
Abstract
We introduce a novel and potentially effective approach in the treatment of tonsil stones using Coblation technology. A retrospective pilot case series was performed demonstrating the effectiveness of a technique that we call Coblation tonsil cryptolysis. This technique is unique in that it can be performed in adult patients without sedation using only local anesthesia, much like laser tonsil cryptolysis. As with laser cryptolysis, pain is significant for only a few days and most adults can resume normal diet and activity within 1 week. In contrast, tonsillectomy entails significant morbidity for several weeks. However, Coblation avoids the significant disadvantages of laser use, including the potential for airway fire, retinal damage from reflected scatter, dealing with plume from vaporized tissues, oral/facial burns, and the high cost of purchasing and maintaining laser equipment. After a single session of Coblation tonsil cryptolysis, a significant decrease and even elimination of tonsil stones can potentially be achieved.
Introduction
Historically, treatment options for tonsil stones, or tonsilloliths, have been limited. Current available options include surgical tonsillectomy, which is the only known cure for this problem, and more conservative management with gargles and manual tonsillar massage. Laser cryptolysis is an alternative, less invasive option to tonsillectomy in which the tonsillar crypts are ablated resulting in scarring and resolution of tonsil stone production.12 The advantages of laser cryptolysis compared to tonsillectomy include significantly less pain (most patients eat regular food within 24 hours), faster recovery (within 1 week), and avoidance of general anesthesia (only local anesthetics required).
Unfortunately, there also are disadvantages of using a laser, including the potential for airway fire, retinal damage from reflected scatter, dealing with plume from vaporized tissues, and oral/facial burns. 3 There is also the not insignificant financial outlay for the purchase of laser equipment, maintenance, and staff training.
To minimize the disadvantages of laser use in tonsil cryptolysis while preserving all its advantages, we have successfully used Coblation (ArthroCare Corp.; Austin, Texas) to ablate tonsil crypts.
Patients and Methods
This retrospective case series was evaluated and exempted by the Institutional Review Board of Medical City Hospital (Dallas, Texas). Coblation is a well-established, FDA-approved technology already in use to perform tonsillectomy, turbinate reduction, laryngeal surgery, sinus surgery, and palate surgery.4–7 The technology employs a controlled, non-heat-driven process that uses radiofrequency energy to excite the electrolytes in a conductive medium such as saline solution or gel to create a precisely focused plasma. 8 The plasma results in tissue breakdown and/or dissolution at the point of contact, at relatively low temperatures (40 to 70°C), while causing minimal damage to surrounding tissues. Coblation's proven safety (not only for patients, but also for surgical staff) has resulted in uses beyond FDA indications, including skin resurfacing and blepharoplasties. 9
Depending on the clinical scenario and anatomic location, the surgeon can choose from a variety of wands to perform a given procedure. For the purposes of Coblation tonsil cryptolysis, the PROcise XP Plasma Wand provided the greatest active surface area while permitting complete control. For this procedure, rather than using the suction tubing and saline drip, it is best to simply dip the tip of the wand in saline gel.
Patients in our series ranged in age from 19 to 81 years; 4 men and 3 women underwent the procedure. Patients typically presented to the clinic with a long history of daily tonsil stone extrusion, causing bad breath and disruption of quality of life. Positive crypts and tonsilloliths were visualized in every candidate. A decision was made to proceed with Coblation tonsil cryptolysis after discussing the risks, benefits, and alternatives of the procedure.
The tonsils and oropharynx were sprayed with benzocaine, aminobenzoate, and tetracaine anesthetic spray twice, separated by 1 minute. Then, 2% lidocaine with 1:100,000 epinephrine was injected into the tonsils and the anterior pillars. After adequate local anesthesia was obtained, aggressive palpation was performed to thoroughly extrude the tonsil stones and caseous material that were present. Coblation was then applied to the culprit crypts resulting in complete ablation of the area. This was repeated at each tonsil crypt site. The patient was then observed for a few minutes at the conclusion of the procedure to ensure that there was no bleeding and discharged home with instructions to gargle with saline after every meal and to take hydrocodone/acetaminophen as needed for pain control.
The patients returned for postoperative visits 2 weeks and 3 months after the procedure and reported their outcomes with respect to tolerance of the procedure and resolution of tonsil stones.
Results
Patients reported their tolerability of the procedure on a scale of 1 to 10, with 1 being the near absence of pain and 10 being severe pain (table). One patient reported an 8, but all other patients reported a 5 or less. Days of narcotic pain medication use ranged from 0 to 7 days. Days to normal diet ranged from 1 to 7 days.
Five of the 7 patients stated they would undergo the procedure again if required, and 2 said they would prefer tonsillectomy. Of the 2 who would prefer tonsillectomy, 1 was the individual who reported a pain level of 8 and had the lowest overall subjective improvement of 50%. The other patient who would not repeat the procedure had the second lowest level of reported subjective improvement, at 70%. The remaining patients all had subjective improvement of 80 to 100%, and all 7 said they would recommend this procedure to friends and family.
Discussion
Tonsil stones are a potential source of halitosis, causing personal, familial, and social problems. They are typically formed in the palatine tonsils within crypts characterized by twisted invaginations extending from the surface into the tonsil parenchyma. Within these crypts, foreign particles, keratin, and exfoliated epithelium collect and calcify over time, changing from soft gels to caseous concretions known as tonsilloliths. 2 These tonsillar calculi can also be considered living biofilms and, as such, are not easily eradicated with conventional forms of treatment. 10
Although tonsillectomy is curative, this surgery is highly associated with morbidity in adult patients because of the severe sore throat that lasts for weeks, resulting in incapacitation from responsibilities (missed days of work, finding alternative caretakers for children, etc). Therefore, pain minimization while simultaneously achieving long-term relief from tonsil stones is of paramount interest in the adult population.
Results for restrospective case series of patients who underwent Coblation tonsil cryptolysis
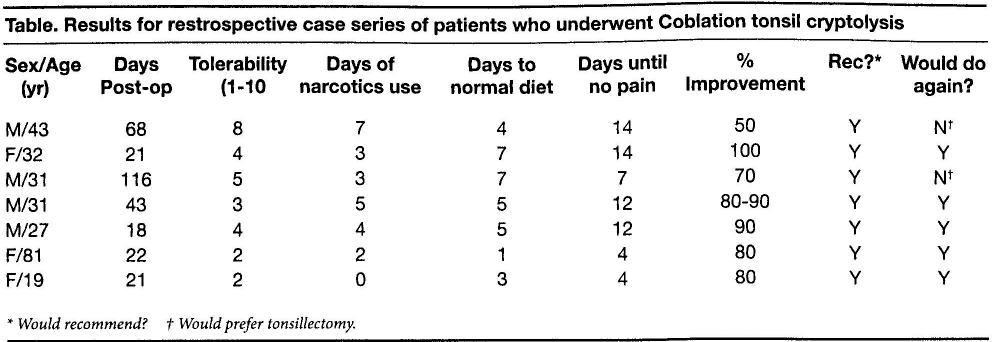
Would recommend?
Would prefer tonsillectomy.
Laser cryptolysis does achieve the goal of addressing tonsil stones while minimizing postprocedure morbidity, but it does so at the expense of intraoperative safety and increased costs. Use of any laser in the airway, including the oral cavity, has the potential hazards of airway fire, retinal damage from reflected laser scatter, damage from vaporized tissue plume, and oral/facial burns from unintended patient/surgeon movement. These risks are compounded by the gag reflex which, under most circumstances, would be simply annoying but during a laser procedure may cause physical harm.
In terms of relative cost, the Coblation device is free, and the disposable wands
average approximately $200 per wand (the cost varies depending on the wand
type used and how many wands are purchased at a time). In contrast, a portable Valam
FOX ENT laser system (Valam Corporation, New York, N.Y.), for example, costs
approximately $17,000 (
Regardless of the technique used, patient selection is important to achieve a successful unsedated procedure. Patient characteristics that allow for tonsil cryptolysis include: adult patient, minimal gag reflex, and easy visualization of the tonsil with the mouth open. Although discrete tonsil crypts are preferred for localized treatment, even tonsil resurfacing can be performed for a severely cryptic caseous tonsillitis with Coblation, although more than one session may be required. In the less ideal patient, this procedure can be easily and safely performed under general anesthesia.
In conclusion, in our small series, 71% of patients reported that the procedure was tolerable and effective enough that they would choose the procedure again if given the opportunity. In the properly selected patient, Coblation tonsil cryptolysis is a safe alternative method for treating tonsil stones in the unsedated patient and can be performed on less ideal patients under general anesthesia.
To the best of our knowledge, this is the first report describing the use of this technique.