
Abstract
We propose the use of a microelectromechanical system (MEMS) accelerometer as a middle ear microphone for future totally implantable cochlear prostheses. The MEMS accelerometer would be attached to the umbo to detect and convert the natural bone vibration that occurs in response to external sounds into an electrical signal that represents the acoustic information. The signal could be further processed to stimulate cochlear implant electrodes. To determine the feasibility of our proposal, we conducted a study to investigate whether the characteristics of umbo vibration along two orthogonal axes—one axis being perpendicular to the tympanic membrane and the other axis being parallel to the tympanic membrane plane but orthogonal to the long process of the malleus—differ significantly enough to compromise the sensing performance of the proposed accelerometer should a position misalignment occur during the implant procedure. We used laser Doppler vibrometry to measure the displacement of the umbo along the two orthogonal axes in 4 cadaveric temporal bones at multiple frequencies within the audible spectrum. We found that the peak-to-peak displacement frequency response along both axes was nearly flat from 250 Hz to 1 kHz, and it gradually rolled off with a slope of approximately −20 dB and −40 dB per decade above 1 kHz and 4 kHz, respectively. At each frequency, the displacement exhibited a linear function of the input sound level with a slope of 20 dB per decade. A comparison of measurements along the two axes indicated a similar frequency response, with an average amplitude difference of 20%. The characterization data suggest that the performance of a miniature ossicular vibration-sensing device attached on the umbo would not be degraded in the event of a position misalignment. The data also indicate that a MEMS accelerometer needs to achieve a resolution of i g /√ Hz to detect normal conversation.
Introduction
More than 30 million people in the United States experience sensorineural hearing loss. While contemporary acoustic hearing aids offer the potential for moderate rehabilitation for a large number of cases, inherent technology limitations and the perceived social stigma associated with these devices have left many patients deprived of basic hearing abilities. Partially implantable middle ear and cochlear prosthetic systems have gained acceptance. However, the use of external accessories such as microphones and electronics presents reliability, practicality, and social acceptability concerns. It is therefore highly desirable to develop totally implantable prosthetic systems.
Significant research efforts have been devoted to the development of fully implantable middle ear systems that use piezoelectric and electromagnetic effects to compensate for conductive hearing loss,1–3 but fully implantable prosthetic systems are not yet commercially available. State-of-the-art semi-implantable cochlear devices can restore sensorineural hearing loss by directly stimulating the auditory nerve inside the cochlea. However, these implants still rely on inconvenient and socially unappealing external components such as a microphone and speech processor. The speech processors in the current implants can potentially be made as a part of a fully implantable system. Realizing a high-performance implantable microphone, however, presents a significant challenge.
We propose using a microelectromechanical system (MEMS) accelerometer as an implantable middle ear microphone for future totally implantable cochlear prostheses. The MEMS accelerometer would be attached to the ossicular chain to detect and convert the natural bone vibration that occurs in response to external sounds into an electrical signal that represents the acoustic information. The electrical signal would then be further processed by an implantable speech processor to stimulate cochlear implant electrodes. The accelerometer-based middle ear microphone design is attractive because of its potential for stable performance over the long term; the sensor would be fully encapsulated in a hermetically sealed, biocompatible package that does not require any opening to the environment, as does a conventional microphone. Thus, the sensor performance would not be degraded by subsequent scar tissue growth or infection as long as the device maintains adequate contact with the ossicular chain. Middle ear disease might have an effect on the accelerometer performance in that the filling of the middle ear by fluid and associated mass loading could alter the natural mechanics of the ossicles.
The most effective sensing performance can be obtained when the accelerometer is attached at an ossicular location that exhibits the greatest vibration amplitude in response to an external acoustic stimulus. Published data indicate that the greatest amplitude of vibration along the ossicular chain takes place at the umbo.4–8 Because the surface of the umbo is curved, it is likely that during an implant procedure, the sensor would exhibit a position misalignment anterior or posterior to the long process of the malleus, thus deviating from a desired sensing axis and degrading system performance. Therefore, it is necessary to investigate and characterize the umbo vibration characteristics of human temporal bones along different axes.
Decraemer and Khanna have performed an extensive series of measurements along the malleus of cats.9,10 These measurements derived the vibration amplitude along orthogonal axes at different points on the malleus by data-fitting techniques. 11 However, to the best of our knowledge, no characterization that directly measures the vibration amplitude along different axes of the umbo in human temporal bones has been reported until now.
The motion of the umbo in response to an input audio stimulus can be described by amplitude vibration along three orthogonal axes (figure 1). For the purposes of this article, the primary axis of the umbo (the y-axis) is defined as the direction perpendicular to the tympanic membrane. This axis represents the direction in which the pinna focuses the sound pressure wave, and this is where the largest vibration amplitude is expected. The secondary axis is the vector parallel to the tympanic membrane plane but orthogonal to the long process of the malleus, which is perpendicular to the viewing plane along the z-axis.
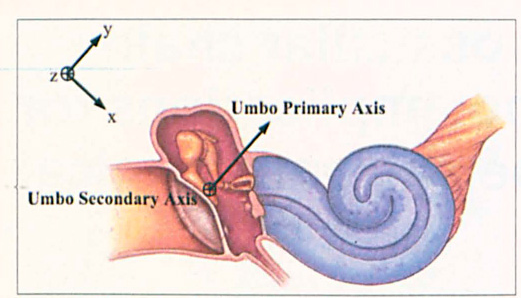
Illustration Depicts the Axes Characterized by the Laser Doppler Vibrometer.
In principle, any two axes that are perpendicular to each other and perpendicular to the primary axis can be chosen as the secondary axis. In practice, however, to ensure the repeatability of measuring response from multiple bones, it is desirable to conduct the measurement along the direction parallel to the tympanic membrane but orthogonal to the long process of the malleus; this axis is designated the z-axis. It is preferable to perform an additional measurement along the x-axis, which is parallel to the tympanic membrane plane and parallel to the long process of the malleus. However, it is not possible to prepare bone samples for these measurements without damaging the tympanic membrane. The measurement data obtained from the primary and secondary axes can provide a better understanding of the sensor performance and its sensitivity associated with position misalignment during implantation. The measurement data can also serve as a design guideline for the MEMS accelerometer development.
Materials and Methods
Four cadaveric temporal bones obtained through the Anatomical Gifts Program at the Case Western Reserve University School of Medicine's Department of Anatomy were used in this study. To maintain soft-tissue compliance and hydration after thawing, the bones were kept stored in 1:10,000 merthiolate in 0.9% saline solution. Each temporal bone was visually inspected under a Zeiss operating microscope to verify an intact tympanic membrane, ear canal, and ossicular bone structure.
Temporal bones were opened in two stages. In the first stage, a bone was securely mounted in a temporal bone clamp. A simple mastoidectomy via a facial recess approach was performed. The mastoidectomy was performed by identifying the tegmen mastoideum superiorly, the external auditory canal anteriorly, and the sigmoid sinus posteriorly using an otologic drill. The facial recess was opened by identifying the short process of the incus and drilling posterior to this landmark and anterior to the facial nerve. Once the middle ear mucosa was identified, the facial recess was further opened carefully until the umbo and incudostapedial joint were visualized through the facial recess. Any bones showing overt pathology or evidence of injury as a result of the mastoidectomy and exposure of the middle ear cavity would not have been included in this study.
A piece of 1-mm 2 reflective film, weighing approximately 50 μg, was then placed on the posterior surface of the umbo for the secondary axis vibration measurement by using a laser Dopplervibrometer (LDV). An LDV generates a laser beam at a reference frequency. When the beam is reflected from a target moving or vibrating along the direction of the laser, a frequency shift that is proportional to the target velocity is produced. By comparing the frequency of the reflected beam to the reference frequency, the velocity and frequency of the vibration can be obtained. A VibroMet 500V laser Doppler vibrometer (MetroLaser; Irvine, Calif.) was employed for the temporal bone characterization.
After the measurement was performed, the second stage of drilling open the temporal bone was undertaken. In this stage, the facial recess was widened interiorly and posteriorly so that full access to the middle ear was achieved. In the middle ear, most of the cochlea was drilled down; the posterosuperior quadrant was not. In the posterosuperior quadrant, a thin piece of bone was left entirely surrounding the stapedial footplate so that the annular ligament was completely preserved. The facial nerve and sigmoid sinus were then removed. The drilling proceeded as far into the petrous apex as was necessary in order to visualize the umbo from the medial aspect of the tympanic membrane. (Ravicz et al showed that changing the stapes-cochlear input impedance by draining the cochlea or removing tissue can result in a corresponding change in the motion of the ossicles near the stapes. 12 However, the effect on input impedance and motion at the tympanic membrane was negligible.) The bone was then thoroughly rinsed in saline.
A piece of reflective film was again placed on the posterior surface of the umbo as a target for repeating the vibration characterization along the secondary axis of the umbo. (The results of the two measurements made along the secondary axis can be used as a comparison to study the effect on the umbo's vibration characteristics before and after the medial wall dissection, as we discuss in the following section.) At this point, another piece of reflective film was placed on the umbo to characterize its vibration behavior along the primary axis.
Each temporal bone was placed in a weighted temporal bone holder. Pure tones from a function generator with amplitudes from 70 to 100 dB sound pressure level (SPL) in the audible spectrum were presented to the tympanic membrane by an insert earphone. A probe microphone was positioned approximately 4 mm from the tympanic membrane to monitor the input SPL. Umbo vibration characterization along the two defined axes was conducted by using the LDV as described earlier.
Results
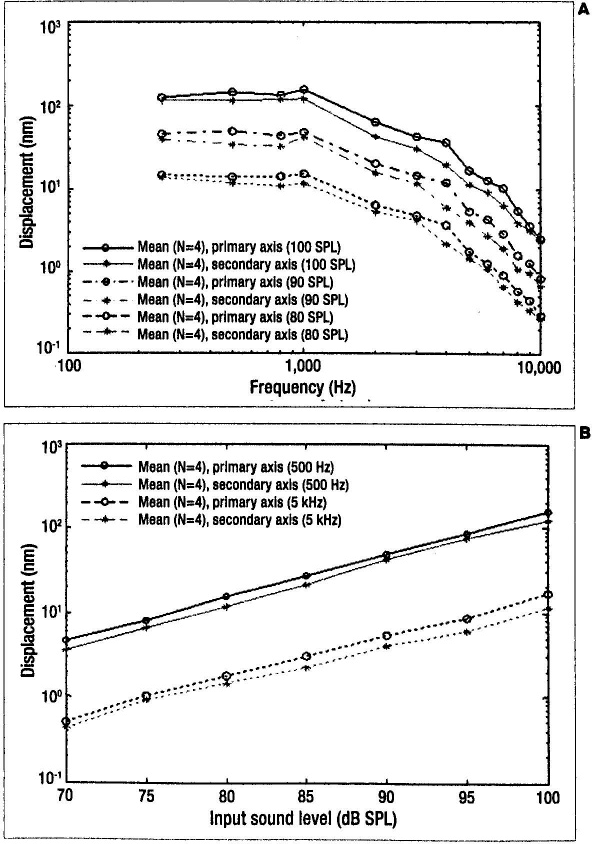
The average peak-to-peak displacement of the umbo measured along the primary and secondary axes in the 4 cadaveric temporal bones, stimulated by an input tone at 80, 90, and 100 dB SPL within the audible spectrum, is shown in figure 2, A. The shape of the displacement frequency response along the primary axis was almost identical to that along the secondary axis. The response curves were nearly flat up to 1 kHz, with an umbo vibration peak-to-peak amplitude of about 100 nm at 100 SPL, and they exhibited a roll off with a slope of-20 and −40 dB per decade above 1 kHz and 4 kHz, respectively. A 20% increase in displacement amplitude was measured along the umbo primary axis compared with the secondary axis. Although the difference between the two axes measurements was small, it occurred with approximately equal magnitude in all bones at all sound levels. Therefore, potential position misalignment of the accelerometer during an implant attachment process would not cause a significant sensing performance degradation. An accelerometer detects umbo-vibration-induced acceleration and converts the signal into an electrical output such as voltage for further signal processing. A 20% difference in umbo displacement amplitude would result in a 1.5-dB difference in the minimum detectable sound strength, which is small with respect to a typical full-scale signal range between 40 and 65 dB across the audio frequency band. The average loudness response of the umbo along the primary and secondary axes at the frequencies of 500 Hz and 5 kHz is shown in figure 2, B. At each frequency, the displacement exhibited a linear function of the input SPL with a slope of 20 dB per decade.
Graphs show the displacement response curves of the umbo along the primary
and secondary axes after medial wall removal.
It is necessary to derive the umbo acceleration response characteristics along the primary axis from the measured vibration behavior as a design guideline for developing the MEMS-accelerometer-based middle ear microphone. The resulting acceleration frequency response of the umbo along the primary axis is shown in figure 3, A. The acceleration amplitude increased with a slope of 40 dB per decade from 250 Hz to 1 kHz and with a slope of about 20 dB per decade from 1 kHz to 4 kHz. Above 4 kHz, the acceleration signal remained relatively constant. The linear relationship of 20 dB per decade between the acceleration amplitude and input sound level is shown in figure 3, B. As depicted in this figure, this allowed for an acceleration signal projection for an input sound level below 70 dB SPL, which is the resolution limit of the LDV measurement system.
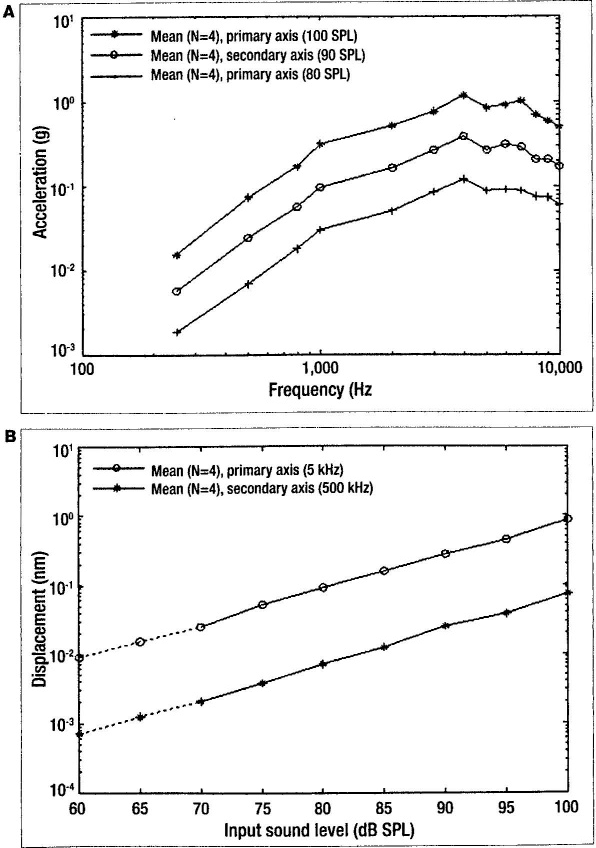
Graphs show the acceleration response curves of the umbo along the primary
axis after medial wall removal.
The umbo vibration characteristics along the secondary axis before and after the medial wall dissection are presented in figure 4. As seen in figure 4, A, the corresponding average peak-to-peak displacement of the umbo from the 4 cadaveric temporal bones stimulated by an input tone of 80, 90, and 100 dB SPL within the audible spectrum exhibited the same characteristics as illustrated in figure 2, A. The corresponding average peak-to-peak displacement of the umbo as a function of input sound level at 1 kHz and 5 kHz exhibited a linear relationship of 20 dB per decade at each frequency, as shown in figure 4, B. From this measurement, an insignificant difference was found in the response curves before and after medial wall dissection, thus verifying that the umbo vibration characteristics measured along the primary axis are valid and can be used as a design guideline for implementing the proposed implantable accelerometer.
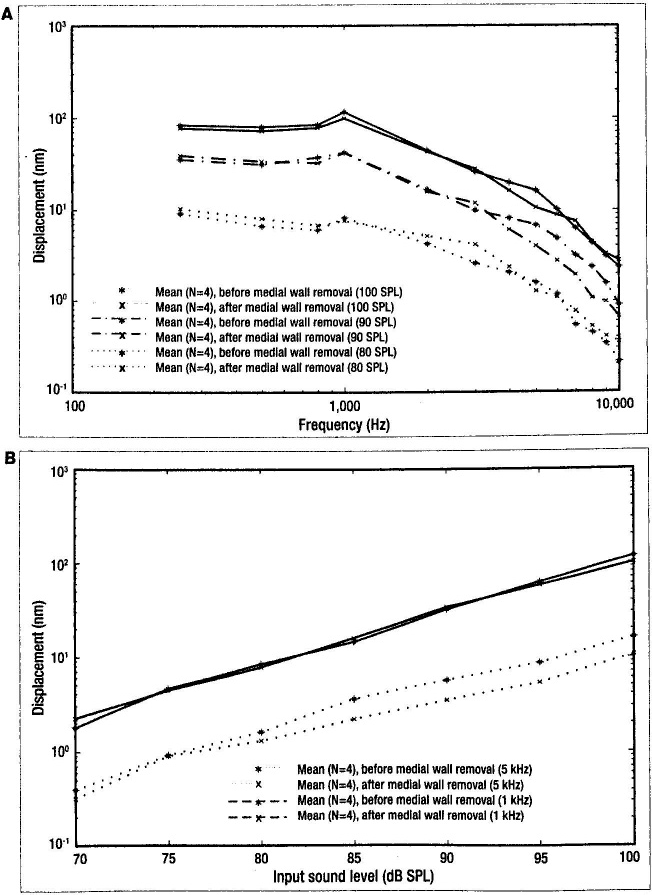
Graphs show the displacement response curves of the umbo along the secondary
axis before and after medial wall removal.
Discussion
Keeping in mind that speech energy is focused primarily between 500 Hz and 8 kHz and that the loudness of normal conversation is approximately 60 dB SPL, figure 3, B shows that within the audible spectrum, 500 Hz has the lowest acceleration response, and thus it is most difficult to detect. The projected acceleration amplitude for a 60-dB SPL input sound at 500 Hz is approximately 700 μg, which can serve as a reasonable target for detecting normal conversation, where g refers to the earths gravitational acceleration and can be expressed as 9.8 m/s 2 . Modern cochlear implants employ multiple channels and electrodes to provide an appropriate stimulus to the correct location within the cochlea. At 500 Hz, the electrode channel bandwidth is around 200 Hz. Therefore, to detect sounds at 60 dB SPL at 500 Hz, an accelerometer achieving a sensing resolution of 35 ì g/√Hz is required. The findings expressed in figure 3, A show that the maximum umbo acceleration was approximately 1 g along the primary axis.
In conclusion, a comparison of umbo measurements along both axes in our study indicated a similar vibration frequency response, with approximately a 20% difference in signal strength. These data suggest that the performance of a miniature ossicular vibration-sensing microsystem attached to the umbo would not be degraded by a position misalignment of the sensor. Furthermore, an accelerometer with a resolution of 35 ì g/√Hz would be required to detect an input sound level of 60 dB SPL at 500 Hz as a reasonable target for normal conversation.