
Abstract
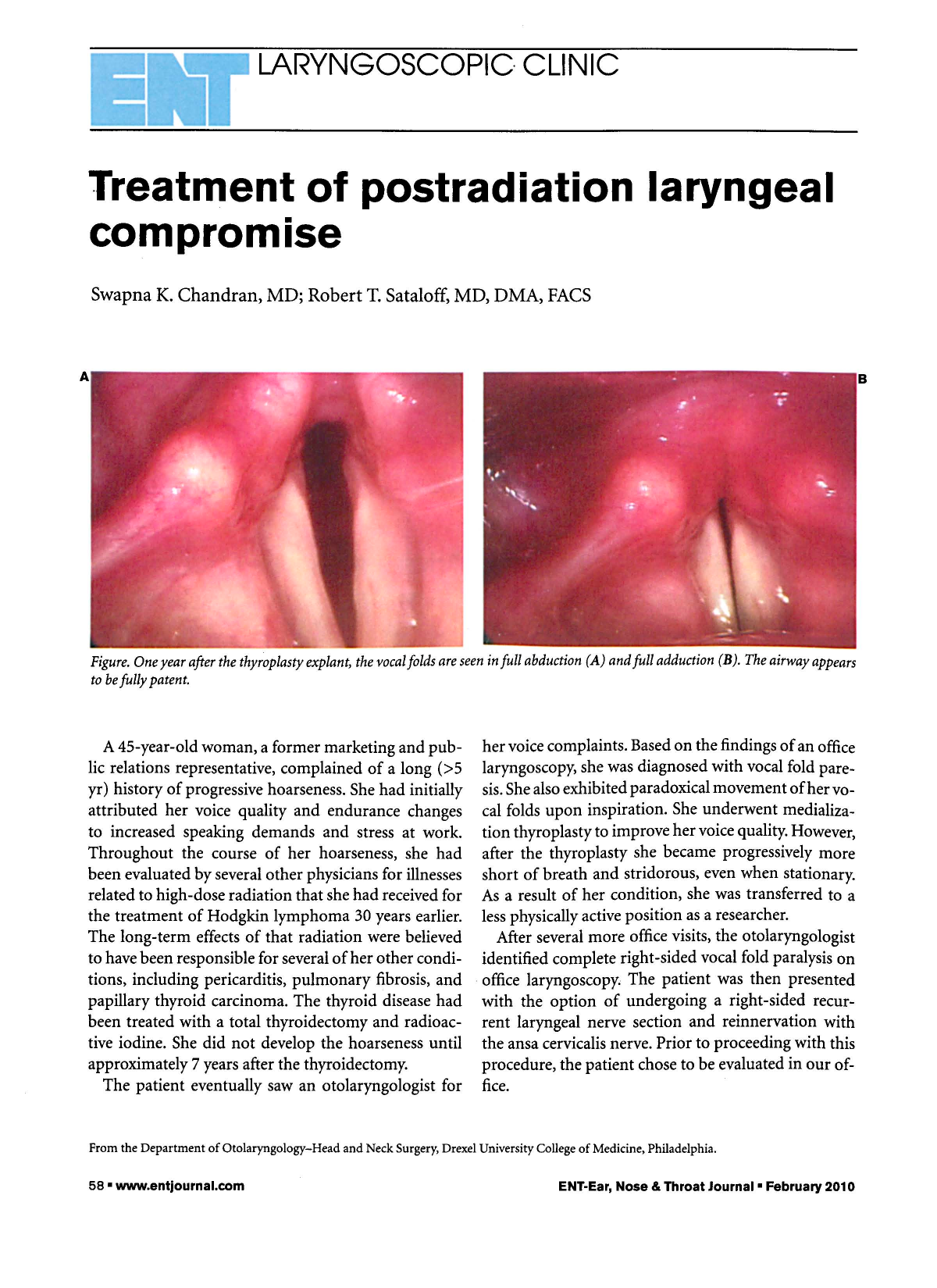
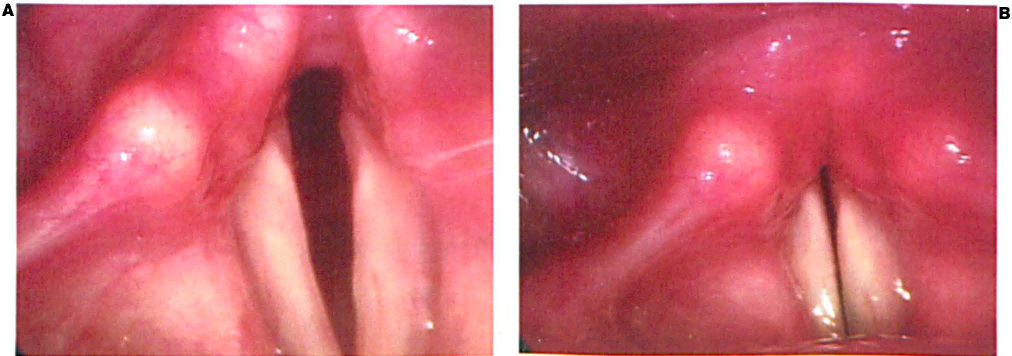
Figure. One year after the Thyroplasty Explant, the Vocal Folds are Seen in Full
Abduction (
A 45-year-old woman, a former marketing and public relations representative, complained of a long (>5 yr) history of progressive hoarseness. She had initially attributed her voice quality and endurance changes to increased speaking demands and stress at work. Throughout the course of her hoarseness, she had been evaluated by several other physicians for illnesses related to high-dose radiation that she had received for the treatment of Hodgkin lymphoma 30 years earlier. The long-term effects of that radiation were believed to have been responsible for several of her other conditions, including pericarditis, pulmonary fibrosis, and papillary thyroid carcinoma. The thyroid disease had been treated with a total thyroidectomy and radioactive iodine. She did not develop the hoarseness until approximately 7 years after the thyroidectomy.
The patient eventually saw an otolaryngologist for her voice complaints. Based on the findings of an office laryngoscopy, she was diagnosed with vocal fold paresis. She also exhibited paradoxical movement of her vocal folds upon inspiration. She underwent medialization thyroplasty to improve her voice quality. However, after the thyroplasty she became progressively more short of breath and stridorous, even when stationary. As a result of her condition, she was transferred to a less physically active position as a researcher.
After several more office visits, the otolaryngologist identified complete right-sided vocal fold paralysis on office laryngoscopy. The patient was then presented with the option of undergoing a right-sided recurrent laryngeal nerve section and reinnervation with the ansa cervicalis nerve. Prior to proceeding with this procedure, the patient chose to be evaluated in our office.
We recommended laryngeal electromyography (EMG) to confirm the vocal fold paralysis. The EMG failed to show complete paralysis of the recurrent laryngeal nerve on either side. As a result, the option of laryngeal nerve reinnervation was rejected. Instead, the patient underwent removal of her right thyroplasty implant.
At the 1-year follow-up, the patient reported less stridor. She was able to climb stairs without increased respiratory effort—an activity that she had been unable to perform prior to the procedure. She also reported better voice quality with less fatigue after working with vocal pathologists and singing voice specialists. Examination revealed good abduction and adduction (figure).
A determination of laryngeal paralysis requires both laryngoscopic visualization and electromyography. Electromyography of the distributions of both the recurrent and superior laryngeal nerves not only helps determine the severity of paresis, but it also helps guide treatment strategies.
This case illustrates a laryngeal complication of radiation therapy that was not diagnosed for many years. Caution must be exercised when performing thyroplasty in patients with reduced pulmonary function. Reduction in the upper airway size by only a few millimeters may be enough to cause respiratory difficulty. This is an example of a complicated case in which an acceptable compromise was made between pulmonary function and voice quality.