
Abstract
Nasal bleeding is a common disorder in children that is frequently caused by irritation in the Kiesselbach plexus (also known as Little's area). Other common underlying causes include local inflammatory diseases of the nose, infections, vascular malformations, and trauma. We report here a rare case of an ectopic tooth in the nasal cavity as the cause of recurrent epistaxis in a 3.5-year-old child. The clinical presentation, investigations, and management are discussed.
Introduction
An ectopic or supernumerary tooth in the nasal cavity is a rare phenomenon. It can be asymptomatic or may present with a myriad of symptoms, including nasal obstruction, headache, and recurrent sinusitis. Rarely, it presents with recurrent epistaxis as the only symptom. Such cases are usually associated with abnormal dentition.
An ectopic tooth in the nasal cavity can be caused by obstruction at the time of tooth eruption, or it may be associated with cleft palate. Computed tomography (CT) and panoramic radiographs confirm the diagnosis. Endoscopic excision of the intranasal tooth is the treatment of choice.
Case report
A 3.5-year-old boy presented as an outpatient at the ENT and Head and Neck Surgery Department, Post Graduate Institute of Medical Education and Research, with a history of intermittent nasal bleeding from the right nasal cavity of 2 years’ duration. The bleeding was spontaneous, with a frequency of 2 to 3 episodes every month, and was mild to moderate in amount. The patient also complained of right-sided nasal obstruction and occasional mucopurulent discharge from the right nasal cavity. There was no history of blood transfusion or nasal packing, nor a history suggestive of a bleeding disorder. The child had undergone cleft lip and palate repair 3 years earlier. His general physical examination was unremarkable.
Anterior rhinoscopy revealed purulent discharge in the floor of the right nasal cavity with a thickened nasal vestibule. A heap of granulation tissue was seen at the junction of the floor of the nasal cavity and nasal septum. Overcrowding of teeth was seen, and the right canine tooth was absent (figure 1). The palate was high arched, and the palatal scar was healthy.

Photo snows the abnormal dentition with the absent canine tooth (arrow).
A diagnosis of foreign body was suspected, but nasal suction and probing revealed no foreign body. Contrast-enhanced CT of the nose and paranasal sinuses revealed a dense radiopaque shadow in the floor of the nasal cavity (figure 2). A routine blood investigation was done and was normal. Hemoglobin was 11.4 g/dl, bleeding time was 5 minutes, clotting time was 4 minutes, and the prothrombin index was 100%.
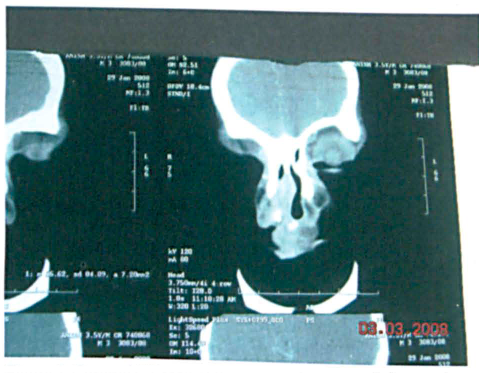
Coronal CT scan of the nose and paranasal sinuses shows a dense radiopaque shadow in the floor of the nasal cavity.
The patient was taken to surgery for nasal endoscopy under general anesthesia. On endoscopy, a heap of granulation tissue was seen overlying the impacted tooth projecting from the floor of the right nasal cavity. The ectopic tooth was removed along with the granulation tissue and sent for histopathologic examination, which confirmed the diagnosis.
The patient was on regular follow-up. At the last follow-up visit, he was asymptomatic and had experienced no further episodes of epistaxis.
Discussion
A tooth occurring in the nasal cavity is an unusual phenomenon that rarely may cause recurrent epistaxis in a child, as seen in our case. In general, the incidence of supernumerary teeth ranges from 0.1% to 1% in the general population. 1 The most commonly affected location is the upper central incisor area. 2 Ectopic teeth are commonly seen in the palate and maxillary sinus, but cases also have been reported at unusual sites such as the mandibular condyle, coronoid process, orbit, and nasal cavity. 3 Rarely, they have also been reported at the anterior mediastinum, sacral region, ovaries, and testes.1,4,5 Extra teeth usually have an abnormal appearance and may be in a vertical, horizontal, or inverted position.
The mechanism of eruption of ectopic teeth has been poorly understood. One theory is that there is a defect in the migration of neural crest derivatives destined to reach the jawbones. 5 A more plausible theory is multistep epithelial and mesenchymal interaction. 6
A supernumerary tooth in the nasal cavity could result from obstruction at the time of tooth eruption because of crowded dentition, persistent deciduous teeth, trauma, a developmental disturbance such as cleft palate, or a genetic predisposition.1,7,8
A supernumerary tooth in the nasal cavity sometimes may be asymptomatic and may be seen accidentally as a dense radiopaque shadow on radiology. 9 However, it commonly causes a variety of symptoms including facial pain, headache, nasal obstruction, nasal discharge, nasal bleeding, recurrent sinusitis, foul smell, and anosmia.1,10 Clinically, an intranasal tooth may be seen embedded in the mucosa of the nasal cavity or may be covered in granulation tissue.
The differential diagnosis for an ectopic tooth includes foreign bodies in the nose, rhinoliths, granulomatous infections, and tumors. Nasal endoscopic examination, CT, and panoramic radiographs can help in the diagnosis and treatment plan.
Early extraction of the intranasal tooth via a conventional or endoscopic approach prevents potential morbidity and complications. The endoscopic approach is desirable as it is associated with less morbidity and a shorter hospital stay.