
Abstract
Pleomorphic adenomas of the nasal cavity are rare. We describe the case of a middle-aged white man who presented to our clinic with a long history of unilateral nasal obstruction. Preoperative imaging was performed, and the patient was taken to the operating room for endoscopic excision of the lesion. Surgical margins were negative. The patient's nasal obstruction resolved, and he was doing well at his first postoperative visit. The pathologic diagnosis was a pleomorphic adenoma. We discuss the features and management of this entity.
Introduction
Pleomorphic adenoma is the most common benign neoplasm of the major salivary glands, accounting for approximately 65% of all salivary gland neoplasms. 1 In the salivary glands, 80% of all cases of pleomorphic adenoma occur in the parotid gland, and 6.5 to 8% of cases occur in the minor salivary glands.2,3 Pleomorphic adenomas of the upper respiratory tract are very rare in the literature. When they have occurred, the most common site of origin is the nasal cavity; other cases have been documented in the maxillary sinus, nasopharynx, larynx, and trachea.3,4 We report a new case of a pleomorphic adenoma of the nasal cavity.
Case Report
A 44-year-old white man presented to the otolaryngology clinic with a complaint of a unilateral (left-sided) nasal obstruction that had slowly worsened over the previous 5 years. He denied associated pain, epiphora, epistaxis, rhinorrhea, and episodes of sinusitis. He also denied occupational exposures to wood and heavy metals. He reported no fevers, chills, night sweats, lymphadenopathy, or recent change in weight. His medical history was significant for obstructive sleep apnea, hypertension, and the removal of a bone cyst from his right humerus as a teenager. He was a nonsmoker and drank socially.
On examination, anterior rhinoscopy revealed that the septum was mildly deviated to the right. On the left, the inferior turbinate extended from the floor of the nose to the nasal roof. Neither rigid nor flexible endoscopy on the left was possible in the office because of the enlargement of the inferior turbinate. The tympanic membranes were normal, and findings on examination of the oral cavity, oropharynx, and neck were within normal limits.
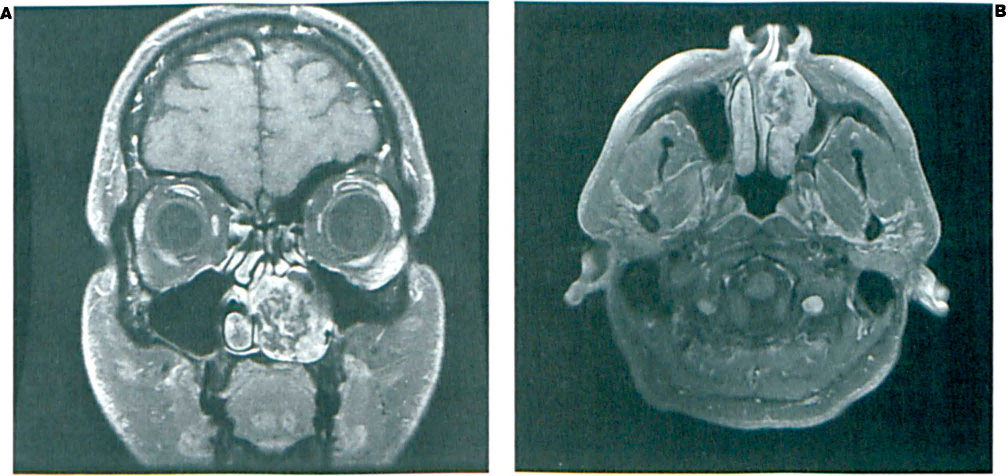
Computed tomography (CT) detected a soft-tissue mass with calcification that was obscuring the left nasal cavity and causing osseous displacement, but no bony destruction or invasion was evident (figure 1). Magnetic resonance imaging (MRI) demonstrated a heterogeneous 3-cm mass arising from the inferior turbinate; again, no destruction or invasion was evident (figure 2).
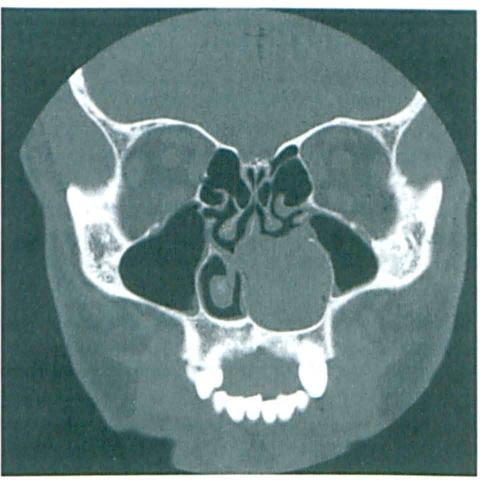
Coronal CT in bone windows shows the soft-tissue mass in the left nasal cavity.
The patient was counseled about endoscopic removal of the mass and a possible lateral rhinotomy or medial maxillectomy. Intraoperatively, the mass was found to be confined to the anteroinferior turbinate. It was removed without complication intranasally with the endoscope. Negative margins after wide local excision were confirmed by frozen-section histopathology. Postoperatively, the nasal obstruction resolved and the patient did well. Pathology identified the mass as a pleomorphic adenoma.
Discussion
Approximately 80% of intranasal pleomorphic adenomas are found in the septum. 3 Only about 20% are found in the lateral wall or turbinate, 3 despite the fact that there is a significantly higher proportion of mucous and serous glands located on the lateral nasal wall. 5 Several theories have been proposed to explain why there is a higher incidence of pleomorphic adenomas in the nasal septum than in the gland-rich tissue of the lateral nasal wall, but none has been proven.
The differential diagnosis of an intranasal mass is broad; it includes inverting papilloma, benign nasal polyp, squamous cell carcinoma, cartilaginous tumors, adenocarcinoma, melanoma, chondroma, encephalocele, and adenoid cystic carcinoma.5–9 Most intranasal pleomorphic adenomas arise in whites from the third to sixth decades of life; there is a slight female preponderance. 1 The most common presenting symptom (75% of cases) is unilateral nasal obstruction. 5 Less often, the chief complaint is epistaxis, sinusitis, or a mass within the nasal cavity.1,5 Sinusitis can occur as a result of either (1) an extension of a primary neoplasm into the maxillary sinus or (2) obstruction of the osteomeatal complex by the tumor. Occasionally, pleomorphic adenomas arising from the nasopharynx obstruct the eustachian tubes and cause symptoms of eustachian tube dysfunction. 10 Generally, affected patients present within 1 year of the onset of symptoms. 5
Most intranasal pleomorphic adenomas range in size from 0.5 to 7 cm, and most have a broad base (a few have a pedicled base). 5 These neoplasms have been described as exophytic, polypoid, oval, dome-shaped, firm, and gray. 5 Grossly, these masses have a polypoid, smooth, lobulated appearance with a well-defined capsule. 1 No destruction of surrounding tissue is seen.
Histologically, pleomorphic adenomas of the nasal cavity are not identical to those found in the salivary glands. In the nasal cavity, these neoplasms have greater cellularity and they contain more epithelial components than the chondroid, myxoid, and collagenous stromal components that are seen in pleomorphic adenomas of the parotid gland. 5 These small, oval epithelial cells are densely packed “back to back” in masses or cords, a pattern that is associated with benign neoplasms. 5 There is usually minimal or no evidence of mitotic activity.
Malignant transformation of pleomorphic adenoma of the nasal cavity has been reported in 2.4 to 10% of cases. 10 The most common variant is carcinoma ex pleomorphic adenoma, which is capable of metastasis. A less common form of malignant transformation is the malignant mixed form, in which both the epithelial and stromal components transform and metastasize together. Bone is the most common site of metastasis, followed by the liver, lung, and regional lymph nodes.
The radiographic findings with pleomorphic adenomas of the nasal cavity are nonspecific, much like the clinical presentation. CT typically shows a well-defined soft-tissue mass; calcification is seen in rare cases. CT allows the clinician to assess bony involvement or destruction, which may occur when a neoplasm has been left untreated over time. 1 MRI is used to assess the epithelial and stromal components of the neoplasm, as well as the surrounding soft tissue. MRI of the stromal components reveals a low signal intensity on T1-weighted imaging and an intermediate to high signal intensity on T2-weighted imaging; epithelial components have a low signal intensity on T2-weighted imaging.
Treatment entails wide local excision with clear margins. 5 If these neoplasms are allowed to progress untreated, their expansion may cause local destruction of the paranasal sinuses. Four approaches to the removal of intranasal pleomorphic adenomas have been reported in the literature: a transpalatal approach, a lateral rhinotomy, a Le Fort I osteotomy, and an endoscopic intranasal approach.1,11 The transpalatal approach provides good exposure of the posterior nasal cavity and nasopharynx, but considerable palatal dysfunction from soft-palate retraction is a known complication. 1 The lateral rhinotomy, which requires an external approach, is typically not favored for this benign neoplasm because it leaves a facial scar. A facial scar can be avoided by using the Le Fort I osteotomy, but this technique requires fixation of the alveolar ridge. The endoscopic intranasal approach allows for good visualization without external scarring and is therefore the preferred approach.
Postoperative follow-up is necessary for all patients with an intranasal pleomorphic adenoma because as many as 10% of patients may experience a recurrence despite wide local excision with clear margins. 5 Even so, this recurrence rate is much lower than the 50% recurrence rate seen in patients with pleomorphic adenoma of the parotid gland. 5 Histologically, recurrence is most associated with the myxoid stromal pattern. Freeman et al reported the discovery of a metastasis 17 years after the excision of a primary intranasal pleomorphic adenoma. 12
In conclusion, intranasal pleomorphic adenoma is rare. The most common site of this benign neoplasm is the parotid gland. Compared with pleomorphic adenomas of the parotid, intranasal lesions are associated with greater cellularity (more epithelial components), a more benign course overall, and a lower rate of recurrence (10 vs. 50%). 5 Intranasal pleomorphic adenomas have no definitive clinical or radiographic findings. Despite the fact that intranasal pleomorphic adenomas have a nonspecific appearance on CT and MRI, it is advantageous to use these two modalities to assess bony destruction and soft-tissue components, respectively. The treatment of choice is local excision with clear margins, usually via an intranasal approach. Recurrence and metastasis are uncommon, but patients need to be followed postoperatively nevertheless.