
Abstract

Odontogenic fibromas are rare, benign neoplasms composed of odontogenic epithelium embedded in fibrous stroma. They may arise within the jaw bones (central odontogenic fibroma) or in an extraosseous site within the oral cavity (peripheral odontogenic fibroma).
Clinically, peripheral odontogenic fibroma (POF) forms a firm gingival mass that resembles a common fibrous epulis. Central odontogenic fibroma (COF) presents as a painless, asymptomatic, slow-growing mass in the mandible or maxilla. COF is more prevalent in females and can occur at any age. Radiologically, COF has well-defined borders, is usually radiolucent, and may be unilocular or, if larger, may show multiloculation.
Histologically, odontogenic fibromas can be divided into two types: epithelium-poor (simple type) and epithelium-rich (complex, or WHO type). The epithelium-poor type lacks odontogenic epithelium (figure 1) or only contains scattered islands and cords of odontogenic epithelial remnants embedded in a collagenous or fibromyxoid stroma. The epithelium-rich type is more cellular because it has more prominent islands or strands of odontogenic epithelium growing within a dense fibrous stroma (figure 2), admixed with occasional cementum-like calcified deposits. These lesions are rarely encapsulated.
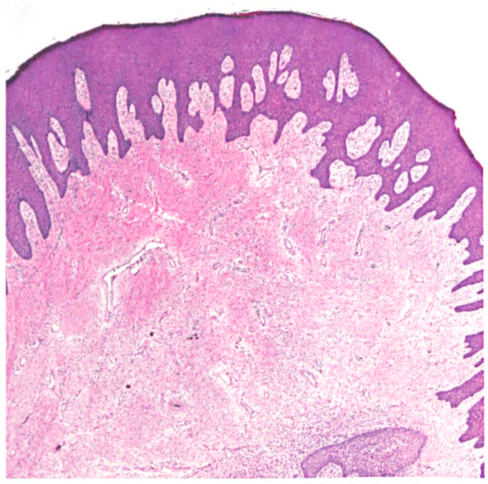
In this epithelium-poor POF of the gingiva, odontogenic epithelium is notably absent in fibrous tumor stroma (H&E, original magnification x40).
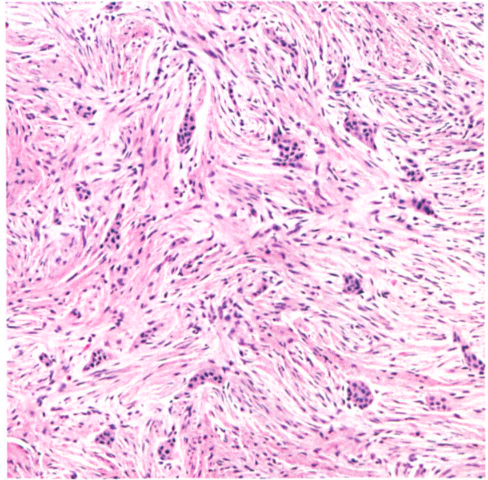
This epithelium-rich COF contains islands of inactive odontogenic epithelium surrounded by fibrous tumor stroma (H&E, original magnification x200).
Two variants of COF have been described: (1) a granular-cell variant that has large, S-100–negative cells with eosinophilic granules, and (2) a hybrid giant-cell granuloma-like variant (figure 3). The differential diagnosis of a POF includes a fibrous epulis and odontogenic gingival epithelial hamartoma, whereas for a COF one needs to consider hyperplastic dental follicles, myxofibroma, desmoplastic fibroma, odontogenic myxoma, intraosseous neurofibroma, and possibly carcinoma.
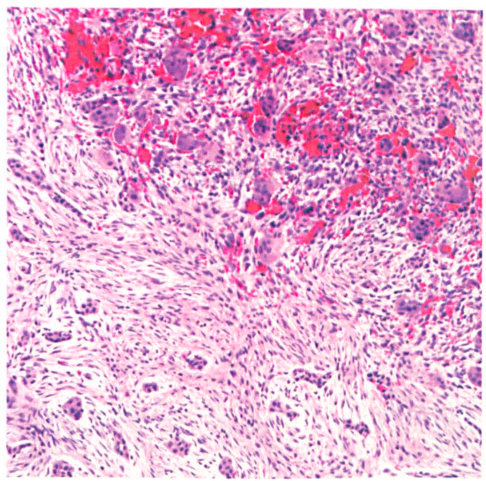
In this hybrid giant-cell granuloma-like variant of COF, odontogenic rests are seen adjacent to many giant cells admixed with hemorrhage (H&E, original magnification x200).
Since these lesions are benign and do not infiltrate bone, their management consists of excision for a POF, and enucleation by vigorous curettage for a COF. Larger lesions may require more extensive surgery. Their recurrence rate is low. Although the histologic distinction between the different types is controversial and probably of no value in predicting behavior, the presence of a giant-cell component has been suggested by some authors to portend a slightly higher recurrence rate.