
Abstract
We report a case of a neurilemmoma presenting as a midline nasal mass in a 13-year-old girl. To the best of our knowledge, this is the first report of a nasal neurilemmoma in a pediatric patient. Although this neoplasm is benign in nature, surgical resection is warranted to prevent recurrence, and it is the sole means of treatment. The overall prognosis is excellent, as was the case for our patient. We discuss the diagnosis and management of neurilemmomas and urge physicians not to exclude nasal neurilemmoma from the differential diagnosis in a pediatric patient who presents with a nasal mass.
Introduction
Schwannomas are benign neural sheath tumors that can be further classified into neurilemmomas and neurofibromas. Each is a distinctly different type of neural growth, yet the terms schwannoma and neurilemmoma often are used interchangeably. With an incidence of 1 per every 3,000 live births, 1 this benign neoplasm typically presents in the third to sixth decade of life.1–3 Neurilemmomas arise from Schwann cells of sympathetic, peripheral, or cranial nerves. Most often, they originate from the VIIIth cranial nerve. 4 These tumors have a predilection for the head and neck region, as this area is afflicted in close to one-third of all cases. 1 Despite this, they can originate from anywhere in the body, thus obscuring the diagnosis.
With such a wide range of possible locations, neurilemmomas can present with a variety of symptoms. Their slow growth often leads to a misdiagnosis. Although they are noninvasive in nature, their continual growth results in symptoms arising from the compression of nearby anatomic structures. Only 4% are found in the nose or paranasal sinuses.1,4,5 This, along with a much greater occurrence in the adult population, makes our report an unusual presentation of a neurilemmoma. We describe a case of a 13-year-old girl with a midline nasal mass that was diagnosed as a neurilemmoma after excision.
Case Report
A 13-year-old girl presented with a mass on her nasal dorsum after being hit with a ball approximately 7 years earlier. The patient sought evaluation because she was concerned about the enlargement of the mass, which had become more noticeable during the previous 2 years. She did not have any associated symptoms of rhinorrhea, epistaxis, or nasal obstruction.
On physical examination, a firm, 3 × 2-cm mass was visualized on the nasal dorsum. It was slightly mobile with palpation and not fixed to the overlying skin. Coronal and axial computed tomography (CT) scans confirmed the presence of a well-defined, 2 × 1.8 × 1-cm mass on the nasal dorsum, deep to the skin (figure 1). There was minimal contrast enhancement. Surgical excision was planned for both diagnosis and therapeutic management of the patient's midline nasal mass.
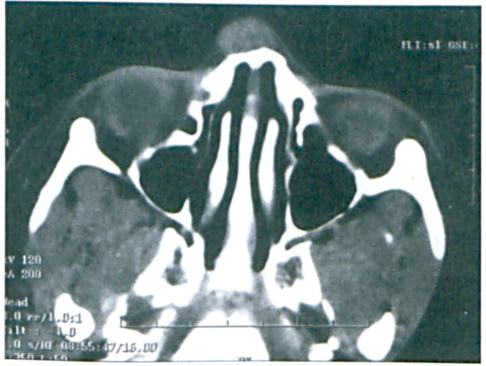
Axial CT Scan with Contrast Shows the Neurilemmoma on the Nasal Dorsum and the “Scalloping” Nasal Bone.
The procedure was performed with an endoscopic endonasal approach for therapeutic and aesthetic benefit. An intercartilaginous incision was made between the upper and lower lateral cartilage on the left. The nasal skin was elevated off the dorsum. A 4° telescope was placed intranasally through the incision for visualization. The tumor was completely excised endoscopically from the surrounding tissues. Preoperative and postoperative lateral views are shown to emphasize the improvement and aesthetic benefit obtained by avoiding an external approach (figure 2).
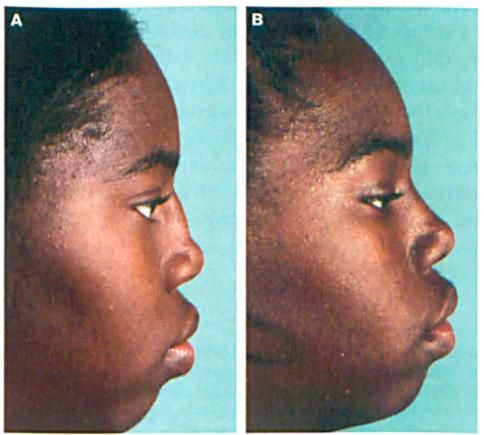
Preoperative Lateral View (
Gross examination of the excised specimen identified a 1.6 × 0.8 × 1.2-cm firm, circular, pinkishtan mass. It stained positively for S-100 protein, and histopathologic examination revealed an Antoni-A pattern, as evidenced by the Verocay bodies (figure 3). This confirmed the diagnosis of a neurilemmoma. The child was well and without recurrence at the 2-year follow-up.
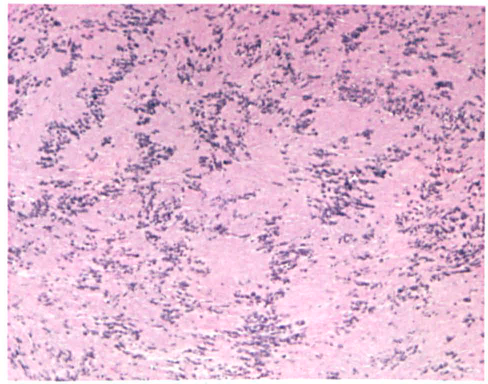
Histopathology reveals characteristics typical of a neurilemmoma: elongated cells with oval nuclei and nuclear palisading, forming Verocay bodies (H&E, original magnification x100).
Discussion
Neurilemmomas are benign, slow-growing, encapsulated tumors. Usually found as solitary masses, they are derived from Schwann cells, which typically encase the nerve. Since the neural fibers are not affected, the nerve function usually remains intact. Much of the existing literature states mere is an equal incidence between the sexes, although some case series have shown a female preponderance.1–3,5
Tissue sampling, to show immunoreactivity for the S-100 protein, is required for accurate diagnosis. In addition, based on the histologic examination, the tumor can be classified by one of two distinct patterns: Antoni type A or B. The type A pattern has spindle cells arranged in a palisading manner with two linear strips; one strip consists of aligned nuclei, and the other lies adjacently and is composed of cytoplasm. The cytoplasmic strip is commonly referred to as a Verocay body. The Antoni-B pattern is much less organized with loose, myxoid stroma and is hypocellular in comparison. Of note, there are previous reports of both patterns being present within the same tissue sample. 3
Therapy is limited to surgical excision. Neurilemmomas are resistant to radiation, and chemotherapy is not indicated.1–3,5,6 Preoperative imaging is required to define the exact location and to rule out any intracranial extension. Malignant transformation is unlikely, but complete excision is necessary because recurrence has been documented. The prognosis associated with neurilemmoma is excellent, with symptomatic resolution.5,6
Our case was a rare presentation of a nasal neurilemmoma in a child. To date, only 3 cases of this tumor in the pediatric population have been reported, all of which were localized to different areas: endobronchial, 7 the thyroid gland, 8 and the larynx. 2 Although neurilemmomas commonly affect the head and neck area, only 4% arise from the nasal region.1,4,5 In fact, one study, spanning the period between 1943 and December 2006, found a total of only 62 reported cases of nasal neurilemmomas. 1
Numerous case series have been published regarding extracranial head and neck schwannomas, but to the best of our knowledge, only 2 of these reports have documented nasal neurilemmomas. One of these, involving 2 cases, was from McKay Memorial Hospital in Taipei 9 ; the more recent was from the Ruijin Hospital in Shanghai and documented 4 nasal neurilemmomas. 10 Neither study included comments regarding the specific ages of the patients with the nasal masses. Therefore, we believe ours is the first report of a neurilemmoma of the nasal dorsum in a pediatric patient.
Regardless of the patient's age or the location of the neurilemmoma, surgical excision is the only definitive treatment. Adequate removal is essential to prevent recurrence, yet a cautious technique should be employed because of the close proximity to the nerve from which the neurilemmoma originates. Additionally, priority should be given to minimizing cosmetic deformity, if possible, as this tumor is noninvasive and slow growing in nature. The endoscopic endonasal route we chose afforded good exposure, adequate removal, and an excellent outcome.
In conclusion, nasal midline masses have a wide differential diagnosis, including inflammatory lesions, traumatic deformities, benign neoplasms, malignancies, and congenital masses. The most common in the pediatric population are congenital growths, such as dermal sinus cysts, encephaloceles, and gliomas. 11 In this population, neurilemmomas rank low on the differential for a nasal mass. However, they should not be excluded as they can occur at any age and location.