
Abstract
Cerebrospinal fluid (CSF) rhinorrhea after a septoplasty procedure is very rare and potentially life-threatening. We present a case of iatrogenic postseptoplasty CSF rhinorrhea. To the best of our knowledge, only 2 other cases of CSF rhinorrhea complicating septoplasty have previously been reported. However, neither resolved in the manner that our case did, when spontaneous cessation of CSF rhinorrhea unexpectedly occurred upon removal of intranasal splints. We discuss the clinical importance of anatomic variations and potential causative mechanisms of CSF rhinorrhea during septoplasty. Our experience with this case suggests a mechanism of injury to the cribiform plate during septoplasty that has not been described previously.
Introduction
Septoplasty is one of the most widely performed operations in the treatment of nasal obstruction caused by septal deviation. Complications include hemorrhage, septal perforation, saddle nose deformity and, more rarely, cavernous sinus thrombosis and periorbital emphysema. 1 Although cerebrospinal fluid (CSF) rhinorrhea is well documented as a complication of nasal surgery, it has mostly been reported after rhinoplasty and endoscopic sinus surgery. CSF rhinorrhea after septoplasty is quite rare; to the best of our knowledge, only 2 cases have been previously reported in the literature. 1 CSF rhinorrhea has the potential for life-threatening sequelae, including meningitis, encephalitis, and cerebral abscess formation. We present a third case of iatrogenic CSF rhinorrhea after septoplasty. In our patient, the rhinorrhea resolved in a manner not previously described in the literature.
Case report
A 55-year-old man presented with a history of right nasal obstruction. On examination, we found that his septum was grossly deviated to the right. He underwent a septoplasty as a day case under general anesthesia. Using a standard hemitransfixion incision, mucoperichondrial flaps were elevated on either side of the septum. The deviated cartilage was centralized, and inferior bony spurs were removed using a pair of Tilley Henckel forceps.
Satisfactory realignment of the nasal septum was achieved. Bilateral Silastic intranasal splints were inserted, followed by packing with vaseline ribbon gauze. Four hours postoperatively, the packs were removed and the patient was discharged home uneventfully with instructions to return in 7 days for splint removal.
Three days postoperatively, the patient returned to the hospital, clinically well but with persistent unilateral watery rhinorrhea that had started after he arrived home. The right-sided rhinorrhea was confirmed to be CSF rhinorrhea by beta-2 transferrin assay. High-resolution computed tomography (CT) of the anterior cranial fossa demonstrated air in the cranial cavity, indicating a fracture or breach of the cribiform plate (figure 1).
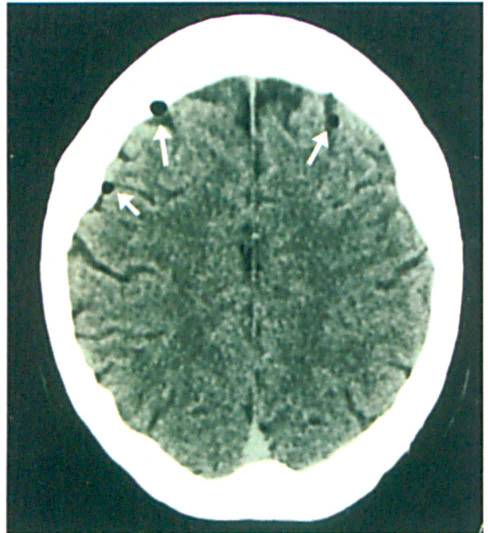
Pockets of air (arrows) are visible within the cranial cavity, over both frontal lobes
The patient was treated conservatively with intravenous antibiotics and strict bed rest with 45° elevation of the head of the bed. The following day, the patient's intranasal splints were removed on the ward, and the CSF rhinorrhea ceased completely. He was discharged home, and at the 6-month follow-up he remained well, with no recurrence of the rhinorrhea.
Discussion
In the 2 previously reported cases of iatrogenic CSF rhinorrhea after septoplasty, both patients required surgery via an endoscopic approach to repair the CSF leak with temporalis fascia. 1 In our case, spontaneous resolution was unexpectedly achieved with a simple maneuver, i.e., removal of the intranasal splints that had been inserted at the end of the septoplasty operation. Cartilage manipulation during septoplasty and subsequent insertion of the splints might have led to destabilization of the superior attachment of the middle turbinate to the cribiform plate in our patient.
The spontaneous resolution of CSF rhinorrhoea upon splint removal suggests that the Silastic splint had pushed the right middle turbinate into an overlateralized position, further weakening the superior attachment of the middle turbinate to the cribiform plate and causing a fine fracture defect (figure 2). Subsequent removal of the splint might have allowed the fracture margins to realign and seal off the CSF fistula, once the middle turbinate had returned to its natural position.
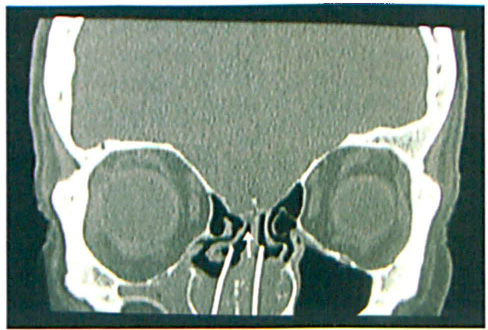
The CT scan shows the Silastic splint in situ and its relation to the middle turbinate, which appears lateralized by it. This might have destabilized the superior attachment of the middle turbinate to the cribiform plate.
Two other mechanisms of injury to the cribiform plate have previously been postulated in the development of iatrogenic CSF rhinorrhea after septoplasty. 2 First, when elevating septal mucoperichondrial flaps, advancing the elevator forceps superiorly too far beyond the limits of the ethmoid roof may lead to perforation of the cribiform plate. Second, grasping and fracturing the perpendicular lamina of the ethmoid bone to correct bony deviations may lead to the exertion of multidirectional rotational forces to the perpendicular lamina and delicate cribiform plate, thereby resulting in fractures of the latter. 1
The anatomy of the cribiform plate itself also makes it highly vulnerable to fracture. It is situated at the roof of the nasal cavity and is the most delicate part of the anterior cranial fossa. Here, the bony structures are very thin and the dura is tightly attached to bone. Multiple olfactory filaments perforate the cribiform plate, surrounded by a meningeal cuff containing CSF, which lies in direct communication with the subarachnoid space. 3 Shearing forces may cause fractures of the cribiform plate at its junction with the perpendicular plate of the ethmoid. 3 In addition, the ethmoid roof may be at different levels on the right and left sides (i.e., the distance between the highest level of the ethmoid labyrinth and cribiform plate ranges from 0.6 to 11.7 mm, and the distance from the floor of the nasal cavity to the cribiform plate ranges from 38 to 52 mm). 1 The perpendicular plate should therefore be gently manipulated during septoplasty, avoiding a rocking action that could fracture it. Turbinate or septum scissors should be used to remove the deviated portion of the perpendicular plate, carefully ensuring that the bone is cut, and not broken, before removal.
If a CSF leak is detected during septoplasty, it should be repaired intraoperatively; a variety of materials, such as temporalis fascia, septal mucosal grafts, or osteomucoperiosteal flaps can be used.3,4 However, conservative management should be attempted for a CSF leak diagnosed postoperatively.
Although cribiform plate fractures may not always be visible radiologically, the presence of a pneumocephalus indicates that the cranial cavity has been breached. The patient should be managed with strict bed rest in a semi-recumbent position, avoiding any physical strain. Lumbar drainage may be used if the leak persists. Although it has been theorized that prophylactic antibiotic use may reduce local inflammation and bacterial contamination of traumatized mucosa and exposed cartilage, evidence does not suggest that this reduces infection rates. 5 Fortunately, 70% of iatrogenic CSF fistulae close spontaneously. 3 Therefore, surgical intervention should be reserved for (1) patients whose leaks persist despite CSF drainage, or (2) those whose rhinorrhea continues for longer than 2 weeks.2,3
In conclusion, prevention of CSF rhinorrhea complications in septoplasty and other types of nasal surgery is achieved through good technique. Taking note of anatomic variations and potential causative mechanisms of CSF fistulae is critical; our experience with this case suggests a possible third mechanism of injury to the delicate cribiform plate during septoplasty—i.e., during insertion of intranasal splints—and certainly serves to emphasize the importance of their cautious insertion under direct vision to avoid overdisplacement of the middle turbinate and subsequent injury to the cribiform plate.