
Abstract
Epiphora has traditionally fallen under the purview of ophthalmologists. However, owing to the development of endoscopic dacryocystorhinostomy, this condition has been increasingly observed in otolaryngologic practice. We report the case of a woman with a 4-month history of right epiphora and dacryocystitis. Nasal endoscopy revealed the presence of a tumor at the inferior meatus. Histopathologic examination of a biopsy specimen identified the tumor as an oncocytoma. Surgical excision via a lateral rhinotomy approach was performed. At 3 years postoperatively, the patient was disease-free. Lacrimal sac and nasolacrimal duct tumors are rare, but they should be considered as a possible etiology in patients with acquired epiphora because most of these tumors are malignant.
Introduction
Acquired epiphora is a common condition caused by chronic inflammation and fibrosis of the lacrimal sac and/or nasolacrimal duct. In rare cases, nasolacrimal obstruction can be caused by a tumor. 1 Some lacrimal tumors are benign, but most are malignant. We describe a case of nasolacrimal duct obstruction caused by a benign tumor (an oncocytoma).
Case report
A 92-year-old woman was referred to our Department of Otolaryngology–Head and Neck Surgery for evaluation of epiphora, nasal obstruction, trifling epistaxis, and an abscess in the right lacrimal sac that had arisen 4 months earlier. Three years prior to presentation, she had undergone drainage of an abscess in the same sac at another hospital; the scar from that procedure was visible on the lower eyelid. Her medical history was free of allergy, chronic sinusitis, and rhinologic pathology.
Ophthalmologic examination confirmed the epiphora and the abscess in the area of the right lacrimal sac. It also revealed bilateral cataract, normal ocular mobility, and a right and high displaced right eye with no exophthalmos. No metastatic cervical adenopathy was found on palpation. On nasal endoscopy, a friable mass was observed at the inferior meatus. Computed tomography (CT) revealed that the tumor extended to and filled the entire length of the right nasolacrimal duct, from the orbit to the inferior meatus. No extension to the sinuses or orbital walls was seen (figure 1). A biopsy of the inferior meatus was obtained, and histologic analysis identified the mass as an oncocytoma (figure 2).
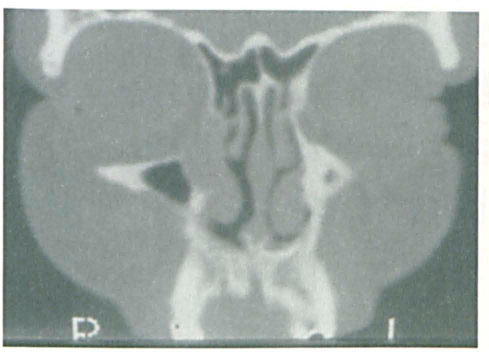
Coronal CT demonstrates the extension of the tumor in the right nasolacrimal duct from the orbit to the inferior meatus.
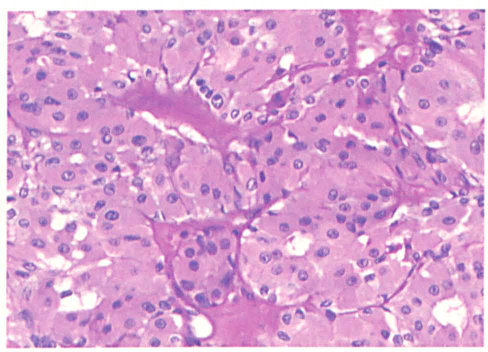
On histopathology, clusters of oncocytes with prominent granular eosinophilic cytoplasm, a centrally placed nucleus, and a single nucleolus are separated by and surrounded by capillaries. Small lumina are often apparent in the centers of the clusters.
The patient was treated with a complete surgical resection of the lacrimal sac and nasolacrimal duct. The medial and lateral walls of the maxillary sinus were removed via a lateral rhinotomy. Pathologic examination of the surgical specimen confirmed an oncocytoma of the nasolacrimal duct with free margins. At follow-up 3 years later, no evidence of recurrence was detected.
Discussion
Epiphora is considered a banal symptom that has traditionally been seen in ophthalmologic practice. It has become more commonly encountered in ENT practice since the advent of endoscopic sinonasal surgery, which has allowed a greater number of otorhinolaryngologists to perform dacryocystorhinostomy.
Tumors of the lacrimal sac and nasolacrimal duct are rare. A review of case reports and limited series that have been reported in the literature revealed that most of these tumors (75 to 90%) are malignant.2–5 Oncocytomas are also rare. These benign tumors account for 3.5% of all lacrimal neoplasms, 6 and only about 20 cases have been reported.7-10
Clinically, the presence of some specific signs can be useful in diagnosing tumors of the lacrimal sac and nasolacrimal duct. These signs include bloody reflux, epistaxis, and a noncompressible mass above the medial canthal tendon.4,11,12 However, the most important element required for the diagnosis is clinical suspicion. 4 When symptoms are uncommon or in cases of dacryocystorhinostomy failure, radiologic examinations should be routinely performed.
CT may show a tissular lesion of the lacrimal sac and nasolacrimal duct with no bony extension. Magnetic resonance imaging (MRI) can help distinguish tumors (variable thickness with heterogeneous gadolinium enhancement) from pyoceles (content looks like fluid in the thin side with homogeneous gadolinium enhancement). CT and MRI can also help clarify the extent of the soft-tissue density, which is useful in determining the surgical approach. 13
The diagnosis is often based on the results of a histologic examination of a biopsy or surgical specimen. Histology will show large cells with abundant granular eosinophilic cytoplasm and a round to oval paracentral nucleus. 8
Complete surgical excision is the treatment of choice because malignant transformation has been reported (3 cases).1,14 Most malignant tumors are diagnosed at an advanced stage, so a major excision is sometimes required to remove tumor extension to the sinuses and/or orbit. 5 When the nasolacrimal duct is involved, a lateral rhinotomy allows for a wider excision.
Adjuvant radiation therapy has been shown to reduce the recurrence rate of malignant epithelial tumors, 15 but no adjuvant therapy has been recommended for benign tumors. Hornblass et al asserted that radiotherapy is contraindicated as a treatment for benign tumors because it might result in a malignant transformation. 11
Oncocytomas are rare in head and neck pathology. When they do occur, they usually involve the salivary glands. Even so, oncocytomas account for less than 3% of all salivary gland tumors; most of these (80 to 90%) occur in the parotid gland. Head and neck oncocytomas occur equally in men and women, and their peak incidence occurs during the seventh to ninth decades of life. 16 The diagnosis is based on pathologic examination. The prognosis following surgical excision is excellent. 16 Some authors have reported that oncocytomas of the minor salivary glands, nasal cavity, and sinuses are more aggressive. 17 A few rare cases of malignant oncocytic carcinoma have been reported. 18
Although all acquired nasolacrimal duct obstructions do not require a simple dacryocystorhinostomy, we must keep in mind the possibility of a lacrimal sac or nasolacrimal duct tumor such as an oncocytoma whenever symptoms are not classic. The suspected diagnosis can be approached on the basis of careful clinical and radiologic examinations and confirmed by histologic examination. A wide surgical resection is required because of the possibly aggressive nature of any given tumor.
Footnotes
Acknowledgment
The authors thank Richard Medeiros, a medical editor at the Rouen University Hospital, for his valuable help in editing the manuscript.