
Abstract
Cerebellopontine angle (CPA) ganglionic hamartomas are rare. We present a case of a 49-year-old woman who presented with left-sided hearing loss of more than 4 years’ duration and vertigo since childhood. Magnetic resonance imaging revealed a mass on the intracanalicular segment of cranial nerve VIII on the left side, consistent with acoustic schwannoma. She opted for observation of the tumor. The patient returned 21 months after the initial evaluation with new-onset left facial weakness. At this time, a working diagnosis of facial nerve neuroma was made. The lesion was excised, and pathology confirmed a diagnosis of left-sided CPA ganglionic hamartoma. Otolaryngologists should be familiar with this uncommon tumor and include it in the differential diagnosis of CPA lesions.
Introduction
Acoustic neuromas account for 90% of cerebellopontine angle (CPA) lesions, with the other major primary tumors being meningiomas (3%), primary cholesteatomas (2.5%), and facial nerve schwannomas (1%). 1 Other CPA lesions are rare, with ganglionic hamartomas being among the rarest; only 11 cases have been reported.2-10 We present a case of CPA ganglionic hamartoma in which the lesion was diagnosed preoperatively as a probable facial nerve neuroma.
Case report
A 49-year-old woman presented with left-sided hearing loss of more than 4 years’ duration, occasional tinnitus, and vertigo. She had experienced vertigo since the age of 12 years, but the frequency of episodes had increased during the preceding year. She had no abnormal findings on physical examination.
All cranial nerve function was normal bilaterally with the exception of cranial nerve VIII. An audiogram revealed normal hearing on the right and mild to moderate sensorineural hearing loss (72% speech discrimination) on the left. Brainstem-evoked-response audiometry showed no signs of retrocochlear pathology. A 22% reduced left vestibular response and right-beating nystagmus were found on electronystagmography.
Electroneuronography (ENoG) demonstrated a 78% decreased facial response on the left. Probably because of the thickness and resiliency of the facial nerve, we have seen ENoG results showing as much as an 85% decrease in some patients who still had clinically normal facial function. Magnetic resonance imaging (MRI) revealed an enhancing 5 × 3-mm mass on the intracanalicular segment of cranial nerve VIII on the left, consistent with acoustic schwannoma (figure 1). Observation was recommended initially, with audiograms every 3 months and MRI every 6 months.
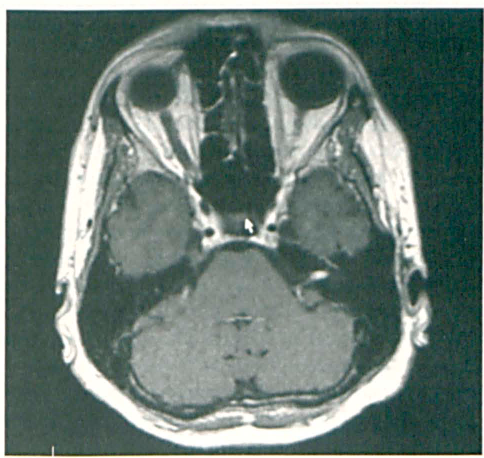
T1-weighted MRI demonstrates a 5 × 3-mm enhancing intracanalicular mass.
The patient returned 21 months after her initial evaluation with new-onset facial weakness on the left. The weakness was most prominent in her upper lip and nasolabial crease, and it was most pronounced when she spoke. Physical examination revealed a House/Brackmann grade I-II/VI palsy of the left facial nerve. Repeat ENoG revealed no change in electrical function when compared to the previous study. A working diagnosis of facial nerve neuroma was made, although the patient was informed that acoustic neuroma or other pathology could not be excluded.
The patient underwent a translabyrinthine excision of the lesion, which was located on a superior vestibular nerve, extending inferiorly to the area of the cochlear modiolus. The lesion was reflected medially, and an incision was made in the cerebellar dura. The lesion was larger than recognized on MRI and was followed to its medial extent of a few millimeters into the posterior fossa. Facial nerve function was preserved, but a House/Brackmann grade I–II/VI palsy was still evident 5 months postsurgically. Compression of the facial nerve by the tumor in the superior compartment of the internal auditory canal explained the preoperative and postoperative facial paresis.
Histologic evaluation of the lesion demonstrated normal myelinated axon fascicles separated by fibrous stroma and adipose tissue. Along the axons were multiple foci of mature ganglion cells with well-formed Nissl bodies in the peripheral cytoplasm. Foci of less mature ganglion cells also were identified. Immunohistochemical staining for synaptophysin, neurofilaments, and S-100 protein demonstrated a normal pattern of immunoreactivity. Furthermore, immunohistochemical staining for the tumor-proliferation marker MIB-1 revealed no positive cells. Based on the histologic examination, a diagnosis of left CPA ganglionic hamartoma was established (figure 2).
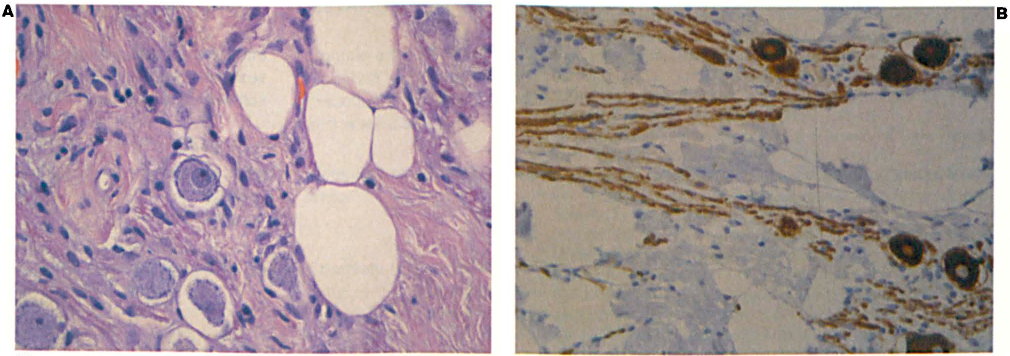
Low-power view (
Discussion
The term hamartoma refers to a mass of abnormally arranged cells typically found in the surrounding tissue. 11 Such a lesion is believed to be a result of aberrant differentiation of tissue during embryonic development. Intracranial hamartomas can be subdivided into lipomatous and glioneuronal types. Lipomatous hamartomas are also known as lipomas and constitute less than 0.14% of CPA neoplasms. 4 Glioneuronal hamartomas are much rarer, with only 11 cases reported in the literature before the present case.2–10
Of the 11 patients whose cases were described in the previous reports, 2 were asymptomatic; the neoplasm was an incidental finding on autopsy in those 2 patients and in 1 additional patient (table). The remaining 9 patients presented with hearing loss on the affected side. Even when small, these firm tumors can compress cranial nerves VII and VIII and produce symptoms. Other symptoms include vertigo/disequilibrium, facial palsy, tinnitus, and headache.
Complete tumor excision was performed in most cases, with 1 partial resection to preserve the cochlear nerve. In 3 cases, partial resection of cranial nerves was performed to allow complete excision of the tumor. In one of these cases, the cochlear nerve was sacrificed; in another both the cochlear and vestibular nerves were sacrificed; and in the third case, the cochlear, vestibular, and facial nerves were sacrificed. In the case in which partial resection of the tumor was performed, the patient was doing well 1.5 years postoperatively, with no tumor regrowth. One patient who underwent complete tumor resection with preservation of cranial nerves suffered from facial nerve palsy, which improved over the first postoperative year. No other complications were reported.
Table. Previously reported cases of cerebellopontine angle hamartoma
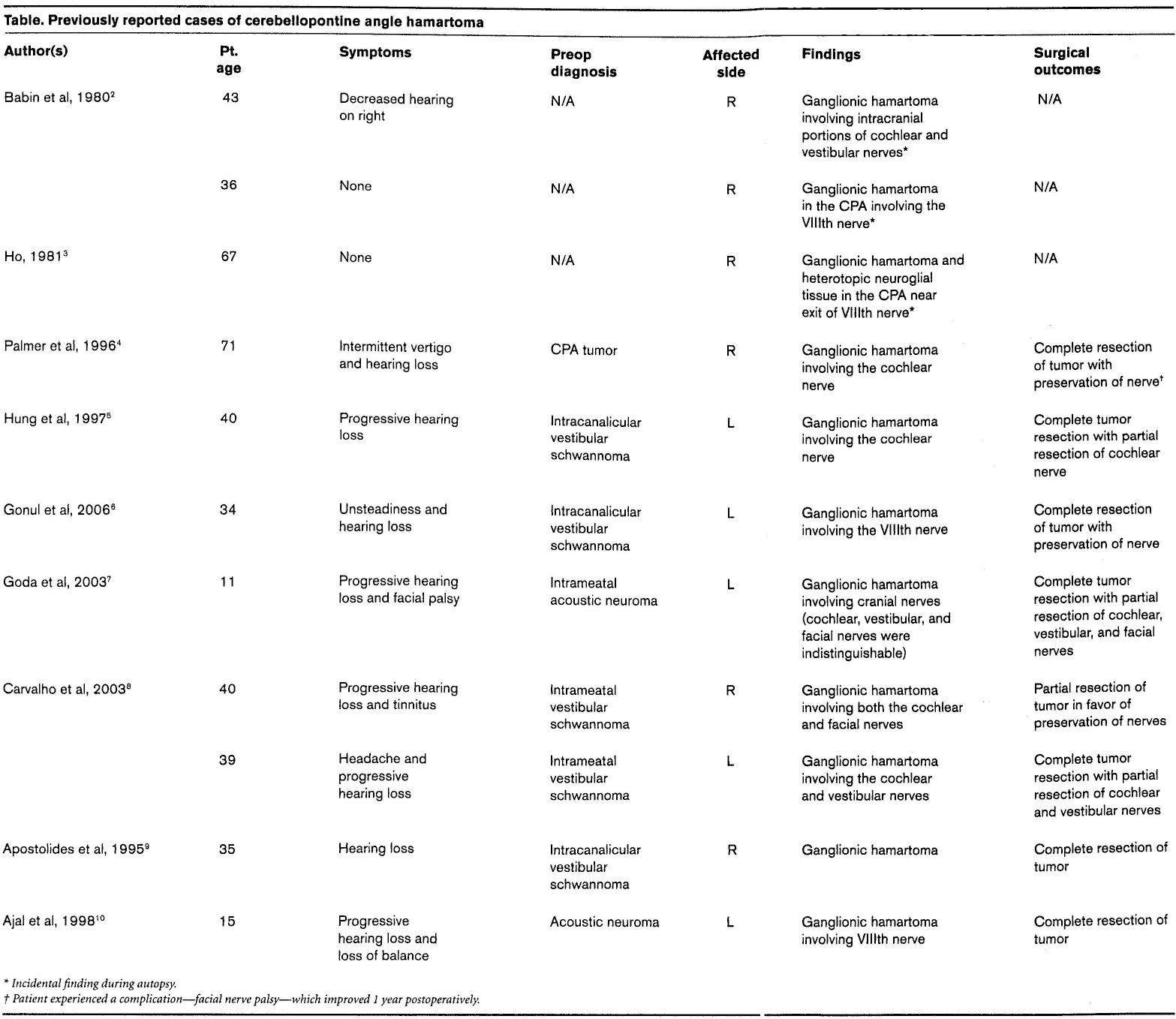
Incidental finding during autopsy.
Patient experienced a complication—facial nerve palsy—which improved 1 year postoperatively.
Our patient presented initially with left-sided hearing loss, vertigo, and tinnitus with subsequent development of facial palsy. The tumor was situated on the superior vestibular nerve, which was sacrificed in favor of complete resection of the tumor. The postoperative course was uneventful, with no complications.
Complete resection of these tumors is considered curative; however, only limited data are available regarding recurrence or regrowth following partial resection. In asymptomatic patients, surgical excision of the tumor may not be advisable because of the risks associated with resection, provided an accurate diagnosis can be established preoperatively, which is not common. 4 In the 11 previously reported cases and in the present case, no patient was accurately diagnosed preoperatively. Our patient was initially diagnosed with an acoustic neuroma, and the working diagnosis was changed to facial nerve neuroma when the studies were completed and her facial paresis occurred, but other pathology could not be excluded. Because of the progressive symptoms, surgical excision was deemed appropriate.
Ganglionic hamartomas remain challenging to differentiate preoperatively from other neoplasms of the CPA.