
Abstract
Unilateral sinus disease has a wide differential diagnosis. When a patient has a history of maxillary dental work on the same side as the sinusitis, a foreign entity introduced during or subsequent to the dental manipulation must he considered. We present a case of calcified maxillary cyst that was discovered at the site of a remote tooth extraction. Pathologic analysis revealed the presence of vegetable matter within the cyst. To the best of our knowledge, no case of a maxillary cyst secondary to vegetable matter has been previously reported in the literature.
Introduction
Unilateral sinus disease has a variety of causes, including dental, neoplastic, fungal, and foreign entities. Sinus disease secondary to the presence of a foreign body tends to present as unilateral sinusitis with blood-tinged or purulent foul-smelling discharge. We describe the case of a patient who presented with unilateral fullness in the maxillary sinus.
Case report
A 72-year-old man presented with a complaint of left facial fullness in the maxillary area. He denied nasal obstruction, anosmia, and nasal discharge, but he was able to express blood and purulent material through his nose with manual pressure on the area of fullness. He had received multiple courses of antibiotics from his primary care physician without resolution of the symptoms. His history was significant for multiple tooth extractions and for nasal surgery 50 years earlier that had included inferior turbinectomies.
Anterior rhinoscopy identified a firm fullness on the left inferior lateral nasal wall. The patient's facial sensation was good with no areas of numbness. He was edentulous, and his neck was supple without adenopathy. Flexible rhinoscopy revealed clear ostiomeatal units bilaterally and a bulging on the lateral nasal wall under the resected inferior turbinate. Computed tomography (CT) demonstrated a calcified wall surrounding a soft-tissue mass in the left maxillary sinus (figure 1).
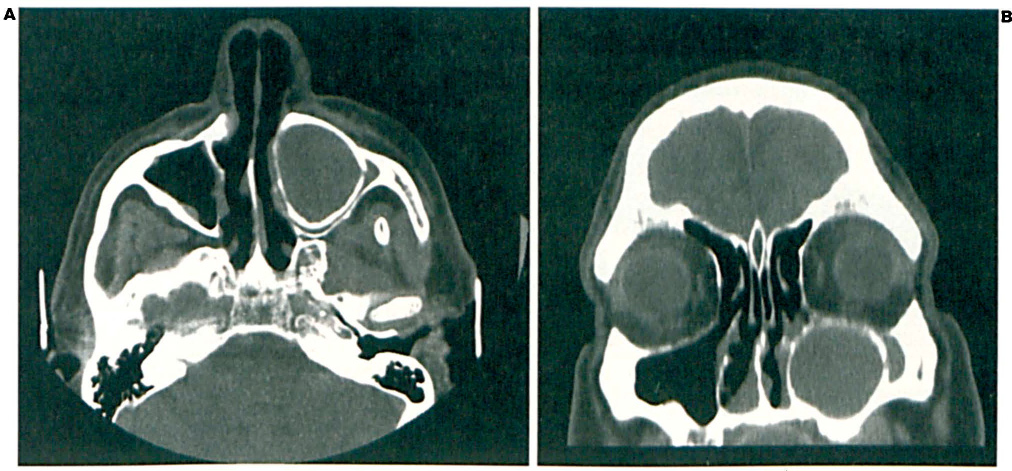
Axial (
The mass was removed via a Caldwell-Luc procedure. Periodic acid–Schiff (PAS) staining revealed that the specimen contained a small amount of vegetable matter surrounded by a calcified wall (figure 2). Neither PAS nor Gomori methenamine silver staining revealed any fungal hyphae, and fungal cultures were negative.
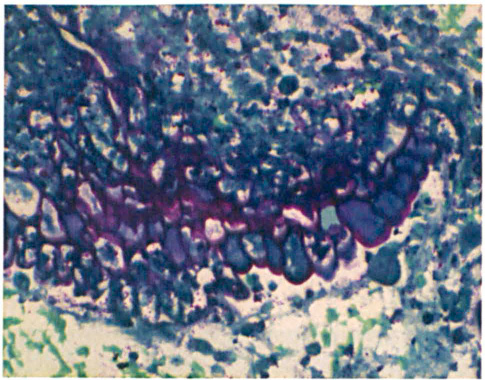
Staining of the cystcontents with PAS reveals vegetable matter with characteristic cell walls (original magnification X200).
Postoperatively, the patient developed an oroantral fistula at the operative site that was repaired without incident. At follow-up 2.5 years postoperatively, he continued to do well.
Discussion
In the case described herein, the presence of a calcified wall surrounding a soft-tissue or fluid mass on CT raised the suspicion of a benign neoplastic process. The differential diagnosis for a calcified mass in the maxillary sinus includes benign tumors (e.g., an osteoma, ossifying fibroma, or calcifying odontogenic cyst), malignant tumors (osteosarcoma), unerupted teeth, antroliths (calcified sinus “stones” that form around a central inflammatory nidus), fungal disease, radiopaque foreign bodies (bone chips or dental cement), and inflammatory cysts. Pathologic examination of the specimen in our case revealed only a small amount of vegetable matter surrounded by inflamed granulation tissue.
Fungal disease can be solely responsible for the symp- tomatology and radiographic appearance of a calcified maxillary cyst. 1 Fungal disease can also be associated with foreign bodies in the sinuses. 2 In our patient, however, PAS and Gomori stains did not reveal any fungal hyphae, and fungal cultures were negative, arguing against the presence of fungus. Calcium salt deposition in a thin layer around the granular cyst explains its radiographic appearance. Antroliths form in a similar manner, but the radiographic and pathologic hallmark of an antrolith is concentric rings of calcium and other salts rather than a thin outer shell.
It is possible that a temporary oroantral fistula formed during the extraction of one or more of our patient's teeth, allowing for the deposit of a small amount of vegetable matter into the sinus. Our patient's previous inferior turbinectomies were unlikely to have contributed to the seeding of his left maxillary sinus by an exogenous foreign body, as anatomic narrowing and obstruction rather than widening of the middle meatus is the likely result of turbinectomy. 3 To the best of our knowledge, ours is the only reported case of a maxillary cyst secondary to vegetable matter.
The Caldwell-Luc approach is the procedure of choice for the removal of complicated maxillary foreign bodies. 4 Indeed, Richtsmeier identified the presence of a foreign body as one of the top 10 reasons for the failure of endoscopic maxillary sinus surgery. 5 This may be attributable in some cases to a failure to identify and/or completely remove a foreign body at the time of surgery. In other cases, it may be attributable to seeding of the sinus with debris, bone chips, or ointments during endoscopic surgery.