
Abstract
Head movement should create a transient pressure imbalance across the membranous inner ear. We used basic concepts of fluid dynamics to develop a theoretical model of the inner ear. According to this model, two contiguous fluidic systems—the perilymphatic system and the endolymphatic system—are in hydrostatic equilibrium across a compliant membrane. Our model demonstrates that changes in resistance or compliance in one system results in a transient distortion of the membranous inner ear until equilibrium between the two systems is restored. The concept of hydrodynamic pressure changes in the inner ear has received little attention, but it may represent a new approach to understanding the inner ear and treating inner ear diseases.
Introduction
While some cases of vertigo are easily diagnosed and treated, others present a challenge. New approaches to understanding the inner ear should be explored to help us better manage the challenging cases. We have developed a theoretical hydrodynamic model of the inner ear that may be useful in this regard.
Two proposed causes of vertigo are canalithiasis and cupulolithiasis, which are often cited to explain benign paroxysmal positional vertigo (BPPV) in particular. Rajguru et al developed a three-canal mathematical model of canalithiasis to explain why the Epley canalith repositioning maneuver is so effective in treating patients with BPPV. 1 However, the fact that not all patients respond to the Epley maneuver 2 suggests that a different etiology is involved, and this led to the theory of cupulolithiasis, which holds that dislodged otoconia irritate the cupula.
Our hydrodynamic model is based on the relationship between the two fluidic systems in the inner ear: the perilymphatic system and the endolymphatic system. These two systems are separated by a compliant membrane (the membranous labyrinth), and in a steady state, they are in hydrodynamic equilibrium across this membrane. When movement occurs, however, the fluid dynamics of the systems is perturbed and a transient pressure imbalance develops. The time required for equilibrium to be regained depends on two variables: resistance to fluid flow and compliance of the system. With our theoretical model, we analyze the relationships among these variables, and we express these relationships in mathematical formulas. Our model can be applied to the study of challenging cases of vertigo, BPPV, and Ménière disease.
The hydrodynamic model
Applying basic concepts of fluid dynamics, we developed mathematical formulas that describe the relationships among various properties and actions of the perilymphatic and endolymphatic systems. Taking into consideration three variables—volume (V), time to equilibrium (t), and pressure (P)—we can mathematically define flow (F), resistance (R), and compliance (C) thus:
F = ΔV/t
R = ΔP/F
C = ΔV/ΔP
If we combine these expressions, the resulting formulas are as follows:
R = ΔPt/ΔV = t/C
t = RC
We have also expressed our theoretical model in schematic form, as illustrated in figures 1 through 4:
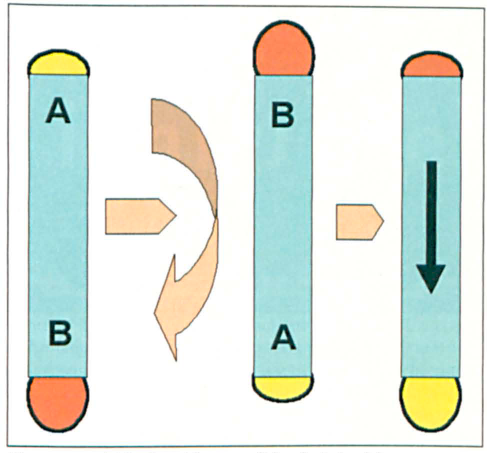
A rigid tube with caps of identical elasticity represents a fluid-filled bony and membranous labyrinth. In the figure on the left, the pressure at B is greater than the pressure at A; as a result, the cap at B becomes stretched, and it holds a greater volume than the cap at A. In the middle figure, the tube has been inverted, and the pressure drops at Band rises at A. In the figure on the right, the downward flow of pressure (arrow) leads to contraction of the cap at B and expansion of the cap at A.
In figure 1, a rigid tube with elastic caps represents a fluid-filled bony and membranous labyrinth.
In Figure 2,
resistance is applied to the system. Resistance expressed as tube narrowing is introduced into
the system. As a result, when the tube is inverted, the downward
flow of pressure is slowed. In the figure on the right,
thepressure within the tube is in equilibrium, but the time
required to achieve equilibrium was longer than the time
required in figure 1.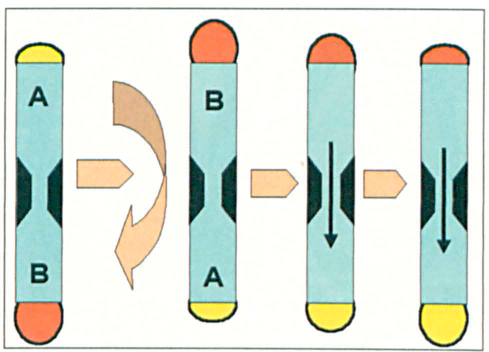
In figure 3, the
two fluidic systems are depicted as a rigid circular tube with two segments.
Two fluidic systems representing the perilymphatic and
endolymphatic systems, which are separated by compliant
membranes at the end of each tube, are seen in equilibrium. On
the left, the pressure at A and A’ is less than the
pressure at B and B’. When the entire tube structure is
inverted, the pressure at A and A’ increases at the same
rate and the pressure at B and B’ decreases at the same
rate, and thus the system remains in equilibrium and the
compliant membranes that separate the two fluids are not
distorted.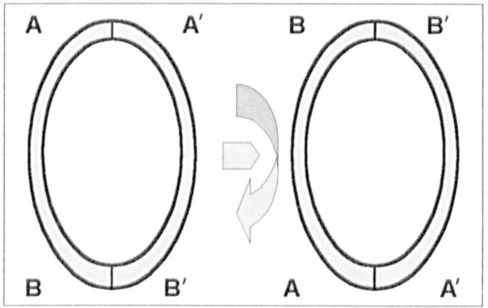
In figure 4,
resistance is added to one of the segments. Resistance is introduced into one of the tubes. When the
structure is inverted, the pressure at A increases more rapidly
than the pressure at A’, and the pressure at B decreases
more rapidly than the pressure at B’. As a result, a
brief pressure differential occurs across the top and bottom
membranes and they are distorted. Over time, the two systems
eventually regain equilibrium (t = RC).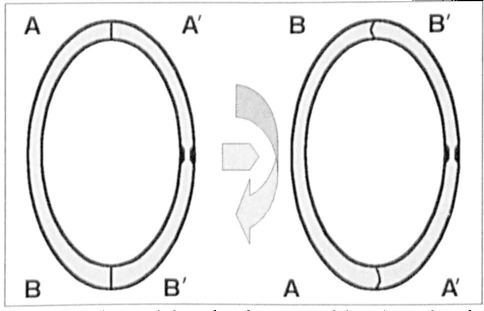
Maintenance of overall system equilibrium across the membranous labyrinth requires that the RC products of both the perilymphatic (p) and endolymphatic (e) systems be equal—that is: Rp Cp = ReCe. A change in any of these four factors (Rp, Cp, Re, and Ce), such as an anatomic variation or change in viscosity, can result in a transient overall system imbalance and distortion of the membranous labyrinth in the inner ear. Anatomic variations may include the distortion of the membranous labyrinth in Ménière disease, an enlarged vestibular aqueduct, and even dislodged otoliths; in the latter case, the fluid dynamics model complements current theories of BPPV.
Discussion
The application of basic physical concepts of hydrostatic pressure may play an important role in understanding the inner ear and may augment current theories of inner ear disease. Groen 3 and Van Buskirk et al 4 separately developed torsion-pendulum models of the inner ear in which endolymph provides inertia and viscous drag and the cupula provides the restoring stiffness. In these theoretical models, the membranous semicircular canal acts as a hollow torus in which the angular displacement of the endolymph is related to the angular acceleration of the head. This system functions like a damped torsion pendulum. Hain et al mathematically simulated episodes of canalithiasis when otoconia fell from different positions. 5 In a guinea pig model, pressure changes in the cranium, ear canal, and middle ear have been shown to lead to pressure changes in the inner ear. 6 ‘ 7 A model involving the use of high-resolution magnetic resonance imaging (MRI) of temporal bones may be useful since studies show that MRI scans can provide a foundation for developing diagnostic criteria for inner ear disease. 8
Our hydrodynamic model of the inner ear provides a novel approach to understanding inner ear function. As mentioned, a change in resistance or compliance in either the perilymphatic system or the endolymphatic system may occur as a result of anatomic variations, which can affect resistance or compliance, and changes in viscosity, which will affect resistance. These changes can result in a transient distortion of the membranous inner ear.
The hydrodynamic model may help explain how symptoms of Ménière disease can be caused by obstructing lesions of the endolymphatic sac and how these symptoms are relieved by the Meniett device, an alternating pressure generator. Our model may also explain why some patients are more susceptible to BPPV and more resistant to treatment with canalith repositioning maneuvers.
In conclusion, the hydrodynamic model of the inner ear demonstrates how variations in the RC product of the two fluidic systems may contribute to inner ear dysfunction. Variations in resistance and compliance can result in a transient pressure imbalance, which might help explain the pathophysiology of conditions such as vertigo, BPPV, and Ménière disease. Future directions include constructing a physical model that can be modified by manipulating the resistance in the endolymphatic or perilymphatic system or by adding canaliths to the system.