
Abstract
Teratocarcinosarcoma(TCS) is a rare malignant neoplasm that has a predilection for the sinonasal cavities. It exhibits a highly invasive behavior and a propensity for recurrence and dissemination. Despite aggressive surgical resection and adjuvant radiation therapy, the prognosis is very poor. 1
Conventional cross-sectional imaging is helpful but limited in the comprehensive staging and post-therapeutic surveillance of TCS. In this article, the author describes a case in which F18-fluorodeoxyglucose–positron-emission tomography/computed tomography (FDG–PET/CT) imaging was used.
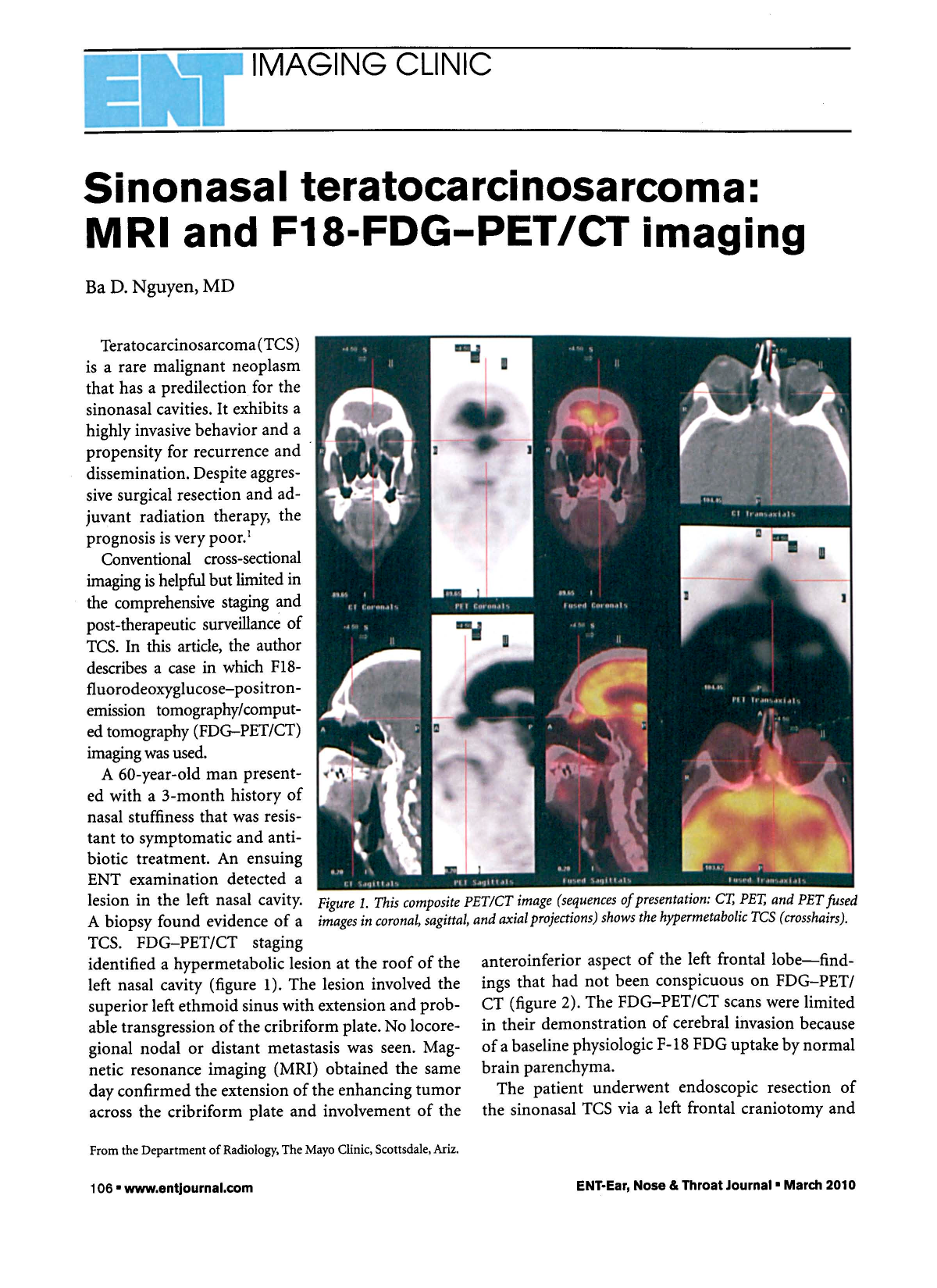
A 60-year-old man presented with a 3-month history of nasal stuffiness that was resistant to symptomatic and antibiotic treatment. An ensuing ENT examination detected a lesion in the left nasal cavity. A biopsy found evidence of a TCS. FDG-PET/CT staging identified a hypermetabolic lesion at the roof of the left nasal cavity (figure 1). The lesion involved the superior left ethmoid sinus with extension and probable transgression of the cribriform plate. No locoregional nodal or distant metastasis was seen. Magnetic resonance imaging (MRI) obtained the same day confirmed the extension of the enhancing tumor across the cribriform plate and involvement of the anteroinferior aspect of the left frontal lobe—findings that had not been conspicuous on FDG–PET/ CT (figure 2). The FDG–PET/CT scans were limited in their demonstration of cerebral invasion because of a baseline physiologic F-18 FDG uptake by normal brain parenchyma.
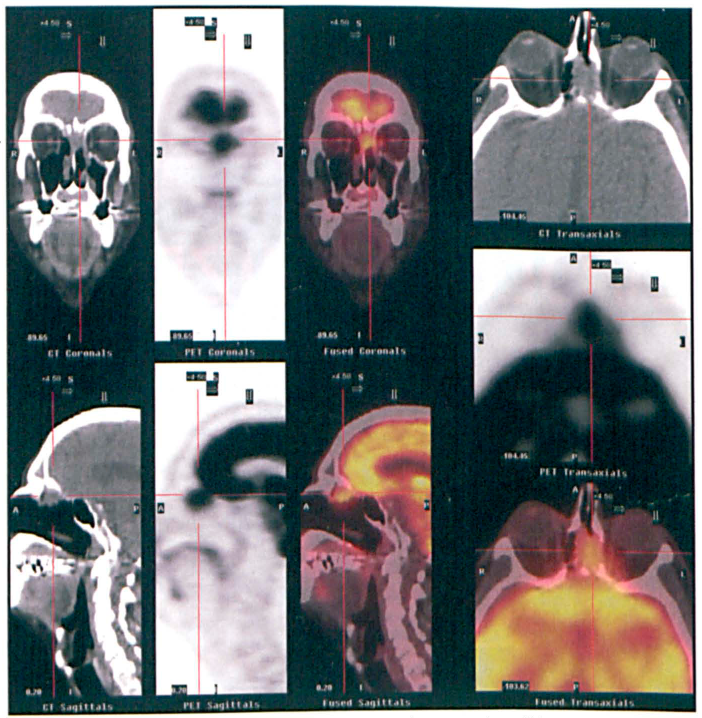
This composite PET/CT image (sequences of presentation: CT, PET, and PET fused images in coronal, sagittal, and axial projections) shows the hypermetabolic TCS (crosshairs).

Contrast-enhanced T1-weighted MRI shows the TCS (arrow) invading the anteroinferior aspect of the left frontal lobe.
The patient underwent endoscopic resection of the sinonasal TCS via a left frontal craniotomy and resection of the left frontal lobe tumor. He also received postoperative adjuvant external-beam radiotherapy. Less than 3 months after surgery, a bilateral enlarging cervical adenopathy was found on clinical follow-up. Tissue sampling revealed that the finding represented metastatic TCS. Restaging with FDG-PET/CT showed hypermetabolic TCS dissemination to cervical nodes bilaterally, the right submandibular node, the C6 vertebra, the deltoid muscle, two sites in the right lung, the liver, the right iliac bone, and the right sacral ala (figure 3). The patient died shortly thereafter as a result of the rapid progression of the diffuse metastases.
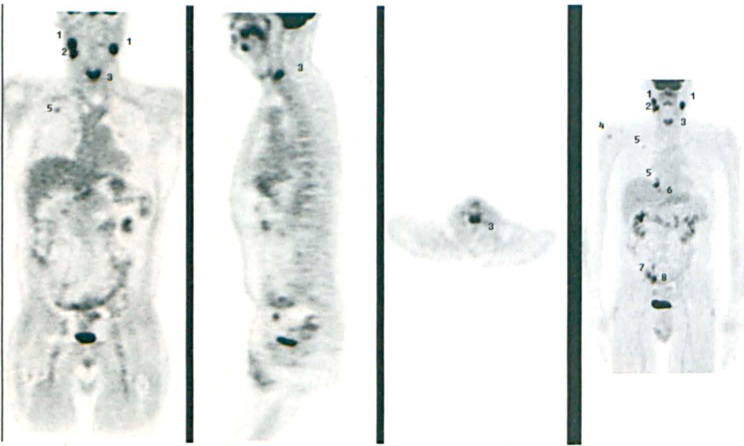
At postoperative restaging, the whole-body volumetric FDG-PET/CT shows the hypermetabolic TCS dissemination to cervical nodes bilaterally (1), the right submandibular node (2), the C6 vertebra (3), the deltoid muscle (4), two sites in the right lung (5), the liver (6), the right iliac bone (7), and the right sacral ala (8).
In view of its complex histologic architecture, TCS has also been known as malignant teratoma, blastoma, and mixed mesodermal tumor. 1 It may be mistaken for esthesioneuroblastoma because of its neuroectodermal histologic component and features of cribriform plate transgression. The diagnosis of TCS is based on the demonstration of teratoid and carcinosarcomatous features. TCS probably arises from primitive embryonic sinonasal tissue or immature pluripotential cells. It occurs almost exclusively in the sinonasal cavities; rare instances of nasopharyngeal and oral involvement have been reported. 2 The average survival is less than 2 years, and the survival rate beyond 5 years is less than 45%. 1
Even though FDG-PET/CT is limited in the initial evaluation of cerebral integrity, it can provide a comprehensive and timely detection of asymptomatic regional and distant metastases that is not readily documented by the limited field of view on CT and MRI.3,4