
Abstract
The presentation of ectopic cervical thymic tissue as an anterior neck mass is rare. We report 3 similar cases in 3 boys—2 who had a thymic cyst and 1 who had an ectopic cervical thymus. We discuss the radiographic presentation on ultrasound and magnetic resonance imaging in these cases. We also review the typical histologic picture; histology is the only way of diagnosing this condition.
Introduction
Ectopic cervical thymic tissue presenting as a neck mass is rare. Only about 100 cases have been reported in the world literature. Approximately 70% of thymic cysts occur in patients younger than 20 years. 1 In 90% of cases, patients have no specific symptoms. 1 Ectopic cervical thymic tissue is difficult to diagnose preoperatively; the diagnosis can be made only on histology of a biopsy specimen. Once the cyst is diagnosed, surgical excision is the treatment of choice. 1 We report 3 similar cases of ectopic cervical thymic tissue that were all seen within a 1-year period.
Case Reports
Patient 1
A 6-year-old boy presented with a painless right neck swelling that had been present for about 6 months. The size of the mass fluctuated, but it had recently become more visible. On examination, a 3 × 5-cm cystic mass was felt anterior to the sternocleidomastoid muscle. The mass did not transilluminate, and no lymph nodes were palpable. Ultrasonography demonstrated an echogenic 40 × 22 × 11-mm cyst anterior to and close to the common carotid artery and internal jugular vein (figure 1). The patient was tentatively diagnosed with a branchial cyst.
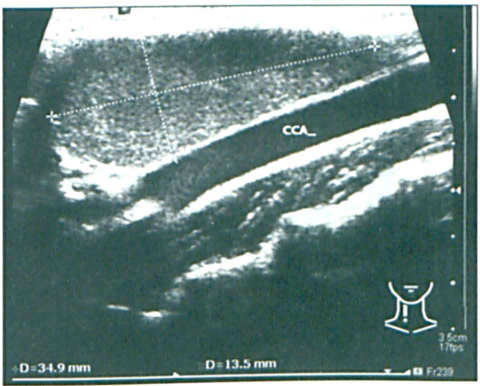
Patient 1. Ultrasonography demonstrates the cystic nature of the mass near the common carotid artery (CCA).
During surgery, the cyst was found to extend deeply into the area of the internal jugular vein, carotid artery, and vagus nerve. It contained dark fluid and some solid material. Histology identified Hassall corpuscles, and on that basis, a diagnosis of a thymic cyst was made.
Patient 2
A 6-year-old boy was brought to us with a 3-month history of a painless neck mass that fluctuated in size. Examination revealed a soft, 5-cm cystic mass in the anterior triangle of the neck; its posterior border extended medially to the sternocleidomastoid muscle. In view of the boy's age and the location of the cyst, we made a provisional diagnosis of a branchial arch remnant, most likely from the second arch.
At surgery, a large loculated cyst was found that had to be dissected from the internal carotid artery, internal jugular vein, and the vagus and accessory nerves. The cyst measured 90 × 50 × 33 mm, and it contained thick, yellow, inspissated material (figure 2, A). Its outer surface was smooth, and its inner surface had a trabeculated appearance. Pathologic examination detected characteristics of a thymic cyst (figure 2, B). Microscopic examination identified the mass as a multiloculated cyst partially lined with squamous epithelium. The epithelium demonstrated no cytologic atypia. Lobules of thymic tissue containing Hassall corpuscles were seen in the cyst wall. In some areas, the cyst lining had been lost and an associated multinucleated foreign-body giant-cell reaction to the cyst contents was present in the surrounding tissue. Collections of cholesterol clefts were also present in the cyst wall.
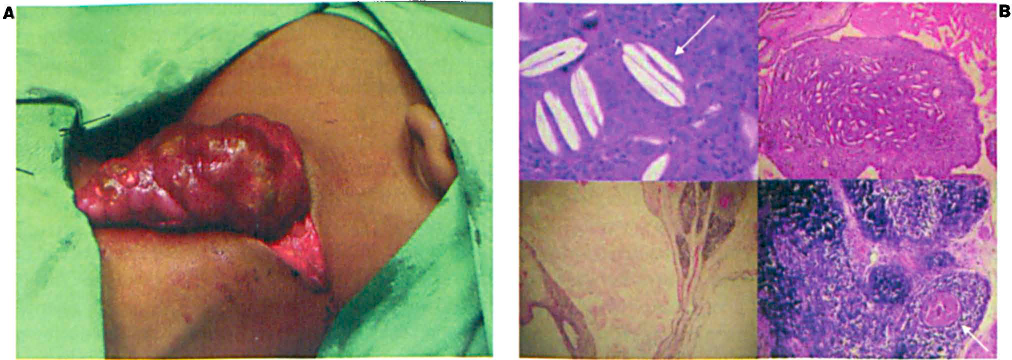
Patient 2.
Patient 3
A 7-month-old boy presented with a mass below the right mandible. The lesion had been noticed soon after birth, and it had grown progressively bigger. The patient seemed to have difficulty swallowing, but his history was otherwise unremarkable. Examination revealed that the mass was located below the submandibular gland and that it extended medially into the neck. Magnetic resonance imaging (MRI) showed that a very large (35 × 29 × 23 mm) mass had displaced the vasculature and extended into the retropharyngeal space (figure 3). On MRI, the mass did not exhibit the multiloculated appearance typical of a cystic hygroma. The results of an earlier biopsy obtained from the referring hospital had suggested a cyst of thymic origin.
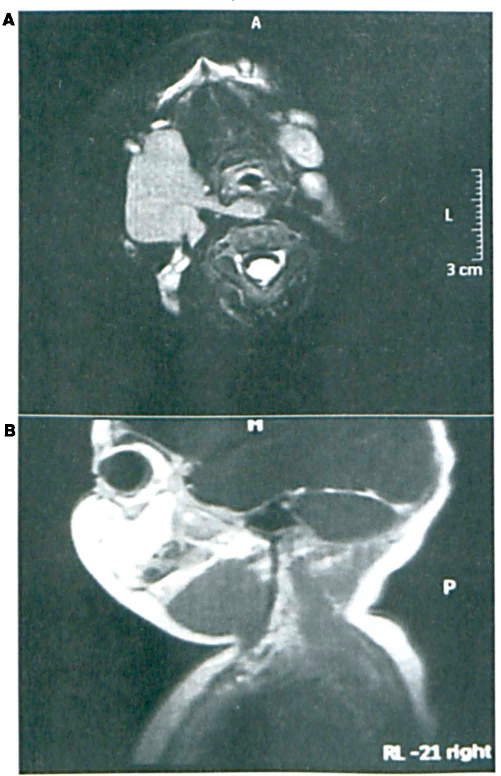
Patient 3. Axial (
Surgery was undertaken via a right submandibular approach. Clinically, the mass had the appearance of thymic tissue. It extended around the great vessels with retropharyngeal extension. There was a distinct plane between the mass and the surrounding tissue, which allowed us to easily dissect and remove it. Histology confirmed the clinical suspicion of an ectopic cervical thymus.
Discussion
Ectopic cervical thymic cysts are believed to represent persistent tubular remnants of a third pharyngeal pouch (figure 4).2,3 The thymus gland is the first lymphoid organ to develop during embryogenesis; its development has been well reviewed by Berenos-Riley et al. 3 During the sixth week of embryonic life, the thymus begins its development as two bilateral outgrowths from the third pharyngeal pouch. Both outgrowths elongate medially and caudally to form the thymopharyngeal ducts. During the seventh week, the connections between the ducts and the pharynx are severed. The ductal lumina are obliterated by epithelial proliferation into solid cords known as thymopharyngeal cords. After the eighth week of gestation, the caudal parts of the cords meet in the midline and fuse in the upper mediastinum. They reach their final position during the ninth week and evolve into thymic lobules. A capsule surrounds the developing thymus and maintains the gland in close association with the parietal pericardium, which is key to its descent to the mediastinum. By the tenth week, adjacent mesenchymal cells destroy the solid cords of the pharyngeal ectoderm, and the remaining epithelium transforms into Hassall corpuscles.
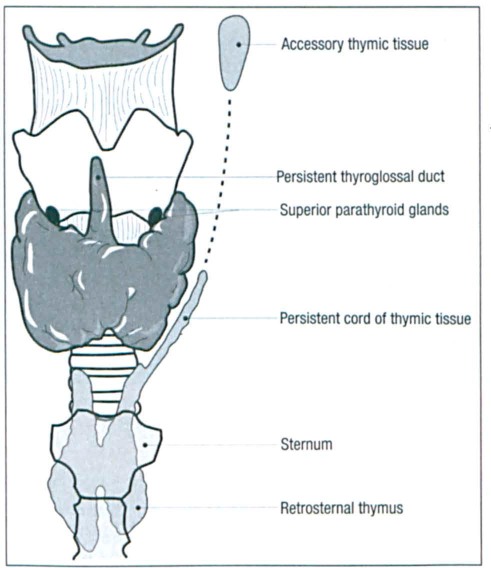
Illustration Shows the Persistent Cord of Thymic Tissue and the Areas Where a Cyst Might Develop.
The usual pathway of the thymus gland's descent is via a third branchial arch derivative, which explains the gland's intimate relationship with the large vessels in the neck. The pathway starts at the piriform sinus and pierces the thyrohyoid membrane. Then it exits between the common carotid artery and the vagus nerve. From there it passes posterior to the glossopharyngeal nerve and lateral to the thyroid and then into the mediastinum.
It has been hypothesized that cervical thymic cysts occur as a result of cystic degeneration of Hassall corpuscles or cystic changes in remnants of the thymopharyngeal ducts.1,3 This would explain the various locations of thymic anomalies, which can be found anywhere along the embryologic course of the thymus gland's descent. In 50% of cases, thymic cysts may present with mediastinal extension. This can be either direct extension or connection to a vestigial remnant or solid cord.4,5 Cervical thymic tissue can be found in the form of aberrant solid thymic rests or cystic thymic tissue. 6 Nowak et al reviewed 91 cases, 84% of which presented as neck masses and 16% of which presented as enlarged anterior mediastinal masses. 7 The cystic form (71%) was substantially more common than the solid form (29%). Solid forms develop as a result of either a complete or partial failure of the gland to descend from the neck or from a sequestration and failure of involution along the normal thymic pathway into the mediastinum. 7 Cervical thymic tissue often extends into the retropharyngeal space. 8
Most cases (75%) of ectopic thymic tissue occur in boys in the first decade of life.1,9 The reason for this is unknown. Although affected patients are usually asymptomatic, severe respiratory compromise has been known to occur. 5
In view of their rarity and the lack of distinguishing imaging and laboratory features, ectopic cervical thymic cysts and masses generally are not suspected preoperatively.1,9 There is no known imaging modality or laboratory evaluation that will accurately identify cervical thymic cysts. 10 As a result, they are frequently misdiagnosed as lymphadenitis, branchial cysts, thyroglossal duct cysts, cystic hygromas, thyroid adenomas, and parathyroid, dermoid, or epidermoid cysts.1,11 Histologic investigation of biopsied tissue remains the only definitive means of making the diagnosis. 12 The histologic criteria for diagnosis are the presence of thymic tissue with Hassall corpuscles and cholesterol granulomata. 13
In a few cases, these cysts have proved to be malignant, even in asymptomatic patients. 14 The preferred treatment is surgical excision. In neonates, the presence of mediastinal thymic tissue should be documented prior to excision of a cervical mass because of the thymus’ important role in the development of the immune system.14,15