
Abstract
COVID symptoms typically can last up to four weeks (Chippa et al., 2023). However, for many individuals, the symptoms can persist for weeks or months. Researchers of a systematic review concluded that at least 45% of COVID survivors experience ongoing symptoms for more than four weeks (National Research Action Plan, 2022). The symptoms and conditions that persist or develop four weeks after the initial COVID or SARS-CoV-2 infection are referred to as “long COVID,” “long-haul COVID,” “ongoing COVID,” or “chronic COVID syndrome” (long COVID hereafter) (Chippa et al., 2023; National Research Action Plan, 2022). In the United States, 40% of adults have had COVID, and 19% of those who had COVID had long COVID, resulting in a prevalence of 7.5% in the U.S. adult population (National Center for Health Statistics, 2022).
While initially causing respiratory problems, the virus can affect almost every organ in the body and lead to multi-organ syndrome (Ziauddeen et al., 2022). For example, SARS-CoV-2 virus is found in the eye's tear film (Gulias-Cañizo et al., 2021) and can lead to conjunctivitis and impact the ocular system (Akbari & Dourandeesh, 2022; Ho et al., 2020). A systematic review of case reports and cross-sectional case series suggests that ocular inflammation may occur within one to six weeks after COVID infection (Sen et al., 2022). Researchers in another systematic review and meta-analysis of 19 cross-sectional studies involving 7,300 individuals estimated that 11.0% of COVID patients had ocular manifestations of the disease (Nasiri et al., 2021).
Retinal involvement and anomalies due to COVID have been reported (Menuchin-Lasowski et al., 2022). COVID can lead to retinopathy, which can impair vision (Mesentier-Louro et al., 2021). Generalized hypoxia resulting from pulmonary fibrosis in COVID patients may cause visual disturbances (Baig, 2022). Although some of the symptoms occur during the acute phase of COVID, it is not yet clear whether these ocular manifestations can also develop later and are related to long COVID. Long COVID patients can experience ocular symptoms, such as eye pain, blurred vision, dry eye, and photophobia (Trott et al., 2022). Furthermore, several post-COVID conditions such as headaches, dizziness, fatigue, and myalgia have been linked to visual disturbances and vision loss (Trott et al., 2022). Researchers are conducting studies on the long-term effect of COVID on the eyes (Pagen et al., 2022). There have been a few studies on COVID and vision difficulties (Carcamo Garcia et al., 2021; Finsterer et al., 2021; Ripa et al., 2022). However, the association of long COVID on vision difficulties have not been examined nationally in the United States. Therefore, this study examined the association of long COVID with vision difficulties using a nationally representative database from the Household Pulse Survey (U.S. Census Bureau, 2022a, 2022b).
Methods
Study Design and Data Source
The present study is an observational study with cross-sectional analysis of the data from the Household Pulse Survey (HPS). We used HPS data collected from adults (aged 18 years or older), which was gathered between September 14, 2022, and November 14, 2022. The HPS began in April 2020 in response to the COVID pandemic and is conducted by the U.S. Census Bureau in partnership with 16 other federal agencies (U.S. Census Bureau, 2022b). The HPS is designed to produce national-level, state-level, and metro-level estimates for adults living in households during the coronavirus pandemic and recovery. The survey uses a systematic sample of all eligible household units, randomly selected from the Census Bureau Master Address File, and supplemented by the Census Bureau Contact Frame (U.S. Census Bureau, 2022a). The survey is administered online across all 50 states and the District of Columbia (US Census Bureau, 2022b) and gathers information on a range of topics, including socio-demographic characteristics, employment status, food insecurity, healthcare accessibility, physical and mental health, and COVID-related information, including vaccine, testing, and symptoms (US Census Bureau, 2022b). Beginning June 1, 2022, the survey included questions on the presence of COVID symptoms that lasted for three months or longer (US Census Bureau, 2022b). For this study, we used data from the publicly available HPS, which do not contain any identifiable information about individuals. As a result, no ethical concerns arise from the collection, analysis, and reporting of the data.
The analytical sample included adults who responded to questions about long COVID symptoms. We also excluded adults who were in the acute COVID phase (up to four weeks after COVID initial symptoms) (N = 1,311) because of the possibility that at least four weeks after infection is needed to identify long COVID related vision difficulties (CDC, 2022). The final sample comprised 51,288 adult respondents.
Measures
Dependent Variable: Vision Difficulties
The dependent variable for the study was vision difficulties defined as: no difficulty, some difficulty, a lot of difficulty, and unable to see. The variable was derived from the HPS Washington Group Short Set of Functioning (WG-SS) section of the questionnaire. Participants were asked “Do you have difficulty seeing, even when wearing glasses?” and were provided the following choices: no—no difficulty, yes—some difficulty, yes—a lot of difficulty, and cannot do at all. Since 2001, this instrument has been extensively tested and validated across countries. We combined “a lot of difficulty,” or “unable to do” under the category “at least a lot of difficulty” due to small sample sizes for each. This three-way categorization of functional difficulties from the Washington Group Short Set of Questions has been widely used in the literature (Hanass-Hancock et al., 2023).
Key Explanatory Variable: COVID Status
We categorized the key explanatory variable, COVID categories, into three groups: (1) long COVID, (2) short-term COVID, and (3) no COVID. The “short-term COVID” group included individuals who had contracted COVID but did not experience symptoms for 4 weeks or more, while the “no COVID” group comprised adults who had never been infected with COVID. More precisely, the presence of long COVID was identified from the following question: “Did you experience any symptoms lasting 3 months or longer that you did not have prior to contracting coronavirus or COVID?” Persons who had other COVID (not long) or no COVID were identified based on their response “no” to the above question as well as their response to the question on COVID positivity: “Have you ever received a positive test result for COVID (using a rapid point-of-care test, self-test, or laboratory test), or been informed by a doctor or other healthcare provider that you have or had COVID-19?”
Other Explanatory Variables
We incorporated demographic variables: age (18–34 years, 35–44 years,45–54 years, 55–64 years, and 65 years or older); gender (female, male, transgender); race and ethnicity. We also examined social determinants of health: marital status (married, widowed, separated or divorced, and never married); poverty status, according to the federal poverty line (poor, < 100%; low income, 100% to < 200%; middle income, 200% to < 400%; and high income, ≥ 400%); education (less than high school, high school, associate degree, college); food insecurity (food secure or not food secure); health insurance (private, public, and none); and geographical region (Northeast, Midwest, South, and West). We adjusted for remote work for at least 1 day in past 7 days of survey (yes or no) because the increased use of digital devices during the pandemic, such as computers and smartphones, has been linked to increased visual fatigue, causing eye strain, headaches, and blurred vision (Bhattacharya et al., 2020). We also adjusted for COVID vaccine (no vaccine, one dose with or without booster, fully vaccinated with no booster, and fully vaccinated as well as boosted), since some research found its association with vision problems (Nyankerh et al., 2022). Since poor mental health may be associated with vision difficulties, we adjusted for depression (categorized as Patient Health Questionnaire, PHQ-2, score > 3), and anxiety (measured using the Generalized Anxiety Disorder, GAD-2, score > 3) (Demmin & Silverstein, 2020).
Statistical Analysis
To account for the complex survey design and to ensure that our estimates were representative of the population, we used replicate survey weights provided by the HPS. We also employed a jackknife approximation to adjust for variability in the estimation of these weights. To test the association between categorical explanatory variables and vision difficulty, the Rao-Scott chi-square tests were employed. To evaluate the association of long COVID with vision difficulty, we conducted multivariable multinomial logistic regressions. In these regressions we adjusted for age, gender, race or ethnicity, marital status, poverty status, education, health insurance, region, remote work, anxiety, and depression. We created missing indicators for explanatory variables which had missing response and included the missing indicators in the regressions. All the tests were two sided and considered significant at 5% level of significance. All analyses were conducted using the SAS survey procedures considering the replicate weights with jackknife method of variance estimation (Lohr, 2010).
Results
In our study, participants were 49.9% female, 47.4% male, and 2.7% transgender; non-Hispanic white (64.1%), non-Hispanic Black (10.2%), Hispanic or Latino (16.1%); 55.8% were currently married, 33% had college degrees, and 26.8% were aged 65 years or older. Only 16.7% had never been vaccinated (see Supplemental Table 1 and Table 1).
Characteristics of Census Household Pulse Survey Respondents (November 2–14, 2022) by COVID Status.
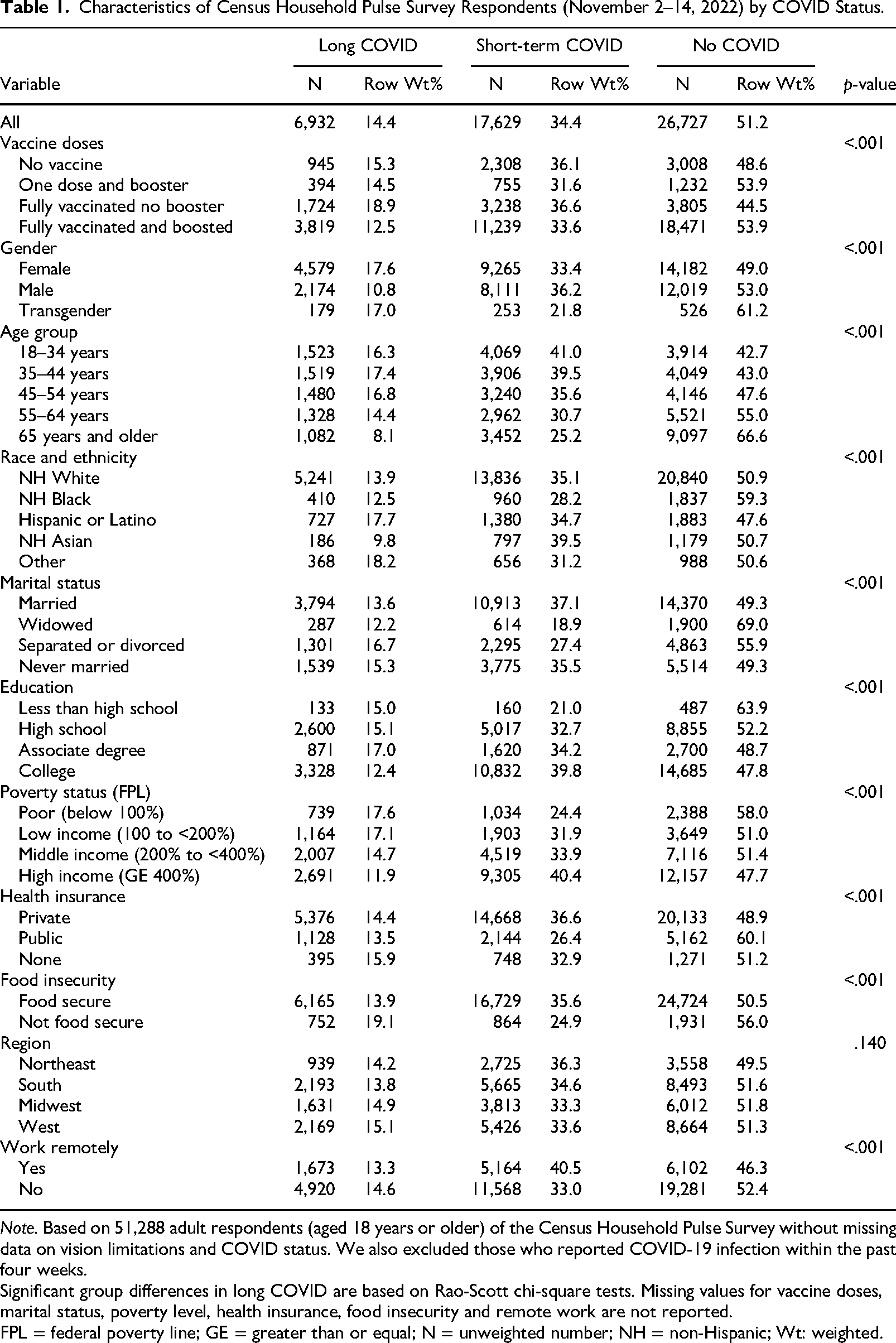
Note. Based on 51,288 adult respondents (aged 18 years or older) of the Census Household Pulse Survey without missing data on vision limitations and COVID status. We also excluded those who reported COVID-19 infection within the past four weeks.
Significant group differences in long COVID are based on Rao-Scott chi-square tests. Missing values for vaccine doses, marital status, poverty level, health insurance, food insecurity and remote work are not reported.
FPL = federal poverty line; GE = greater than or equal; N = unweighted number; NH = non-Hispanic; Wt: weighted.
Characteristics of Adults by Long COVID
Long COVID was reported by 14.4% of adults, and 51.2% adults reported no COVID Infection (see Supplemental Table 1). We observed statistically significant differences in COVID status by all the variables (see Table 1). For example, a higher percentage of females than males (17.6% vs. 10.8%) reported long COVID in comparison to no COVID, and we observed that the percentage of transgender with long COVD was similar to women (17.0% vs 17.6%) (see Table 1). For those who reported long COVID: A higher percentage of adults (17.6%) were lower income (< 100% of the federal poverty line) compared to 11.9% with high income (≥ 400% of the federal poverty line). A higher percentage of the long COVID sample had no health insurance (15.9%), compared to 13.5% who had public health insurance, and 14.4% who had private health insurance. In terms of food insecurity, 19.1% were food insecure, compared to 13.9% who had food security. Fully vaccinated and boosted responders had a lower prevalence of long COVID (12.5%) in comparison to individuals who were not vaccinated (15.3%).
Characteristics of Adults by Vision Difficulty
Nearly one-third (33.1%) of adults reported having some vision difficulty, with 4.2% having at least a lot of difficulty (“a lot of difficulty” and “cannot do at all”). Compared to adults with no COVID, adults with long COVID had a higher percentage reporting at least a lot of difficulty seeing (6.0% vs. 4.5%) and some difficulty seeing (41.6% vs 33.5%) (see Table 2).
Characteristics of Census Household Pulse Survey Respondents (November 2–14, 2022) by Vision Difficulty (Weighted Row Percent).
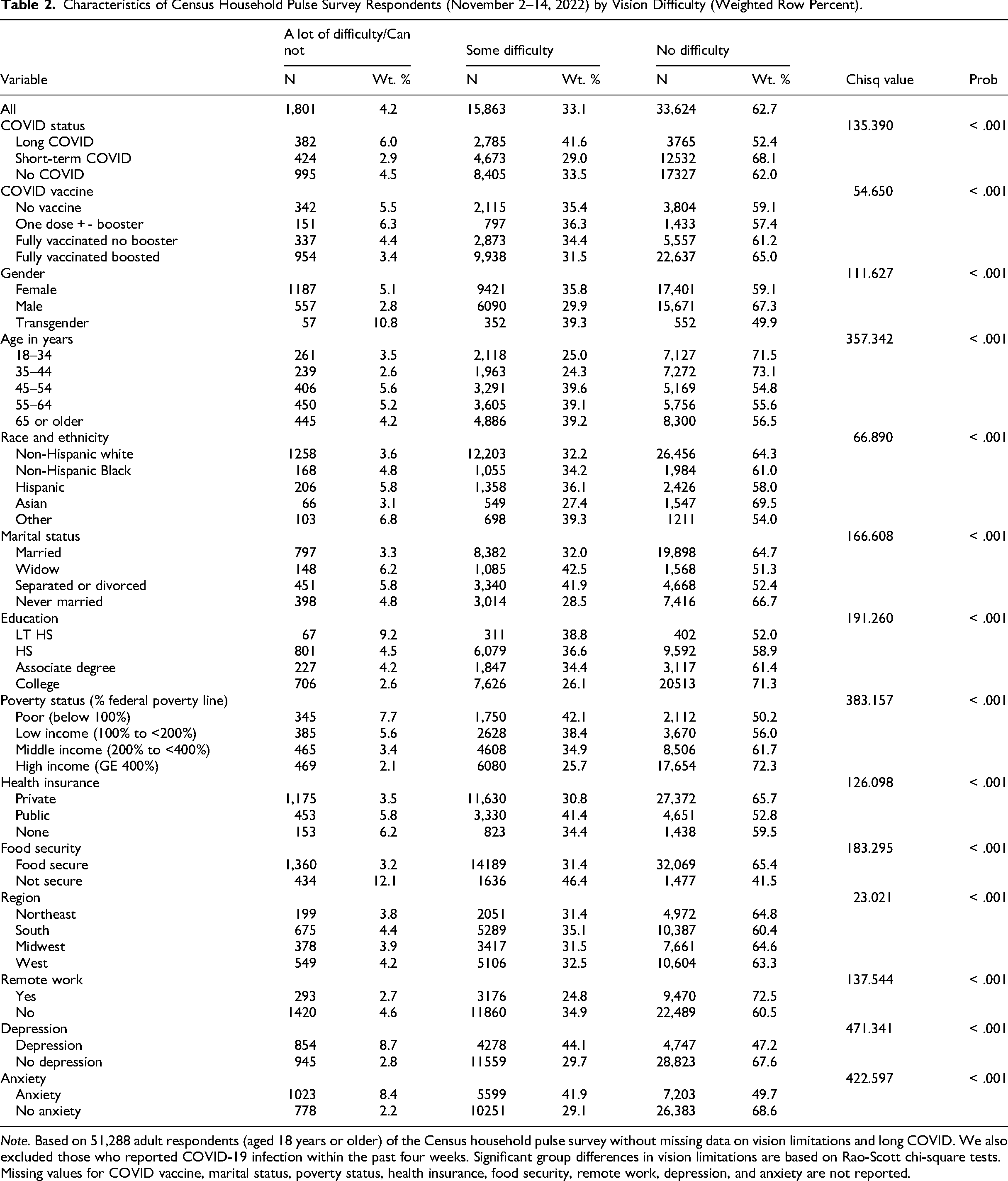
Note. Based on 51,288 adult respondents (aged 18 years or older) of the Census household pulse survey without missing data on vision limitations and long COVID. We also excluded those who reported COVID-19 infection within the past four weeks. Significant group differences in vision limitations are based on Rao-Scott chi-square tests. Missing values for COVID vaccine, marital status, poverty status, health insurance, food security, remote work, depression, and anxiety are not reported.
Across gender groups, the prevalence of “at least a lot of difficulty seeing” and “some difficulty seeing” were the highest among transgender (10.8% and 39.3%, respectively) compared to males (2.8% and 29.9%) and females (5.1% and 35.8%). Vision difficulties were more prevalent among the 45–54 years or older age group compared to the 18–34 years age group (45.25% vs. 28.5%). In terms of marital status, widowed individuals had the highest prevalence of significant vision difficulties (6.2%) and some difficulty (42.5%), which is notably higher compared to other marital status groups. Married individuals had the lowest prevalence of significant vision difficulties (3.3%) and the highest percentage of respondents with no vision difficulty (64.7%). Never married individuals also had a relatively low prevalence of significant vision difficulties (4.8%) and the highest percentage of respondents with no vision difficulty (66.7%). Separated or divorced individuals fell in-between, with a 5.8% prevalence of significant vision difficulties and 41.9% experiencing some difficulty. A higher percentage of those with less than high school education reported vision difficulties compared to those with college degrees (48.0% vs. 28.7%). Similarly, 49.8% of individuals with an income below the poverty line had higher rates of vision difficulties compared 27.8% in the high-income group (49.8% vs 27.8% for vision difficulties of any degree). Food security and private health insurance were associated with lower prevalence of vision difficulties. Depression (52.8% vs 32.4%) and anxiety (50.3% vs 31.4%) were associated with higher prevalence of vision difficulties.
Adjusted Association of Long COVID With Vision Difficulty
In unadjusted multinomial logistic regression analysis, adults with long COVID had higher odds of reporting some difficulty (1.47; 1.28, 1.68) and at least a lot of difficulty (1.57; 1.27, 1.93) in comparison to adults with no COVID (see Table 3). In adjusted multinomial logistic regression analysis, adults with long COVID had higher odds of reporting some (AOR = 1.47, 95% CI = 1.27, 1.70) and at least a lot of difficulty seeing (AOR = 1.47, 95% CI = 1.19, 1.81) compared to those with no COVID, after adjusting for age, sex, marital status, education, income, race and ethnicity, health insurance, remote work, region, food insecurity, anxiety, depression, and COVID vaccine. We did not observe a statistically significant difference between adults who experienced short COVID and those with no COVID in terms of reporting some difficulty (AOR = 0.97, 95% CI = 0.88, 1.06) and at least a lot of difficulty seeing (AOR = 0.84, 95% CI = 0.68, 1.04).
Adjusted Odds Ratios (AOR) and 95% Confidence Intervals (CI) of Long COVID and No COVID From Multivariable Multinomial Logistic Regressions on Visual Difficulties (Reference Group = No Difficulty).
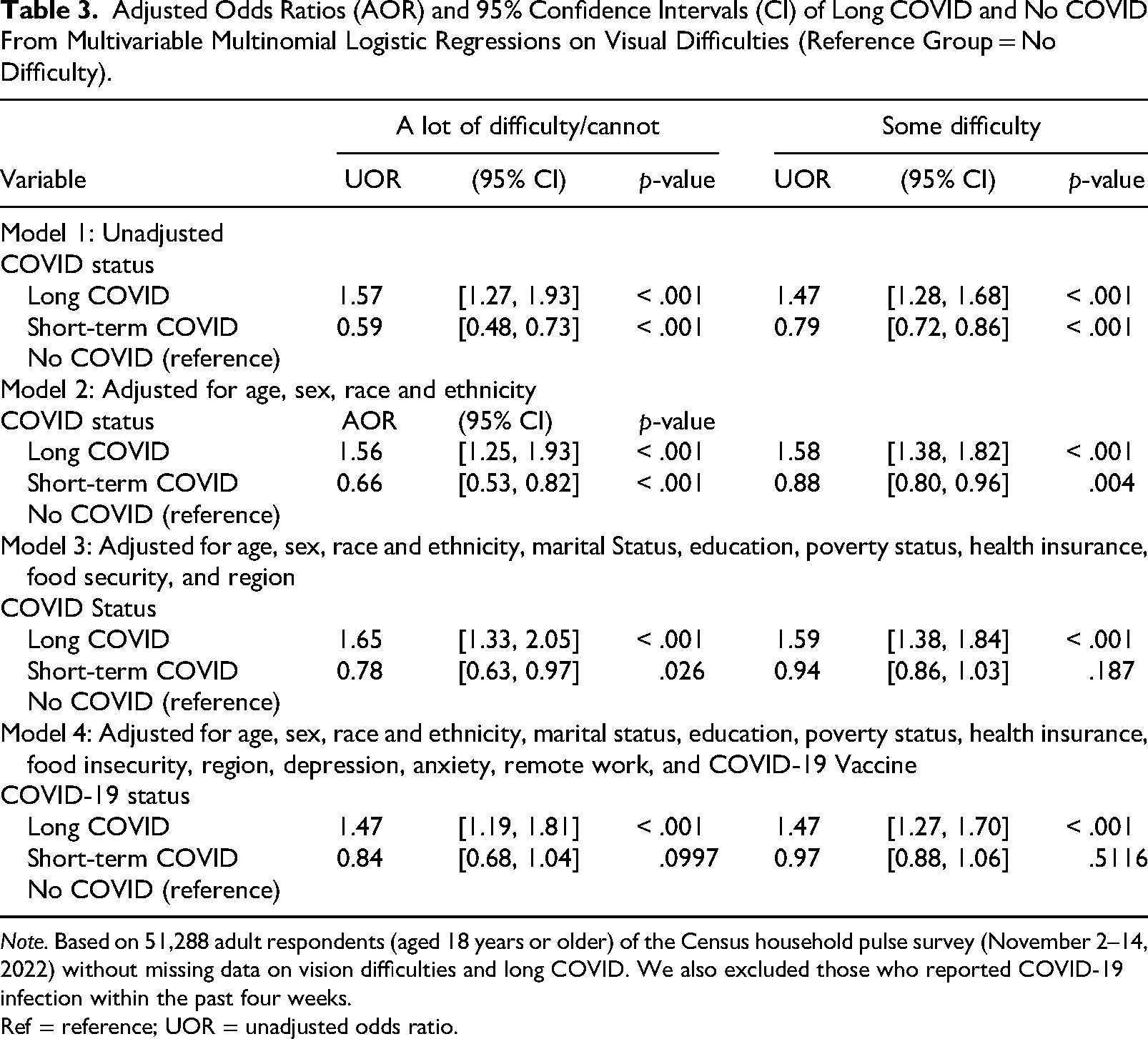
Note. Based on 51,288 adult respondents (aged 18 years or older) of the Census household pulse survey (November 2–14, 2022) without missing data on vision difficulties and long COVID. We also excluded those who reported COVID-19 infection within the past four weeks.
Ref = reference; UOR = unadjusted odds ratio.
Discussion
Overall, in this study of adults, 14.4% reported having had long COVID and 37.3% reported vision difficulty (33.1% with some difficulty and 4.2% with at least a lot of difficulty). The prevalence of vision difficulties was higher among individuals with long COVID than those with no COVID in both unadjusted and adjusted models. After adjusting for potential explanatory variables that may affect vision difficulties, those with long COVID had 1.47 times the odds of reporting vision difficulties as those with no COVID, whether vision difficulties are severe (at least a lot of difficulty) or moderate (some difficulty).
Previous researchers reported that the most common symptoms that occur after the initial acute COVID infection include dyspnea, myalgia, insomnia, mood disturbance, brain fog, headache, and anxiety (Naik et al., 2021; Seang et al., 2022; Tabacof et al., 2022). Common triggers of these exacerbations were reported as physical exertion, stress, and dehydration (Tabacof et al., 2022). Some researchers assessed the impact of acute COVID on eye problems but have not specifically addressed vision (Akbari & Dourandeesh, 2022; Bhattacharya et al., 2020; Ho et al., 2020; Sawalha et al., 2020; Sen et al., 2021). A few researchers assessed the impact of long COVID on ocular manifestations, although the studies were small. Researchers of two small case-control studies detected thinning of the retinal layers, especially the ganglion cell layer and the inner plexiform layer (31, 32). They also reported alterations in the contractile pupillary light responses after COVID infection (Bitirgen et al., 2022; Kanra et al., 2022). In a cohort study from China, researchers followed 155 COVID survivors. They reported that, even after two years, 36% of patients had at least one symptom of long COVID (Li et al., 2022). Vision impairment and fatigue were the most common symptoms (Li et al., 2022).
In addition to the direct effects on the eyes and vision, COVID can also have indirect effects. For example, the pandemic disrupted healthcare, including eye care services such as routine eye examinations and management of chronic eye conditions. This disruption and delay of treatment potentially resulted in the progression of existing eye diseases and vision loss. From our findings, it is important that during regular health examinations the healthcare provider makes recommendations for eye examinations or provides vision screenings for long COVID patients. Healthcare providers should consider the recommendations in the “Post COVID Rehabilitation Response Framework” for a systematic approach to such care, including symptom screening and assessment, rehabilitation pathways, and self-management resources for patients (Manhas et al., 2022). As the newest subvariant, Arcturus (XBB.1.16), is highly contagious and causes conjunctivitis, eye care will be of particular importance and awareness is paramount.
Limitations
The association of long COVID with vision difficulties has been examined by only a few researchers with very small, and low-powered studies. In contrast, we presented the association using a recent and nationally representative dataset of the U.S. population living in households. The large data set and national representation strengthen our study, yet the survey instrument (HPS) includes only one generalized, non-specific question to define vision difficulties. Also, we were not able to assess whether the vision difficulties existed prior to COVID. Nevertheless, the study design precludes determination of causation; rather we have determined an association of long COVID and vision difficulties. There remains a need for more insight on the prevalence, risk factors, and long-term impact of COVID, including on vision difficulties. One such ongoing large-scale cohort study that may provide much needed information is the “The PRIME post-COVID” study (Pagen et al., 2022).
Conclusion
Nearly one-third of adults whose data were examined for the present study reported having difficulty seeing even while wearing glasses—this proportion was 48% among the individuals who experienced long COVID. Our findings reveal that those with long COVID had higher odds of experiencing vision difficulties compared to individuals who never had COVID, even after adjusting for potential confounding variables. We emphasize the need for further research with robust study designs to study the long-term impact of COVID on vision difficulties and subsequent vision care.
Supplemental Material
sj-docx-1-jvb-10.1177_0145482X251365588 - Supplemental material for Association of Long COVID With Vision Difficulties Among Adults in the United States
Supplemental material, sj-docx-1-jvb-10.1177_0145482X251365588 for Association of Long COVID With Vision Difficulties Among Adults in the United States by Mona Pathak, Sophie Mitra, Chan Shen, Hao Wang, Patricia A. Findley, R. Constance Wiener and Usha Sambamoorthi in Journal of Visual Impairment & Blindness
Footnotes
Author Contributions
Concept and design: all authors; acquisition of data: Usha Sambamoorthi; statistical analysis: Usha Sambamoorthi, Mona Pathak; interpretation of findings: all authors; drafting of the manuscript: Mona Pathak, Usha Sambamoorthi; critical revision of the manuscript for important intellectual content: Sophie Mitra, Chan Shen, Hao Wang, Patricia A. Findley, and R. Constance Wiener.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project described was supported by National Institute of Health/Artificial Intelligence/Machine Learning Consortium to Advance Health Equity and Researcher Diversity Grant # 1OT2OD032581-02 (Usha Sambamoorthi) and National Institute of General Medical Sciences, 5U54GM104942-07 (R Constance Winer). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.