
Abstract

Figure. Otoscopy of the left ear shows the dissection of the incus by the tympanic cord. Both fragments are in situ. An epitympanic retraction with a cholesteatoma sac is present.
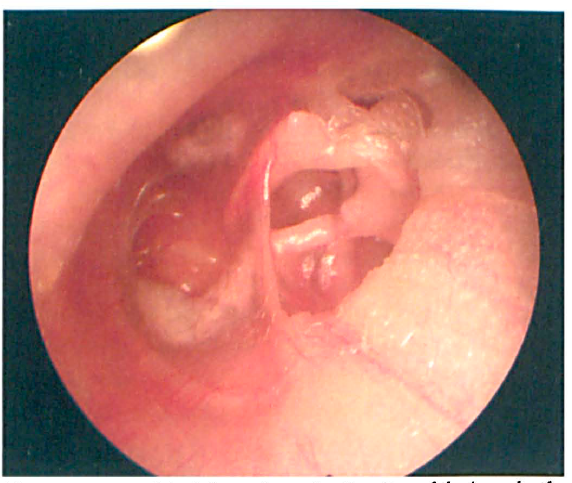
A 16-year-old girl presented with a long history of progressive bilateral hearing loss. She denied otorrhea, otalgia, and vertigo. Examination revealed bilateral pathologies with acquired cholesteatoma of the pars flaccida portion of the right tympanic membrane. In the left ear, besides adhesions and retractions, a dissected long process of the incus could be observed (figure). Findings on audiometry were consistent with a conductive hearing loss bilaterally, with an air-bone gap of 40 to 60 dB. Inner ear function was normal bilaterally.
Cholesteatomas often present with fetid otorrhea, but in this case, progressive hearing loss secondary to poor air conduction was the only presenting symptom.
Chronic inflammation can lead to erosion and necrosis of previously stable and healthy structures, as occurred in our patient, resulting in a dissection of the incus by the tympanic cord.