
Abstract
Laryngeal cancer in patients younger than 30 years is uncommon. We present data on this population obtained from the National Cancer Institute's Surveillance, Epidemiology, and End Results (SEER) Program. We identified 99 patients in this age group from the SEER 17 registry, which includes data submitted from 1973 through 2003. This population was made up of 52 females and 47 males; most were white, and most were aged 25 to 29 years. Malignancies of the glottis were the most common cancers, followed by supraglottic lesions. The 5-year relative survival rate was lowest among those aged 15 to 19 years—60.1%; 5-year relative survival among those aged 20 to 24 and 25 to 29 years was 87.7 and 87.4%, respectively. The etiology of squamous cell carcinoma (SCC) in children and adolescents remains uncertain, but in the adult population, a history of smoking, drinking, and poor oral hygiene cannot be ignored. Carcinoma of the larynx in young people has been related to malignant degeneration of papillomas and to complications of radiotherapy for papillomas. Infection with the human immunodeficiency virus possibly accelerates the development of SCC in patients with significant risk factors, presumably by impairing normal immune surveillance mechanisms.
Introduction
Most patients with laryngeal carcinoma are older than 30 years; the peak prevalence occurs in the sixth decade of life. Among the reported risk factors for laryngeal carcinoma are papillomatosis of the larynx, laryngopharyngeal reflux, human immunodeficiency virus (HIV) infection, immunosuppressive therapy, exposure to drug use during pregnancy, both active and passive smoking, alcohol use, poor oral hygiene, and a family history of cancer. 1 Numerous studies have documented that tobacco and alcohol synergistically produce a progression of changes in the mucosa of the upper aerodigestive tract; these changes can progress from leukoplakia or dysplasia to carcinoma in situ and finally to invasive carcinoma.2-5 However, the literature on head and neck cancer in young adults reveals that these patients generally have not engaged in excessive smoking and drinking.6-8 Others have reported that a disproportionate number of these patients were women 9 and that chances for survival were relatively good. 10
Carcinoma of the larynx in younger patients has also been associated with malignant degeneration of papillomas and to complications of radiotherapy for papillomatosis.11,12 Researchers have also looked at age at the time of the onset of papillomatosis, the different types of human papillomavirus, infection with multiple viruses, histopathologic features, and immunohistochemical measures of cell proliferation.13–17
Questions have been raised as to whether younger patients with an aggressive malignancy have an underlying genetic or immune defect that predisposed them to it. 18 Schantz et al noted a greater number of bleomycininduced chromosomal breaks in cells among young adults with head and neck squamous cell carcinoma (SCC), which is the most common type of laryngeal cancer in patients younger than 30 years. 19 In subsequent research, they found that these breaks might be responsible for an increased risk of developing multiple malignancies. 20 Singh et al reviewed the literature and discovered several trends. 21 Based on their findings, they surmised that younger patients may have genetically distinct cancers, given that they experience less overall exposure to carcinogens and that they have a higher prevalence of HIV infection.
Patients with head and neck SCC present with a wide variety of presenting manifestations and tumor behaviors. Symptoms of hoarseness, dysphagia, and/ or throat pain require the same thorough investigation in younger patients as in older patients.
In this article, we describe our investigation of laryngeal cancer in a younger age group.
Patients and methods
Our patient population was drawn from the Surveillance, Epidemiology, and End Results (SEER) tumor registry, which has been maintained by the National Cancer Institute (NCI) since 1973. 22 The geographic areas that are included in the SEER database represent an estimated 10% of the United States population, and they include both urban and rural areas. Patient follow-up is performed both passively (by reviews of national death certificate data) and actively (by annual correspondence with each patient's healthcare provider).
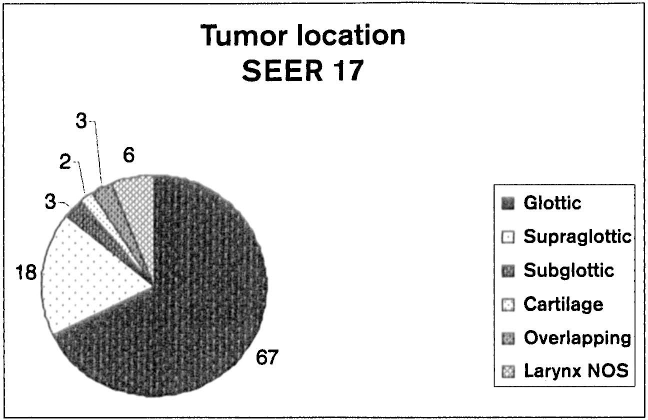
Chart shows the 99 laryngeal cancers grouped by location (NOS = not otherwise specified).
We searched the SEER 17 database, which includes cases diagnosed from 1973 through 2003, and extracted information on all patients younger than 30 years who had a diagnosis of laryngeal cancer. In doing so, we used appropriate International Classification of Diseases for Oncology codes. 23 Our search yielded 99 such cases.
In addition to demographic data, we analyzed data on tumor location, the type of cancer, and 5-year “relative survival” rates. According to the NCI, “Relative survival is a net survival measure representing cancer survival in the absence of other causes of death. Relative survival is defined as the ratio of the proportion of observed survivors in a cohort of cancer patients to the proportion of expected survivors in a comparable set of [cancer-free] individuals. The formulation is based on the assumption of independent competing causes of death. The relative survival rate adjusts for the general survival rate of the U.S. population for that race, sex, age, and date at which the age was coded. If age, race, sex, or year information is missing, that individual is excluded from the analysis.” 24
Results
Demographic data
The 99 patients included 52 females (52.5%) and 47 males (47.5%).
Patients were subclassified into age groups. There was 1 patient (1.01%) aged 1 to 4 years, 1 patient aged 5 to 9 years, 3 patients (3.03%) aged 10 to 14 years, 6 patients (6.06%) aged 15 to 19 years, 26 patients (26.3%) aged 20 to 24 years, and 62 patients (62.6%) aged 25 to 29 years.
Ninety patients (90.9%) were white and 8 (8.1%) were black. The race of 1 patient (1.01%) was not specified.
Tumor location
Sixty-seven patients (67.7%) had a tumor at the level of the glottis, 18 (18.2%) had a supraglottic tumor, 3 (3.03%) had a subglottic mass, and 2 (2.02%) had a carcinoma of the laryngeal cartilage (figure 1). Of the 9 remaining patients, 6 (6.06%) had a carcinoma of the larynx not otherwise specified (NOS), and 3 had an overlapping lesion.
Type of cancer
Most patients—80 (80.8%)—had an SCC. Among the rest, 3 each had embryonal rhabdomyosarcoma, small-cell carcinoma, and synovial sarcoma; 2 each had Kaposi sarcoma, verrucous carcinoma, and fibrosarcoma; and 1 each had mucoepidermoid carcinoma, adenoid cystic carcinoma, papillary carcinoma, and carcinoma NOS.
Survival
With one exception, 5-year relative survival was fairly good across all age groups (figure 2, A). In fact, the SEER 17 survival data were better than the survival data in the SEER 11 database, which covers the period from 1992 through 1999 (figure 2, B). The one exception to the good SEER 17 outcomes was seen in the 15- to 19-year-old group, whose 5-year relative survival rate was only 60.1%. Moreover, this age group also had the lowest survival (66.8%) amongpatients with the most common form of laryngeal cancer, glottic cancer (figure 3). Finally, this age group also had the lowest survival rate in the SEER 11 database (50.1%). The reason for the low rates in this age group is unknown.
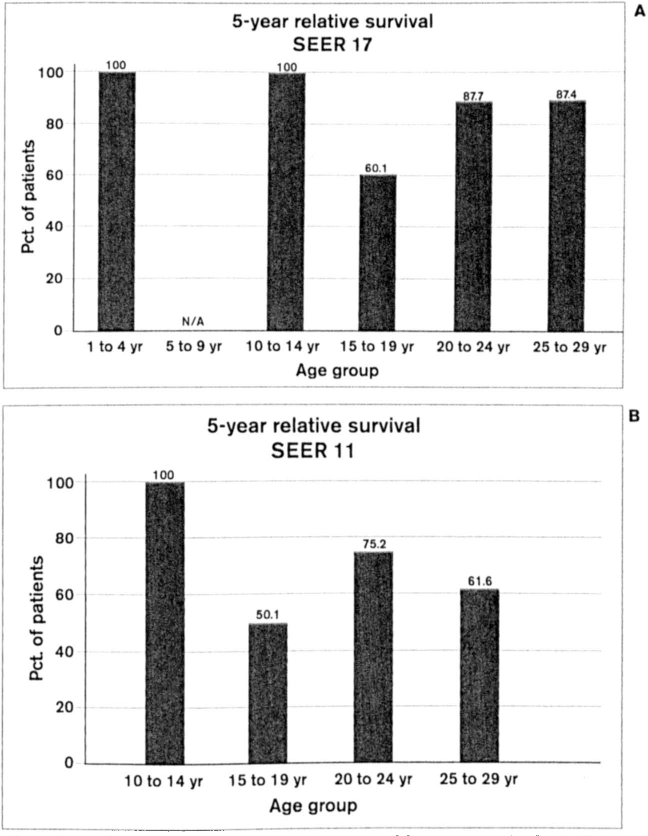
A: Chart shows the 5-year relative survival by age group in the SEER 17 database. (Survival data on the 1 patient in the 5- to 9-year-old group were not available.) B: By comparison, 5-year relative survival among the four older age groups in the earlier SEER 11 database is somewhat lower. (Data on the two younger groups were not available.)
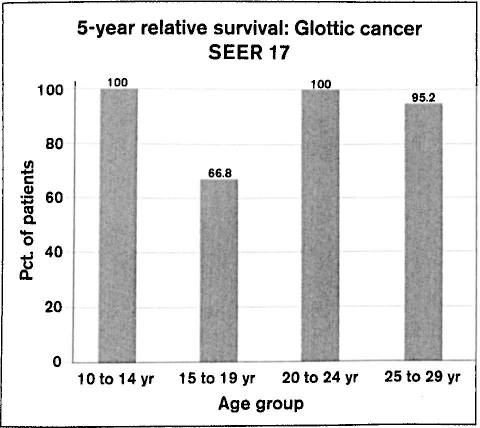
Chart shows the 5-year relative survival for patients with glottic cancer by age group in the SEER 17 database.
Discussion
Studies of laryngeal cancer in young patients have been hampered by small patient numbers (owing to its rarity in this age group) and short follow-up periods. Use of the NCI's SEER database is helpful because it contains data on a large group of young laryngeal cancer patients with long-term follow-up.
There are distinct differences in the presentation of laryngeal carcinoma in children and adults. Recurrent respiratory papillomatosis has a great predilection for the larynx, and it is the most common neoplastic disease to affect this structure in the pediatric population. In contrast, adult-onset papillomatosis is a sexually transmitted disease that preferentially affects men by a margin of approximately 3 to 2.7,25,26
Hoarseness is the heralding symptom of laryngeal papillomatosis, although some children do not present until they have become completely aphonic or have developed a life-threatening airway obstruction. 27 Indeed, most children present with extensive disease. 27 In some cases, diagnosis is delayed because symptoms are attributed to voice abuse, voice changes during puberty, or recurrent upper respiratory tract infections. The consequences of delayed diagnosis highlight the importance of an adequate visualization of the larynx in children who present with dysphonia or other symptoms suggestive of laryngeal pathology.
In 1982, Carniol and Fried in Massachusetts reported their review of more than 2,700 patients with carcinoma of the larynx or pharynx who had been admitted for treatment from 1965 through 1978. 7 Of these, only 6 patients were younger than 20 years, and only 3 were aged 20 to 29 years. The survival rate of these younger patients was equal to that of the entire population.
Also in 1982, Newman and Byers in Texas reported their series of 33 patients younger than 35 years (median: 29) who had presented with SCC of the larynx from 1947 through 1980. 28 Most of these cancers were localized to the vocal folds, and most were in an early stage and were successfully treated with conventional radiation therapy. The more advanced cancers (T3) were treated with sequential surgery and radiotherapy. The survival rate among the patients with early-stage disease (81%) compared favorably with that seen in studies of patients of all ages.
In Belgrade (in what was then Yugoslavia), Petrović et al studied a group of 988 patients who were treated surgically for laryngeal carcinoma from 1976 through 1988. 29 Of this group, 61 patients were younger than 40 years. There was no statistically significant difference in 5-year survival rates between the younger group and the entire group as a whole (83.61 vs. 68.32%; p > 0.05).
Finally, Albright et al published the first study to focus primarily on second malignancies. 30 They obtained information from the NCI's SEER database on 364 patients with laryngeal SCC and determined that patients younger than 40 years were significantly less likely than their older counterparts to develop a second malignant neoplasm during a similar length of follow-up.