
Abstract

A 3-month-old boy was referred to us from the Bahamas for evaluation of persistent aspiration. The patient had been experiencing persistent gagging and cough during feeding. Upper gastrointestinal studies in the Bahamas had been inconclusive.
Upon examination at our institution, the patient was found to be without stridor or respiratory distress, but he experienced a visible cough during a trial of oral feeding, and a gastric feeding tube was placed. Flexible laryngoscopy showed a deep space in the interarytenoid area suggestive of a laryngeal cleft. Direct laryngoscopy and bronchoscopy were performed with careful attention to the interarytenoid area, and they confirmed the presence of a laryngeal cleft that extended into the cricoid cartilage (figure 1). The airway was otherwise normal. A properative modified barium swallow cofirmed aspiration with feeding consistencies.
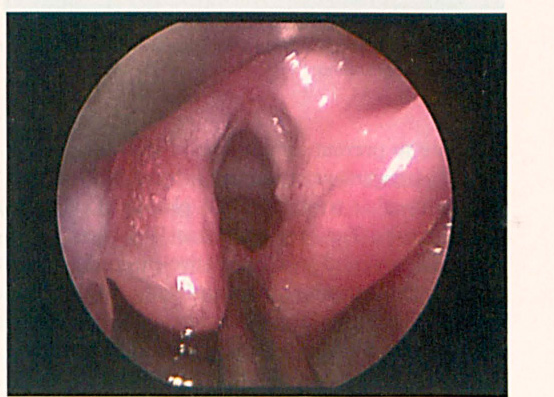
Preoperative Laryngoscopy shows the Laryngeal Cleft Extending into the Cricoid Cartilage.
Endoscopic repair was performed by denuding the mucosa with a CO2 laser and then suturing the mucosal cleft together (figure 2). The patient was extubated on the table, and he was fed via a gastric feeding tube for 1 month. At follow-up, a modified barium swallow test detected no evidence of aspiration, and the patient tolerated oral feeding without coughing. The gastric feeding tube was removed, and the child resumed oral feeds.

Congenital laryngeal anomalies occur in approximately 1 of every 2,000 live births; laryngeal clefts represent 0.5 to 1.6% of these abnormalities. 1 A high index of suspicion is required to make an early diagnosis and prevent chronic pulmonary aspiration.
Benjamin and Inglis 2 developed a classification system for laryngeal clefts based on their location:
A type 1 (supraglottic interarytenoid) cleft is located above the level of the vocal folds.
A type 2 cleft extends below the vocal folds and into the upper cricoid cartilage.
A type 3 cleft extends through the cricoid cartilage and possibly into the cervical trachea.
A type 4 cleft extends into the thoracic trachea and extends variably toward the tracheal carina.
The spectrum of clinical symptoms includes a hoarse cry, stridor, dysphagia, cough, dyspnea, and cyanosis during feeding in type 1 patients; aspiration and recurrent pneumonia in type 2 and 3 patients; and early respiratory distress in type 4 patients. Microlaryngoscopy and bronchoscopy are the definitive means of diagnosing laryngeal clefts. Careful attention should be paid to the interarytenoid space to avoid a missed diagnosis of a subtle type 1 cleft. Once a laryngeal cleft has been diagnosed, a systematic evaluation is required to identify associated anomalies.
Early medical management is required to prevent complications. The primary goals of medical management are to prevent aspiration and gastroesophageal reflux. Management strategies include thickening of feeds, antireflux treatment, and placement of a nasogastric tube. The symptoms associated with type 1 clefts may respond to conservative measures, but if they fail, the definitive treatment is surgical repair via either a minimally invasive endoscopic approach or open surgery. Open surgery is required for type 3 and 4 clefts; these procedures include a lateral approach with lateral pharyngotomy, a lateral approach with posterior pharyngotomy, and an anterior translaryngotracheal approach, which is the most commonly used open approach.
Obviously, the endoscopic approaches for the repair of type 1 and 2 clefts have many advantages over the open approaches, including avoidance of a skin incision, laryngofissure, and pharyngotomy. Also, revision surgery can be accomplished easily without additional morbidity. The closure is performed with the aid of an operating microscope, suspension laryngoscopy, and an endoscopic needle driver and knot pusher. 3 Many surgeons prefer to denude the mucosal margin of the cleft with a CO2 laser in superpulse mode. 3 Once the endolaryngeal and cricopharyngeal mucosa are divided, mucosal flaps are created on either side of the incision with microscissors, and a double-layer closure is made with the sutures placed in a distal to proximal fashion.
Endoscopic cleft repair can be performed with spontaneous ventilation anesthesia. In cases where intubation anesthesia is administered, the patient can often be extubated immediately after surgery and fed after 5 to 14 days. The results of endoscopic laryngeal cleft repair are satisfactory, as reported success rates range from 80 to 100%.4,5