
Abstract
We present a case of bilateral otitis externa that did not respond to local treatment. Cutaneous biopsies revealed bilateral amyloid depositions secondary to multiple myeloma. Persistent, identical bilateral canal lesions may be the only manifestation of treatable systemic disease and should be biopsied, even though their bilaterality argues against malignancy.
Introduction
Chronic otitis externa is common and usually bilateral. The goal of treatment is to resolve the infection and return the canal to its previous morphology and function. We present an unusual case in which external canal skin changes were clinically identical to chronic otitis externa, but biopsy of the lesion established a diagnosis of amyloidosis. The patient was subsequently treated for multiple myeloma and is still alive 11 years after diagnosis.
Case Report
A 47-year-old woman presented to the Otolaryngology Clinic in November of 1998 with bilateral cerumen impaction and bilateral narrowing of the external auditory meatuses (figure 1). The heaped-up appearance of the canal skin was clinically interpreted and treated as bilateral chronic otitis externa. No other abnormalities were identified on head and neck examination.
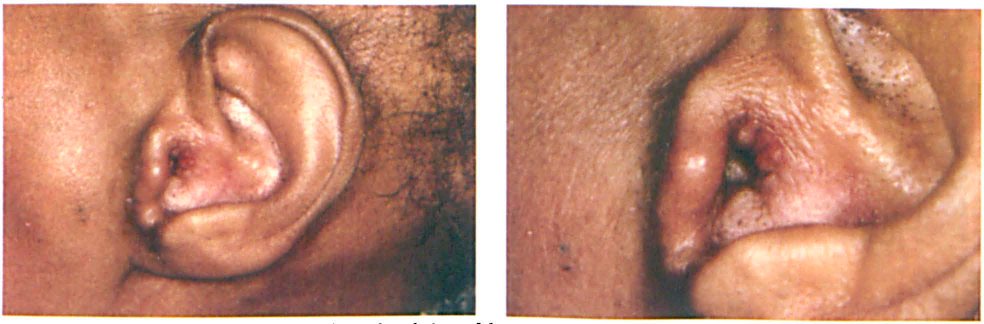
Photographs of the Left Pinna Show Heaped-Up Lesions of the External Auditory Meatus.
The patient returned 2 and 3 months later for cleaning and examination. At the time of her third cleaning, complaints of increasing lower body edema and a finding of monoclonal lambda light chains in her urine brought her to the attention of the Hematology-Oncology service. She was diagnosed with multiple myeloma with monoclonal lambda light chains in serum and urine.
The patient returned to the Otolaryngology Clinic 3 weeks after the diagnosis of her plasma cell dyscrasia. After appropriate informed consent was obtained, biopsy of her left ear canal was performed, which identified dermal amyloidosis, which was confirmed with Congo red stain with apple-green birefringence on polarization (figure 2). A diagnosis of amyloidosis was confirmed by peritoneal fat pad aspirate. Bone marrow biopsy was slightly hypercellular, with cellularity of 65% and plasma cells accounting for 70%.
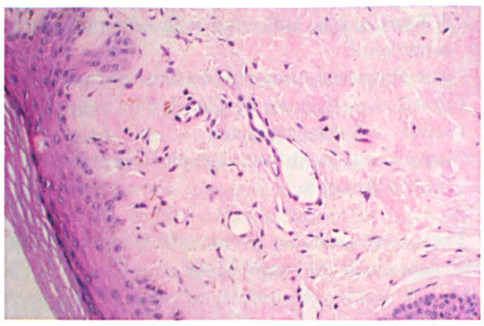
Biopsy section shows amorphous stromal deposits characteristic of amyloid, confirmed by polarization of Congo-red–stained material (original magnification x100).
Her multiple myeloma was treated with melphalan and prednisone. In the following 11 years, her ear examination and complaints remained unchanged, and she was treated with supportive care and cleaning. The patient went on to develop symptoms consistent with systemic amyloidosis, including:
pleural effusion secondary to amyloid infiltration of the pleura;
S4 heart sound, indicating reduced ventricular compliance;
gastrointestinal autonomic dysfunction resulting in abdominal fullness, motility dysfunction, early satiety, and weight loss; and
hepatomegaly with liver edge palpable 6 cm below the costal margin.
The patient is still alive 11 years after being diagnosed with light-chain (AL) amyloidosis.
Discussion
Amyloidosis of the external auditory canal is rare. Six previous articles1–6 have reported 9 cases of cutaneous amyloidosis of the pinna or external ear canal. Primary localized amyloidosis of the pinna, concha, or canal without systemic findings has been reported in 7 cases by four authors.1–4 Only 2 previous cases of systemic amyloidosis presenting with external auditory canal complaints have been reported.5,6 Subsequent workup identified polyclonal increase in gamma globulin levels in one case 5 and multiple myeloma in the other. 6 One of these cases was presumptively treated as chronic external otitis, 6 as was ours.
When the correct diagnosis has been made, it is clear that the process is not inflammatory or infectious but is the manifestation of underlying systemic diesase. Treatment of external canal amyloidosis should be directed toward ear canal hygiene, and not toward return to normal morphology.
Recalcitrant chronic otitis externa should redirect the physician to consider noninfectious etiologies. While many physicians would biopsy a unilateral canal lesion to rule out carcinoma, bilateral canal lesions not responding to therapy should also be biopsied. In our patient, the ear canal findings were the only cutaneous manifestations of her multiple myeloma.
By far the most interesting issue in this particular case is why the external auditory canal should be a preferential site of amyloid deposition. It is difficult to speculate what feature of the canal—its blood supply, the thinness of the canal skin, a possible immunologic feature of the canals—could encourage a predilection to amyloid deposition there. Clearly, some feature of the canal attracts this deposition, otherwise it would not be bilateral.
Amyloidosis is deposition of abnormal or excess proteins that form a distinctive conformation within normal tissues. Multiple disease processes overproduce the array of functional and nonfunctional proteins that can form amyloid deposits. 7 Therefore, a finding of amyloidosis mandates appropriate referral for further evaluation for systemic disease.