
Abstract
Nonoperative management is generally accepted as a treatment strategy for nasopharyngeal cancer characterized by destruction of the skull base. Chemoradiotherapy is considered the standard of care in these cases. We report a case in which imaging studies documented the successful treatment of the patient's locally extensive nasopharyngeal carcinoma with this nonsurgical approach.
Introduction
Nasopharyngeal cancer is usually locally extensive (stage III or IV) at the time of diagnosis.1,2 Al-Sarraf et al concluded from the phase III randomized Intergroup study 0099 that chemoradiotherapy is superior to radiotherapy alone for patients with advanced nasopharyngeal cancer in terms of overall and progression-free survival. 3
At our center, we treated a case of nasopharyngeal cancer that had eroded the skull base in a patient who had undergone sectional computed tomography (CT) before and after therapy. We herein report this case in order to provide radiologic evidence of the efficacy of chemoradiation against nasopharyngeal cancer with skull base erosion. To the best of our knowledge, such evidence has not been previously published.
Case report
A 38-year-old man was seen at our hospital in September 2003 for evaluation of a left neck mass that had enlarged over 1 year's time. Cranial nerve dysfunction was not observed on physical examination. Endoscopy revealed a nasopharyngeal tumor. CT of the head and neck showed that the mass had destroyed the clivus at the skull base. CT also detected bilateral upper (level II) cervical lymphadenopathies. Histologically, the nasopharyngeal neoplasm was identified as a squamous cell carcinoma. Positron-emission tomography confirmed the absence of distant metastatic disease. The tumor was clinically staged as T3N2M0. The patients serum Epstein-Barr virus (EBV) DNA level was not initially obtained or monitored.
Concurrent chemotherapy and radiation were administered. The chemotherapy consisted of 2 cycles of cisplatin and 5-fluorouracil. Radiotherapy involved a total applied dose to the locally extensive nasopharyngeal cancer and neck adenopathies of 64 Gy in 32 fractions. In addition, 50 Gy in 25 fractions were delivered to the clinically negative lower neck. The combined therapy was completed in February 2004.
Follow-up CTs were obtained in May 2004. Comparisons of pre- and post-treatment scans documented the disappearance of the primary tumor (figure 1, A and B) and the nodal disease (figure 2, A and B), as well as reossification of the osteolytic lesion at the skull base (figure 3, A and B).
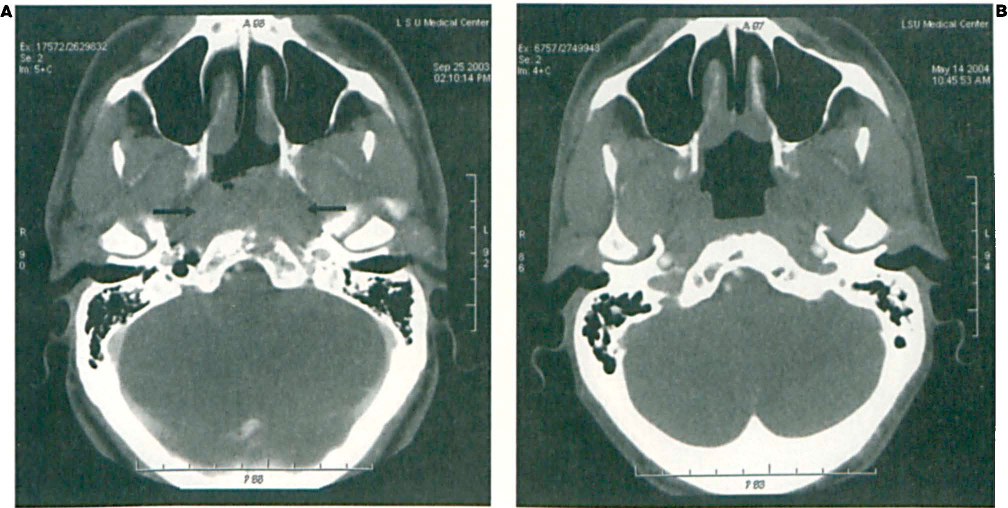
Comparison of CT Scans Obtained before (
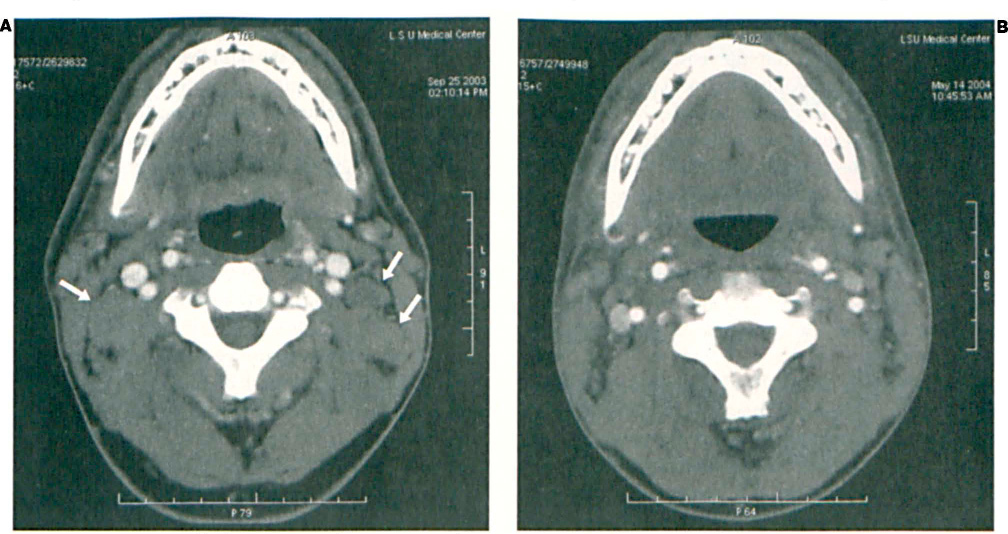
Comparison of before (
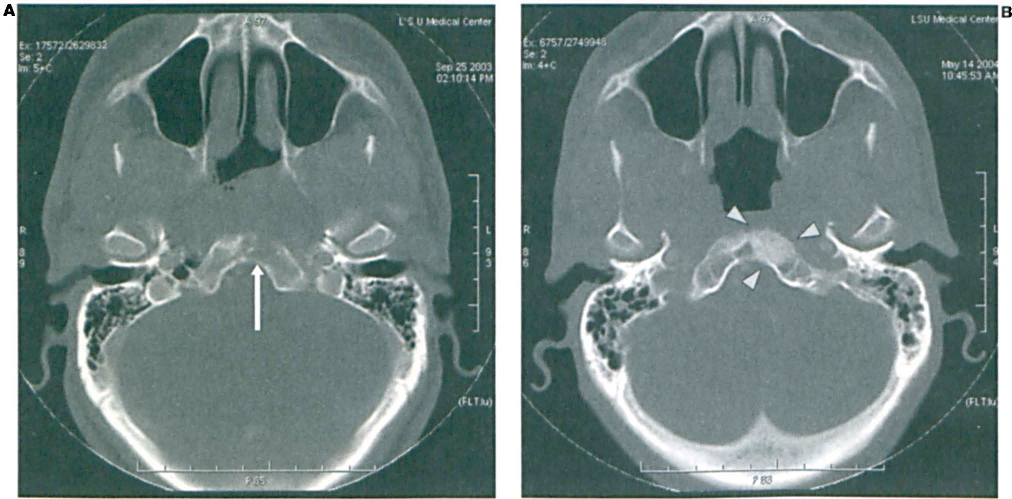
Comparison of pre-(
At follow-up in March 2009 (67 mo after diagnosis), the patient was doing well and was clinically free of tumor.
Discussion
In the United States, the annual incidence of nasopharyngeal cancer is approximately 1/100,000 population. 4 The relative lack of a barrier surrounding the nasopharynx provides a direct route for tumor spread into the skull base and adjacent cranial nerves. 5 In several reported experiences with nasopharyngeal cancer,6,7 erosion of the skull base by the primary neoplasm was often accompanied by involvement of the Vth, VIth, and XIIth cranial nerves (a clinical finding that was not observed in our patient).
Nasopharyngeal malignancies do not lend themselves to simple surgical management because of their location. 8 Moreover, in 29 to 64% of cases, CT or magnetic resonance imaging detects retropharyngeal lymphadenopathy.9,10 Huang studied a series of 1,605 nasopharyngeal cancer patients and recorded a frequency of skull base invasion of 36%. 11 Reports of skull base erosion secondary to nasopharyngeal cancer range from 12 to 36%.1,2,6,7,11
With regard to bone destruction mediated by osteoclasts, it is known that malignant cells secrete factors—such as transforming growth factors alpha and beta, epidermal growth factor, tumor necrosis factor, and interleukin 1—that stimulate osteoclastic activity. 12 These cells also promote the release of procathepsin D from tumor-associated immune cells; procathepsin D is an enzyme whose active form is linked with proteolysis of collagen chains in the extracellular bony matrix. 12 In addition to these paracrine factors, the parathyroid hormone activates osteoclast-related bone resorption. On the other hand, osteoblasts appear to regulate bone resorption by controlling the production of collagenase (the bone matrix-degrading enzyme). Osteoclasts may exert only an indirect action on bone because they lack the required surface receptors for the previously mentioned factors associated with the breakdown of bone matrix.
Chemoradiation for locally advanced nasopharyngeal cancer is the treatment of choice for suitable patients. It is associated with higher rates of survival compared with radiotherapy alone; according to Al-Sarraf et al, 3-year survival rates were 76 and 46%, respectively. 3 Our finding that combination therapy led to a complete primary tumor and nodal disease response in addition to bony regeneration at the site of skull base osseous destruction is consistent with findings reported by others after combined therapy or radiotherapy alone.11,13–15
Little is known about the other effects of combined therapy in cases of nasopharyngeal cancer with skull base erosion or skull base invasion. Roh et al evaluated survival and local control rates in 119 patients who were managed with a combination of cisplatin/5-fluorouracil and external-beam irradiation for nasopharyngeal cancer invading the base of the skull (bimodal therapy akin to that used in our patient). 16 In their experience, the 5-year disease-specific survival and local control rates in 11 patients with skull base erosion were not significantly different from those of 34 individuals without destruction of the skull base.
Clearly, our patient will require continued follow-up to ascertain the long-term results of treatment. Quantification of serum EBV DNA levels (which, unfortunately, was not practiced at our institution) might have allowed us to establish a more certain prognosis. In a reported series of nasopharyngeal cancer patients, Lo et al found that the relative risk of death from the disease was 1.6 for each 10-fold increase in serum EBV DNA concentration. 17
Because of the impressive response to therapy observed in our patient, and in view of the report by Roh et al 16 documenting that cure may be anticipated even in patients with advanced nasopharyngeal cancer, we believe that nasopharyngeal cancer patients with skull base erosion should be treated as aggressively as possible with chemoradiation. However, prior to the initiation of aggressive therapy, one must take into account the patient's general functional status, expected survival time relative to age, and the presence or absence of comorbidities.