
Abstract

A 21-year-old woman presented with a giant hairy nevus on the right side of her face (figure 1). After conducting a detailed physical examination, we described the various options that were available for its removal and for repair of the surgical defect. The patient could not afford tissue expansion surgery, so she opted to undergo simple excision of the nevus and surgical repair with a fasciocutaneous reverse radial artery forearm flap. This flap is similar to a radial forearm free flap; the difference is that with the reverse flap procedure, the radial artery pedicle is kept intact until a second stage is performed, analogous to a paramedian forehead flap.

The giant hairy nevus is seen at presentation.
After we explained the procedure, its complications, and the expected results, the patient provided informed consent. The preoperative surgical planning included an ulnar artery patency test (Allen test). The flap donor and recipient sites were selected, and templates were made. The range of motion of both the arm and wrist on the side of the donor site was evaluated.
With the patient under general anesthesia, the nevus was excised and a reverse radial forearm flap was harvested (figure 2, A) and sized to fit the dimensions of the facial template (figure 2, B). The large surgical defect of the donor site required a split-thickness skin graft.
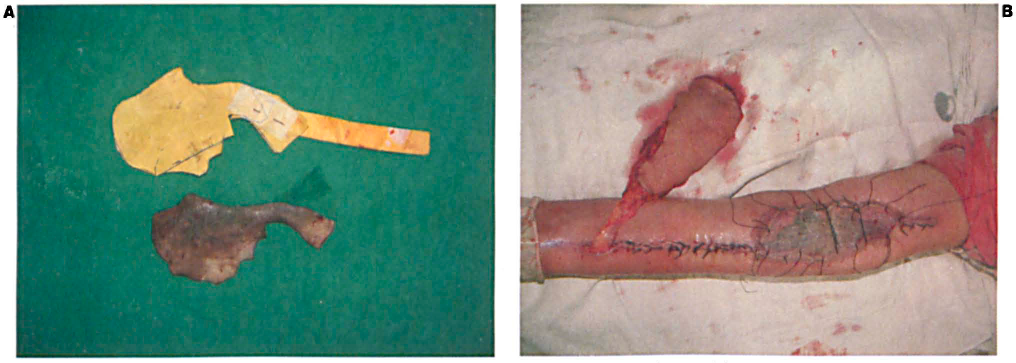
The harvested forearm flap (
The patient's immediate postoperative period was uneventful (figure 3). At 2 weeks postoperatively, the compromised radial artery test (flap delay) confirmed flap survival, and then the flap was detached from its pedicle. As expected, the patient had experienced a mild amount of difficulty with arm movement during the 2 weeks after surgery (flap delay). Her movement reverted to normal following physiotherapy. At subsequent follow-ups, the patient underwent four additional surgical corrections under local anesthesia for excision of the remaining nevus. One year after the initial surgery, the patient was fully satisfied with the cosmetic result (figure 4).

Immobilization of the forearm, with positioning the patient's arm over her head with plaster and bandage, is crucial for flap viability.

One year after the initial surgery, the cosmetic outcome is satisfactory.
In 1981, Yang et al in China became the first to describe the radial artery forearm free flap, which is also known as the Chinese flap. 1 At around the same time, Lu 2 and Stock et al 3 described the use of the reverse radial artery forearm flap. Limitations of this free or pedicle flap include sacrifice of the radial artery and morbidity at the donor site and adjacent joints, particularly in older patients. For this reason, all patients who undergo this procedure should be tested to ensure a patent palmar arch and ulnar artery. Because a pedicle radial artery forearm flap requires immobilization of the arm, it is contraindicated in patients with joint diseases.
The reverse radial artery forearm flap is usually reserved for emergency trauma cases involving soft-tissue defects of the hand because it is a one-stage procedure and microsurgical experience is not needed. This flap is also used as a perforator flap to save the radial artery. 4 This technique results in a longitudinal scar at the donor site, which is much more acceptable to patients than many other types of scar.
In head and neck reconstruction, a radial artery forearm flap is usually preferred as a free flap, but this procedure requires expertise in microvascular surgery. This flap is commonly used in the reconstruction of oromandibular, 5 pallatomaxillary, 6 and preauricular and temporal bone defects, 7 as well as in phallus reconstruction. 8 The free radial forearm flap procedure requires more surgical time than some similar procedures, and postoperative care is crucial to avoid flap necrosis, the rate of which one recent study found to be approximately 9%. 5 Compared with free flaps, pedicle radial artery forearm flaps require less surgical time and expertise, but they involve a two-stage procedure and they require joint immobilization for 2 to 3 weeks.
The different modalities that are used to reconstruct defects after excision of giant hairy nevi include tissue expansion, placement of local flaps, serial excision with full-thickness grafting, and use of a dermal regeneration template (Integra).9–11 Tissue expansion is the preferred method for the management of hairy nevi of the head and neck, and serial excision is preferred for the extremities. 9 However, tissue expansion has several disadvantages, including a long treatment period (∼3 to 6 wk) after insertion of the tissue expander. Such a long period can be unacceptable to patients from a cosmetic and social standpoint, as well as being uncomfortable. Moreover, tissue expanders are expensive, and some patients cannot afford them. In these cases, the pedicle reverse radial forearm flap is a reasonable option. Results with this flap are acceptable in terms of color match and negligible scarring at the donor site (figure 4).