the middle ear exudate proved pre-B-cell ALL recurrence, consistent with a granulocytic sarcoma.
Acute lymphoblastic leukemia is a bimodal malignancy, characterized by excess lymphblasts, that occurs in children predominantly 2 to 5 years of age, with a second peak in incidence in the elderly population. Extramedullary recurrence localized to the middle ear is rare and can present in the form of a granulocytic sarcoma also known as a chloroma, a solid tumor of immature granulocytes. 1 Clinical manifestations of such include otitis media and Bell palsy.
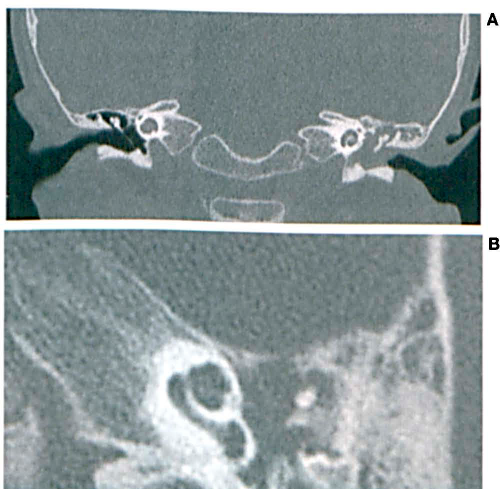
Coronal plane of both temporal bones (
The earliest case of acute leukemia presenting as acute otitis media was reported in 1956. 5 In 1984, the first case of a patient diagnosed with leukemia presenting with atypical otomastoiditis and facial paralysis due to an underlying granulocytic sarcoma was reported. 4 Complete remission and complete recovery of facial nerve function were achieved with localized radiation and systemic chemotherapy. 4 Only 4 other such cases have been reported since then—in 1990, 1993, 1996, and 2010.1,3,6,7
Before 1990, physicians relied on surgical excision or autopsy to diagnose leukemia of the middle ear. Less invasive diagnostic methods were encouraged after 1990. Dr. Maguchi urged readers in 1990 to consider shifting to histologic and cytologic evaluation of the tympanic exudate to clench the diagnosis of leukemic involvement of the middle ear after successfully diagnosing 2 patients. 2
External ear canal skin lesions, red or thick tympanic membrane, middle ear effusions, otitis media, hearing loss, and mastoiditis have been linked to underlying leukemia infiltrating the temporal bone. 7