
Abstract
Streptococcus milleri infections and abscesses in the head and neck region have been previously reported, but there is still a dearth of clinical literature on this topic. To add to the available reports and to promote a better understanding and awareness of this clinically important entity, we present this retrospective review of 7 cases of head and neck abscess caused by S milleri infection. We have placed particular emphasis on antibiotic sensitivity patterns. These patients—6 men and 1 woman, aged 28 to 73 years (mean: 42.7)—had been seen at a district general hospital in Gosford, Australia, over a 6-month period. All patients had undergone surgical intervention and had been treated with intravenous antibiotics. All the S milleri cultures were sensitive to penicillin G, cephalexin, and erythromycin. Six of these patients experienced a resolution of their abscess, while 1 patient died from overwhelmingsepsis. We believe that the initiation of penicillin G, cephalexin, or erythromycin is a good starting point for empiric therapy. S milleri should be considered as a causative organism in a patient who presents with a head and neck abscess, especially in the presence of a dental infection. Such a patient should be monitored closely for airway obstruction and distal infective sequelae. Also in this article, we compare our findings with those reported in two other published series.
Introduction
Streptococcus milleri comprises a group of three distinct gram-positive species: Streptococcus intermedius, Streptococcus constellatus, and Streptococcus anginosus. The identification and classification of this group of bacteria have been historically complicated, and hence recognition of S milleri infections may be under-reported. 1
Guthof coined the term Streptococcus milleri in 1956 to describe nonhemolytic streptococci that were isolated from oral infections; his intention was to honor oral microbiologist W.D. Miller (1853–1907). 2 S milleri is a common commensal organism found in the oral cavity, gingival crevices, dental plaque, dental root canals, throat, oropharynx, gastrointestinal tract, appendix, stool, and the vaginal canal. 3
S milleri is well known for its ability to cause purulent infections and abscesses at various sites in the body Infections caused by this organism usually occur in the abdominal/hepatobiliary system and in the thoracic cavity, while abscesses usually occur in the liver, abdomen, pelvis, lung, and brain. 4
A number of cases of S milleri infections and abscesses of the head and neck region have been previously reported, but there is still a dearth of clinical literature about these pathologies. Han and Kerschner 5 in Milwaukee published a series of 26 cases in 2001, and Hirai et al 6 in Hiroshima reviewed 17 cases in 2005. We describe a small series of patients with an abscess of the head and neck caused by S milleri infection, and we pay particular attention to antibiotic sensitivities in comparison with the two previous case series. It is our wish to add to the available literature and to promote a better understanding and awareness of this clinically important entity.
Patients and methods
We retrospectively reviewed 7 cases of head and neck abscess secondary to S milleri infection that had been treated over a 6-month period in the Department of Otolaryngology at Gosford Hospital in New South Wales, Australia. The 7 patients included 6 men and 1 woman, aged 28 to 73 years (mean: 42.7).
In addition to demographic data, we compiled information on the site of the abscess, comorbidities, the clinical presentation and treatment, outcomes, and inpatient and discharge antibiotic regimens. We also paid particular attention to culture sensitivity patterns. Pus cultured from each of the 7 patients had grown S milleri. Identification of the causative pathogen had been made by the hospital's microbiology service. (At Gosford Hospital microbiologic cultures are reported only as S milleri; they are not further subclassified as either S intermedius, S constellatus, or S anginosus.)
Once our data were complied, we compared our findings with those of Han and Kerschner 5 (the Milwaukee group) and Hirai et al 6 (the Hiroshima group), keeping in mind that our study included only abscesses, while the other two studies included both S milleri infections and abscesses.
Results
Our findings are summarized in table 1, and a comparison of our findings with those of the Milwaukee group and the Hiroshima group is shown in table 2.
Selected characteristics of the 7 patients

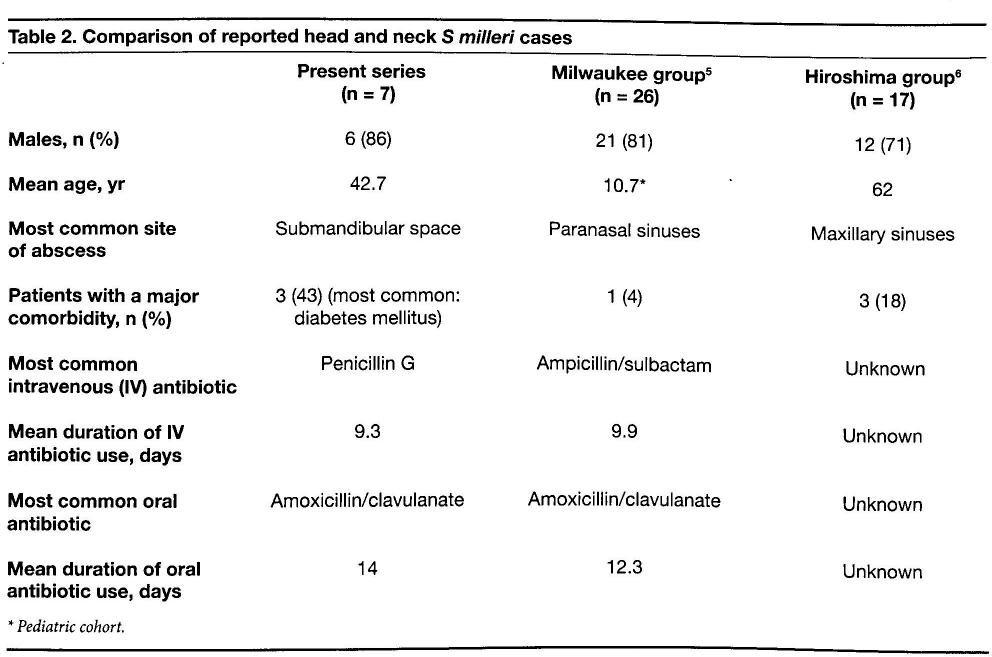
Comparison of reported head and neck S milleri cases
Pediatric cohort.
Sex and Age
The male preponderance in our population (86%) was similar to the proportions of both the Milwaukee group and the Hiroshima group—81 and 71%, respectively. Incidentally, in a review of 28 cases of S milleri infection throughout the body, Shlaes et al also found a striking predisposition for males (6:1). 7
With respect to age, our group was obviously older than the pediatric cohort in the Milwaukee group, and it was generally similar to the Hiroshima group.
Site of Abscess
The most common site of abscess in our series was the submandibular space, wherein 5 of 7 cases (71%) were located. This is in contrast to both the Milwaukee and Hiroshima groups, where sinus involvement was most common (the paranasal and maxillary sinuses, respectively.) On the other hand, our finding is compatible with that of an Italian review of 24 deep neck space infections, which found that 67% of the abscesses studied occurred in the submandibular space. 8 It is interesting that in the Italian study, the most common organism isolated from those abscesses was S milleri, which accounted for half of the total.
Comorbidities
Three of the 7 patients in our study (43%) had at least one major comorbidity, the most common being diabetes mellitus. In the Milwaukee group, only 1 of the 26 patients (4%) had a major comorbidity (cystic fibrosis), but this is not surprising considering that this group represented a purely pediatric population. In the Hiroshima group, a major comorbidity was documented in 3 of the 17 patients (18%); there was 1 case each of diabetes mellitus, human immunodeficiency virus infection, and heart failure.
Treatment
All of our patients required surgical intervention and treatment with at least one intravenous antibiotic. Overall, our patients were treated successfully and relatively easily, even though nearly all of them exhibited signs of systemic sepsis on presentation. The exception was patient 5, who died as a direct result of overwhelming S milleri sepsis from his head and neck abscess. A similar death from sepsis in a patient with S milleri head and neck infection was reported in Wales by Flanagan and Mills in 1994. 9 In their case, the deceased patient was a previously healthy adult, whereas our patient had coexisting diabetes mellitus. Jacobs et al reported a series of predominately intra-abdominal S milleri infections in which the mortality rate reached 22%. 10
Outcomes
Only 1 of the 6 survivors (patient 7) had a difficult course once treatment was initiated. The others were hospitalized for less than 1 week.
Length of Stay
The mean length of hospital stay in our series was 8 days. This excluded 1 case in which the patient self-discharged against medical advice on day 3, and the 1 death, which occurred on day 22.
Sensitivity Patterns
The S milleri cultured from our patients exhibited universally identical sensitivity patterns, as all the isolates were sensitive to penicillin G, cephalexin, and erythromycin. By contrast, the Milwaukee study found a slight decline in the sensitivity of S milleri to penicillin over the 3-year period from 1996 to 1999, and a much greater decline in sensitivity to erythromycin (from 97 to 84%) over the same 3 years. In the Hiroshima group, only 71% of cases were sensitive to ampicillin, but 100% were sensitive to second-, third-, and fourth-generation cephalosporins. These differences illustrate the regional variations in antibiotic sensitivities in S milleri. In our series, cultures of 4 of the 7 patients (57%) grew organisms other than S milleri; corresponding figures in the Milwaukee and Hiroshima groups were 31 and 53%. In the pediatric (Milwaukee) group, these concomitantly cultured organisms included Aspergillus fumigatus, Eikenella corrodens, Haemophilus influenzae, Peptostreptococcus spp, Proteus mirabilis, Pseudomonas aeruginosa, Staphylococcus aureus, Staphylococcus epidermidis, and Streptococcus pneumoniae. In the adult (Hiroshima) group, they included anaerobes, Fusobacterium spp, Haemophilus spp, methicillin-susceptible S aureus, Peptostreptococcus spp, and Prevotella spp. Our series shows a similar incidence of concomitantly cultured organisms in an adult population.
Discussion
In many ways, our findings were similar to those of the Milwaukee 5 and Hiroshima studies. 6 A notable exception was the difference in antibiotic sensitivity patterns, which are presumably influenced by local antibiotic prescribing practices and environmental factors.
S milleri has several properties that make it so pathogenic. It appears to induce less chemotaxis of polymorphonuclear leukocytes than does S aureus, a common abscess-forming pathogen, 11 and this allows S milleri more time to proliferate prior to phagocytosis. It also appears that it takes leukocytes more time to kill S milleri once they have been phagocytosed, the rate of killing by leukocytes being substantially slower than the rate of killing of S aureus. 11
S milleri possesses several other cell-surface characteristics that may promote the formation of abscesses, including the production of hyaluronidase. Hyaluronic acid is a major component of the interstitial barrier, and its hydrolysis by hyaluronidase increases the permeability of tissues. 12
One of the three S milleri subtypes, S intermedius, has been shown to produce a human-specific cytolysin called intermedilysin. Intermedilysin is known to lyse cells of the human immune system, including neutrophils. The presence of S intermedius in sites of deep infection correlates with an increase in the production of this cytolysin. Moreover, S intermedius cultured from dental plaque has also exhibited this increased production. 13
In vitro studies of S milleri have found a gliding type of motility across surfaces with the production of an extracellular material. This is thought to aid movement in the apparent absence of traditional organs of motility such as flagella. 14 It has been proposed that this may aid in the spread of infective organisms in vivo.
The pathogenicity of S milleri is enhanced by its ability to spread hematogenously. 15 In our series, patient 5 developed infective endocarditis several days after his admission. The ability of S milleri to spread hematogenously, to bind fibronectin, and to cause aggregation of platelets and then be incorporated into clots has been widely implicated in the development of endocarditis. In some studies, 9 to 15% of cases of community-acquired endocarditis have been reported to be caused by S milleri. 16
In view of the potential for hematogenous spread of S milleri in the head and neck region, prompt and definitive treatment is vital in order to prevent intracranial sepsis. S milleri is the most common organism isolated from sinus-disease–related intracranial sepsis. 12 Another reason for prompt treatment is the space-occupying nature of some head and neck abscesses, which can rapidly lead to airway compromise, as occurred in patient 5 and patient 7 (figure) in our series.
In conclusion, S milleri should be considered as a causative organism in a patient who presents with a head/neck abscess, especially in the presence of poor dental hygiene. The possibility of rapid deterioration, airway compromise, and involvement of anatomically distant organs must be kept in mind. Individual antibiotic sensitivities should be sought as soon as possible, but empiric antibiotic therapy with penicillin or a cephalosporin appears to be very appropriate, at least in Australia. The presence of a co-organism should also be borne in mind.
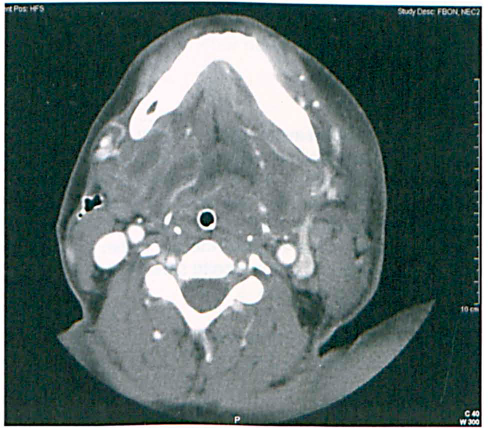
Patient 7. Contrast-enhanced computed tomography shows the abscess in the right submandibular space. This has resulted in extensive edema of the upper aerodigestive tract and complete constriction of the airway around the endotracheal tube. Edema is seen in the contralateral tissues in the neck. Note the presence of a postoperative drain on the right side.
Footnotes
Acknowledgments
We thank Dr. Rosemary Stratford of the Emergency Department at Gosford Hospital and Mr. Julian Savage of the ENT Department at Southmead Hospital in Bristol, U.K.