
Abstract
Keywords
Among the many challenges faced by children and adolescents with visual impairments, difficulties in social skills are more frequently reported than among their sighted peers (Caron et al., 2021; Crocker & Orr, 1996; Huurre & Aro, 1998; McGaha & Farran, 2001; Ozkubat & Ozdemir, 2014). Since the visual system is the primary sensory channel that allows children to incidentally learn social skills, notably through observation and imitation (Bandura, 1977; Sacks & Silberman, 2000), children with visual impairments are particularly at risk for difficulties in this domain.
Social skills have been defined in several ways and there is no universal definition (Merrell & Gimpel, 2014). According to Gresham (2016), social skills refer to behaviors exhibited to complete social tasks that involve interacting with other individuals (for example holding a conversation, creating friendships, or playing a game with peers). With the aim of developing an empirical taxonomy of child and adolescent social competencies, Caldarella and Merrell (1997) conducted an extensive literature search and study selection process that resulted in a model including the following five most common social skills dimensions: Peer-Relation (e.g., positive behaviors toward peers, such as giving compliments or inviting others to play), Self-management (e.g., being emotionally well adjusted, controlling his or her own temper or receiving criticism well), Academic (e.g., being academically independent and productive), Compliance (e.g., get along with others by following rules and expectations), and Assertion (e.g., being self-confident, knowing how to initiate a conversation). This review highlighted that the dimensions Peer-Relation (52%) and Self-Management (52%) were the most frequently studied.
Different methodologies can be implemented to measure social skills, notably systematic observations, semistructured interviews, sociometric evaluations, self-assessment scales, role-play tests, problem-solving scenarios, and standardized behavior rating scales (Whitcomb, 2018). Among the scales focused on social skills assessment, the Social Skills Improvement System-Rating Scales developed by Gresham and Elliott (2008) is presumably the most used standardized behavior rating scale for youth. In addition, specific social skills scales have been developed for the population with visual impairments, in particular the Social Skills Assessment Tool for Children with Visual Impairments: Revised (SSAT-VI:R, (Sacks, 2014)) and the Social Competence Assessment (Loumiet & Levack, 1992).
Social skills are a key component for social participation and, more globally, for quality of life (Gresham, 2016). Many studies have shown that deficits in social skills can have a negative effect on the participation of children and adolescents in this population, with a higher risk of isolation and segregation at the forefront (Sacks & Wolffe, 2006). This effect can already be observed at an early age, and studies have reported that preschoolers with visual impairments tend to spend more time in solitary occupations and have fewer interactions with their peers than sighted children (Cappagli et al., 2018; Caron et al., 2021; Celeste, 2006), and stereotypic behavior such as eye-manipulation or auto-stimulation movements are more frequent (Molloy & Rowe, 2011). Among school-aged children, Salleh et al. (2011) have observed using the SSAT-VI:R that students with visual impairments had a lower score on basic social skills (especially for body language skills) than sighted students. As in other populations, a high correlation between social skills difficulties and behavioral problems has been reported in youths with visual impairments (Runjić et al., 2015). Regarding adolescents, although some studies report positive social experiences (Jessup et al., 2017), several studies highlight reduced social networks (Kef, 1997; Kroksmark & Nordell, 2001), fewer friends and dates than sighted peers, as well as frequent feelings of loneliness (Huurre & Aro, 1998; Rosenblum, 1998).
Furthermore, the effect can be observed throughout life, since adults with visual impairments are reported to have lower engagement in leisure activities (Alma et al., 2011; Salminen & Karhula, 2014), poorer employment rates (Gordois et al., 2012; Kelly, 2013; Wolffe & Candela, 2002), and increased loneliness (Brunes et al., 2019; Hodge & Eccles, 2014) that can be linked with deficits in social skills. Importantly, nowadays, having lower social skills may also affect social interactions at the digital level, since individuals with visual impairments face specific difficulties in the use of social networking sites (Brinkley et al., 2017).
Numerous studies have demonstrated the positive effect of implementing preventive interventions focused on social competence for at-risk children in social skills among various populations with special needs, such as autism spectrum disorders, intellectual disability, or learning disabilities (e.g., Gresham, 2016). Given the high rate of social skills difficulties and their aforementioned effects observed at all stages of development, it seems particularly relevant to implement such interventions for people with visual impairments. Although the scientific literature on this domain is still relatively limited for this population, a significant number of studies have implemented interventions focused on social skills and a systematic review of their effectiveness is lacking in the literature.
Even though no literature review has been conducted specifically on this question, two reviews provide important information on social participation and social support for individuals with visual impairments. The systematic review by Elsman et al. (2019) examined the effectiveness of rehabilitation interventions focused on increasing participation and quality of life. The effect on social skills performance was one of the eight outcome domains considered, with seven studies included. Only studies with a sample size of more than 10 participants were considered. No conclusion could be drawn about the effects of these social skills interventions due to the heterogeneity and the small amount of research. In their final conclusions, the authors stressed the need for future studies focusing on promising interventions where the efficacy is not yet clear, such as mobility and social skills. A second literature review (Manitsa & Doikou, 2020) concentrated on the types of social support delivered individually to students with visual impairments and no additional disability in educational institutions. Out of the 17 studies considered, the authors reported positive effects for 8 studies using educational interventions to improve diverse social inclusion domains for these students.
Despite the important contributions of these systematic reviews, they do not focus on social skills interventions. As a result, practitioners working with this population lack scientific evidence to decide which intervention to implement. In this article, the above-mentioned literature reviews will be complemented by focusing on interventions targeting social skills training in children or adolescents with visual impairments and by including single-case studies. In addition, the studies will be analyzed according to the social skill domain targeted by the interventions, with reference to Caldarella and Merrell's taxonomy (1997). The specific objectives of this literature review are as follows:
To identify studies that have implemented interventions focused on social skills training for children or adolescents with visual impairments; to evaluate the scientific quality of these studies using a standardized assessment tool; to outline the characteristics of the studies and of the interventions; and to analyze the outcomes of the interventions implemented and discuss evidence-based practice in this field.
Method
Search Strategy
The literature review was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines (Page et al., 2021). In order to identify relevant studies, the following electronic databases were consulted: Web of Science, OvidSP, EBSCOhost, SAGE Journals from 1983 up to 2020. The keywords used in the research were visual impairment, blind, blindness, low vision, visually handicapped, vision disorder, and deaf-blind combined with social skills, social skills training, social skills intervention, social interaction, social behavior, and social competence.
Inclusion and Exclusion Criteria
To be included in the review, each study had to be written in English, peer-reviewed, and published in academic journals. As established by the Population, Intervention, Comparison, Outcome, Time method (Hartmann et al., 2012), the following criteria were defined: The study population must be described by the authors as children or adolescents with visual impairments (i.e., blindness or low vision), aged 0–18 years, with or without additional disabilities (P); the intervention must be focused on or contain modules on social skills (I); a comparative intervention if available must be described (C); a measure of social skills must be required as an outcome (O); and the study must be published between 1983 and 2020—that is, after what has been identified as the first study on social skills in this population (Van Hasselt, 1982) (T).
Studies were excluded for different reasons: Lack of availability, noncorresponding population, data on participants with visual impairments could not be extracted separately from other participants with disabilities, the absence of social skills intervention, or absence of quantitative data following the intervention, or both. This process resulted in 1866 hits. After reading titles, 109 studies were retained as potentially relevant. Abstract reading and full reading led to the elimination of further hits, resulting in 44 studies. By eliminating duplicates, a total of 22 studies were found in the databases. Searching by other methods yielded 8 studies from the snowballing effect. Finally, a total of 32 studies were included in the review. Figure 1 presents the flowchart based on PRISMA guidelines and summarizes the procedure (Page et al., 2021).
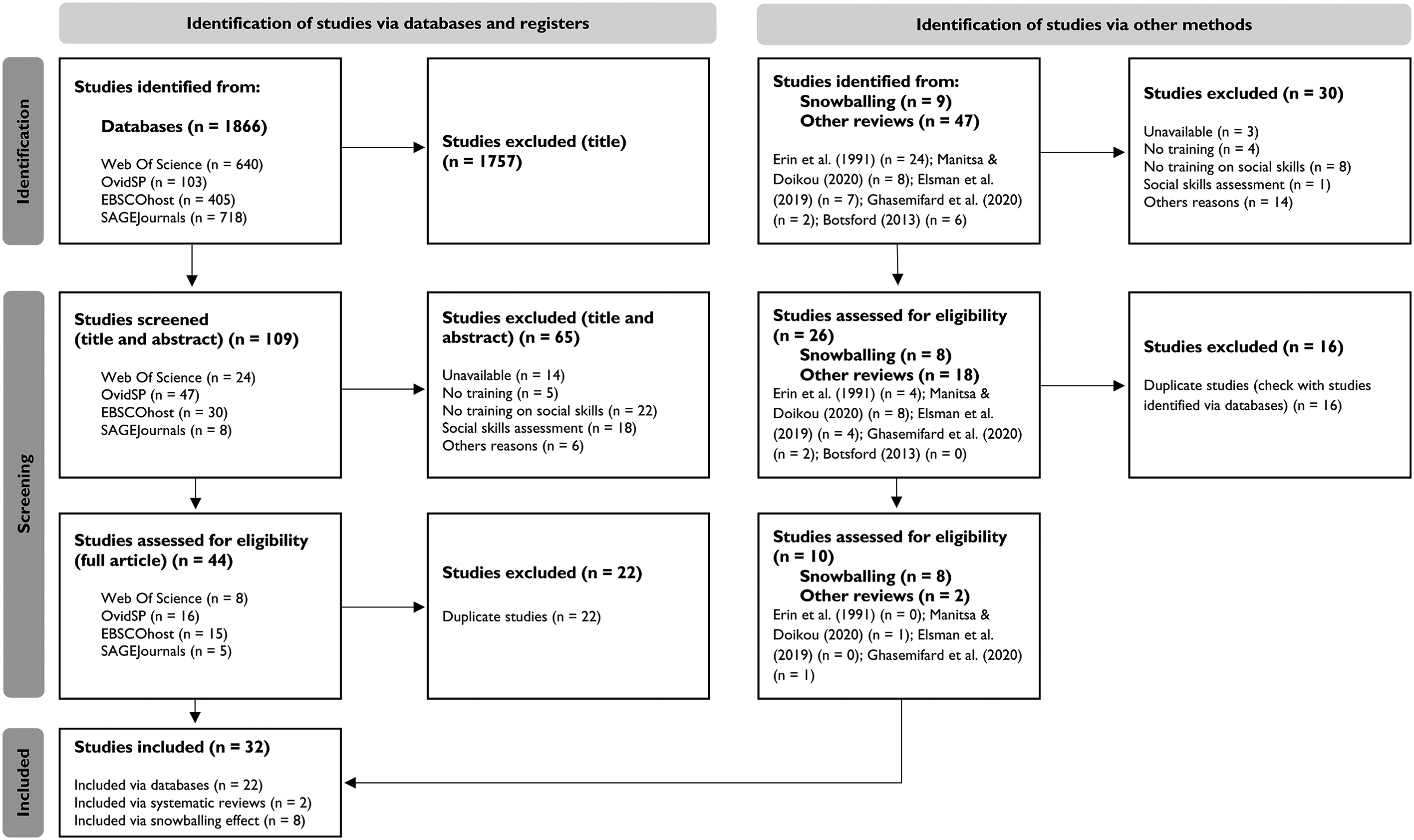
Flow chart of study inclusion process based on Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines (Page et al., 2021).
Data Extraction
A data form was used to extract key information from the studies. The main categories were the characteristics of the studies (author name, year of study, journal title, and country in which the study was conducted), the vision status of the target population, the methods and measures used to assess social skills, the characteristics of the intervention (setting, format, duration, content, and instructional strategies), and the effects of the intervention (types of analysis and outcomes).
Scientific Quality Assessment
Two instruments were used to assess the scientific quality of the selected studies: (a) The Quality Assessment Tool for Before-After (Pre-Post) Studies with No Control Group (National Heart Lung and Blood Institute, 2021) for group studies with experimental and quasi-experimental designs, and (b) criteria developed by Horner et al. (2005) for single-case design studies. The score obtained for each study was converted to a percentage and evaluated using the classification proposed by Cesario et al. (2002): High- (percentages between 75% and 100%), moderate- (50% to 74%), or low quality (25% to 49%).
Inter-Rater Agreement
To increase the accuracy of the systematic review and ensure inter-rater agreement, the following processes were performed by multiple researchers. The database search strategy was done by two researchers simultaneously. The data extraction from the studies was divided among three authors. In order to test the effectiveness of the data form and to ensure consistency in the data extraction process, data from 31.25% of the studies (n = 10) were extracted and compared by the three authors. The scientific quality assessment was carried out by two researchers on 25% of the studies (n = 8). For each study, the sum of the items in an agreement between the two researchers, divided by the total number of items, resulted in a score. The average of these scores resulted in an inter-rater agreement of 86% on four group studies and 83% on four single-case design studies.
Results
Characteristics of the Selected Studies
Country and Journal
Selected studies were published in several countries: United States (n = 16), the Netherlands (n = 4), India (n = 5), Turkey (n = 3), Canada (n = 1), Russia (n = 1), England (n = 1), and Italy (n = 1). The journal in which studies were most frequently published was the Journal of Visual Impairment & Blindness (n = 13).
Research Design and Population
The most frequently used research design was the single-case study (n = 17), followed by quasi-experimental (pre-post measures without control group) (n = 9), and experimental (pre-post measures with control group) (n = 6). Sample sizes were heterogeneous (between 1 and 52 participants with visual impairments, with an average of 12 participants). All studies taken together, a total of 397 participants with visual impairments aged between 3 and 20 years (M = 10.5 years, SD = 5.73) received a social skills intervention. The majority of the studies included children aged between 3 and 13 years, while only five studies included adolescents (between 14 and 18 years old).
In the selected studies, most participants were blind or had low vision (n = 30), while two studies did not report this information. Most of the selected studies (n = 16) included participants with visual impairments due to various etiologies, eight studies did not report information, and only four studies mentioned specifically the etiologies. Information about the presence or absence of cerebral visual impairment and visual acuity or field was not systematically reported.
Other Disabilities
Eight studies mentioned that participants had no other disabilities, while 10 studies mentioned other diagnoses, such as intellectual disabilities (n = 5 studies), deafness (n = 4), autism spectrum disorder (n = 2), multiple disabilities (n = 2), and cerebral palsy (n = 1).
Social Skills Assessment
To assess social skills at pre- and post-phase, behavior rating scales were used (n = 9) and filled out by different people such as parents or teachers. The scales used differed from study to study and were mostly developed by the authors with little information about their psychometric properties. Direct observation was used most frequently (n = 23); data were collected by different agents such as graduate students, an observation system, or the use of software. Observational measures were specific to each study, although some behaviors were frequently assessed (e.g., requests, gaze direction, conversational skills, turn-taking). Of the studies using observational methods, 80% mentioned the interobserver agreement procedure. Finally, a mixed method (combination of observations and a behavioral rating scale) was used in only one study. Table 1 summarizes the characteristics of the selected studies.
Characteristics of the 32 Reviewed Studies.
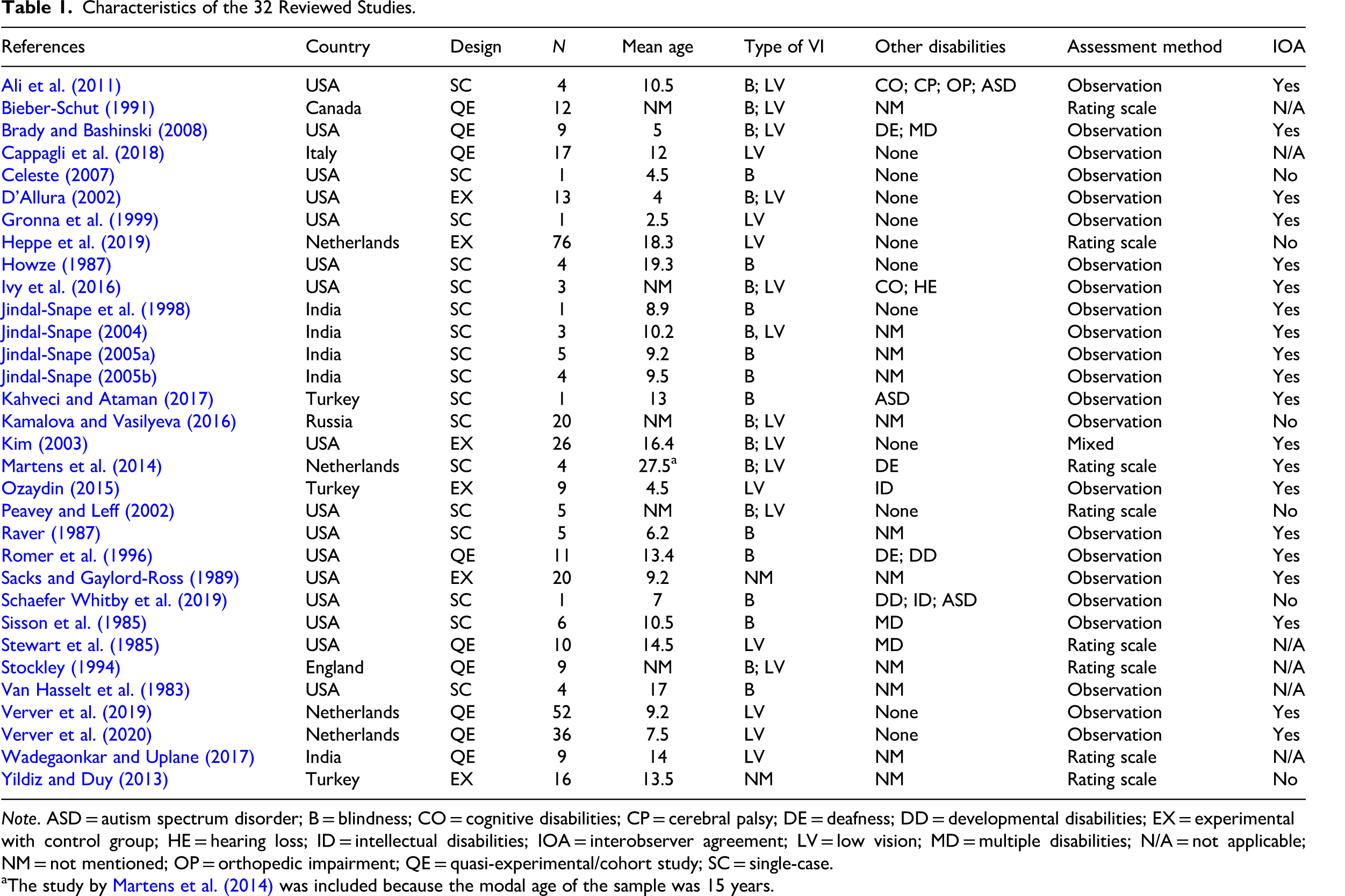
Note. ASD = autism spectrum disorder; B = blindness; CO = cognitive disabilities; CP = cerebral palsy; DE = deafness; DD = developmental disabilities; EX = experimental with control group; HE = hearing loss; ID = intellectual disabilities; IOA = interobserver agreement; LV = low vision; MD = multiple disabilities; N/A = not applicable; NM = not mentioned; OP = orthopedic impairment; QE = quasi-experimental/cohort study; SC = single-case.
The study by Martens et al. (2014) was included because the modal age of the sample was 15 years.
Scientific Quality Assessment
Quality ratings assigned to group studies (n = 15) are presented in Table 2, and quality ratings assigned to single-case design studies (n = 17) are presented in Table 3. Among the 15 studies evaluated with the Quality Assessment Tool for Before-After (Pre-Post) Studies with No Control Group (National Heart Lung and Blood Institute, 2021), six studies obtained a low-quality score, four studies a moderate-quality score, and five studies a high-quality score. Among the 17 studies evaluated according to the criteria of Horner et al. (2005), three studies scored low quality, one study scored moderate quality and 13 studies scored high quality.
Quality Assessment of Group Studies According to the 12 Criteriaa for Before-After (Pre-Post) Studies With No Control Group (NHLBI).
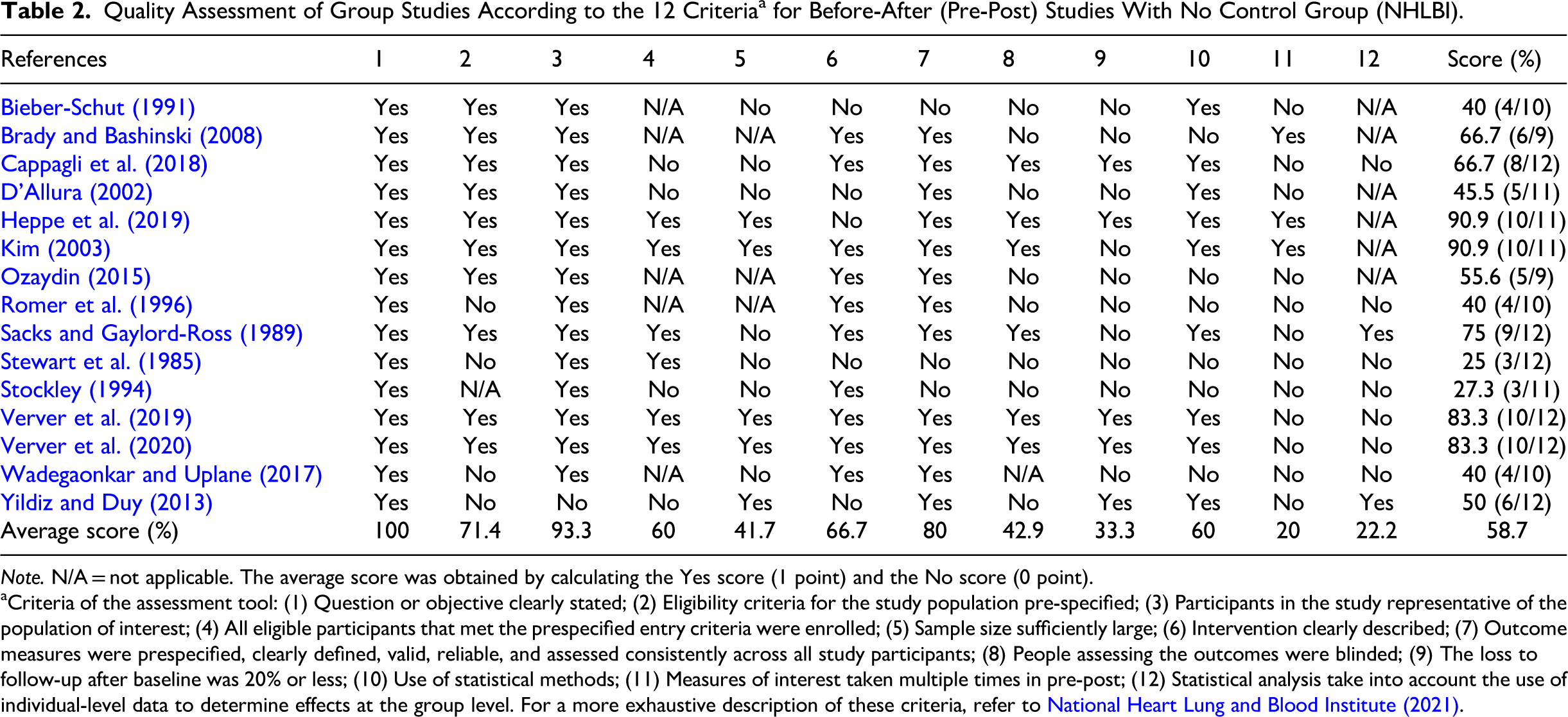
Note. N/A = not applicable. The average score was obtained by calculating the Yes score (1 point) and the No score (0 point).
Criteria of the assessment tool: (1) Question or objective clearly stated; (2) Eligibility criteria for the study population pre-specified; (3) Participants in the study representative of the population of interest; (4) All eligible participants that met the prespecified entry criteria were enrolled; (5) Sample size sufficiently large; (6) Intervention clearly described; (7) Outcome measures were prespecified, clearly defined, valid, reliable, and assessed consistently across all study participants; (8) People assessing the outcomes were blinded; (9) The loss to follow-up after baseline was 20% or less; (10) Use of statistical methods; (11) Measures of interest taken multiple times in pre-post; (12) Statistical analysis take into account the use of individual-level data to determine effects at the group level. For a more exhaustive description of these criteria, refer to National Heart Lung and Blood Institute (2021).
Quality Assessment of Single-Case Studies According to Quality Indicatorsa Within Single-Subject Research (Horner et al., 2005).
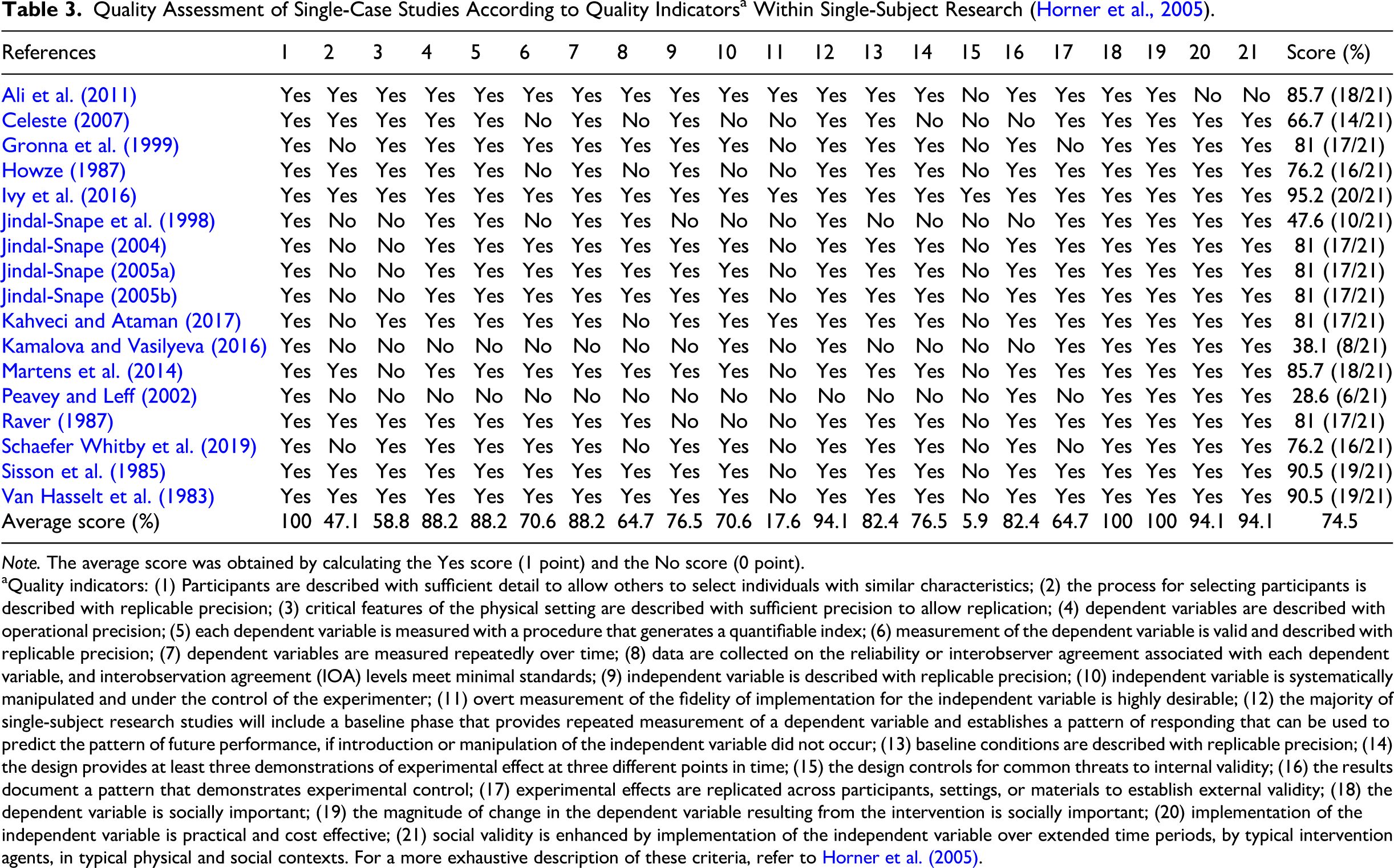
Note. The average score was obtained by calculating the Yes score (1 point) and the No score (0 point).
Quality indicators: (1) Participants are described with sufficient detail to allow others to select individuals with similar characteristics; (2) the process for selecting participants is described with replicable precision; (3) critical features of the physical setting are described with sufficient precision to allow replication; (4) dependent variables are described with operational precision; (5) each dependent variable is measured with a procedure that generates a quantifiable index; (6) measurement of the dependent variable is valid and described with replicable precision; (7) dependent variables are measured repeatedly over time; (8) data are collected on the reliability or interobserver agreement associated with each dependent variable, and interobservation agreement (IOA) levels meet minimal standards; (9) independent variable is described with replicable precision; (10) independent variable is systematically manipulated and under the control of the experimenter; (11) overt measurement of the fidelity of implementation for the independent variable is highly desirable; (12) the majority of single-subject research studies will include a baseline phase that provides repeated measurement of a dependent variable and establishes a pattern of responding that can be used to predict the pattern of future performance, if introduction or manipulation of the independent variable did not occur; (13) baseline conditions are described with replicable precision; (14) the design provides at least three demonstrations of experimental effect at three different points in time; (15) the design controls for common threats to internal validity; (16) the results document a pattern that demonstrates experimental control; (17) experimental effects are replicated across participants, settings, or materials to establish external validity; (18) the dependent variable is socially important; (19) the magnitude of change in the dependent variable resulting from the intervention is socially important; (20) implementation of the independent variable is practical and cost effective; (21) social validity is enhanced by implementation of the independent variable over extended time periods, by typical intervention agents, in typical physical and social contexts. For a more exhaustive description of these criteria, refer to Horner et al. (2005).
Characteristics of the Intervention
Table 4 presents a summary of the characteristics of the interventions and outcomes.
Characteristics of Interventions and Outcomes of the 32 Reviewed Studies.
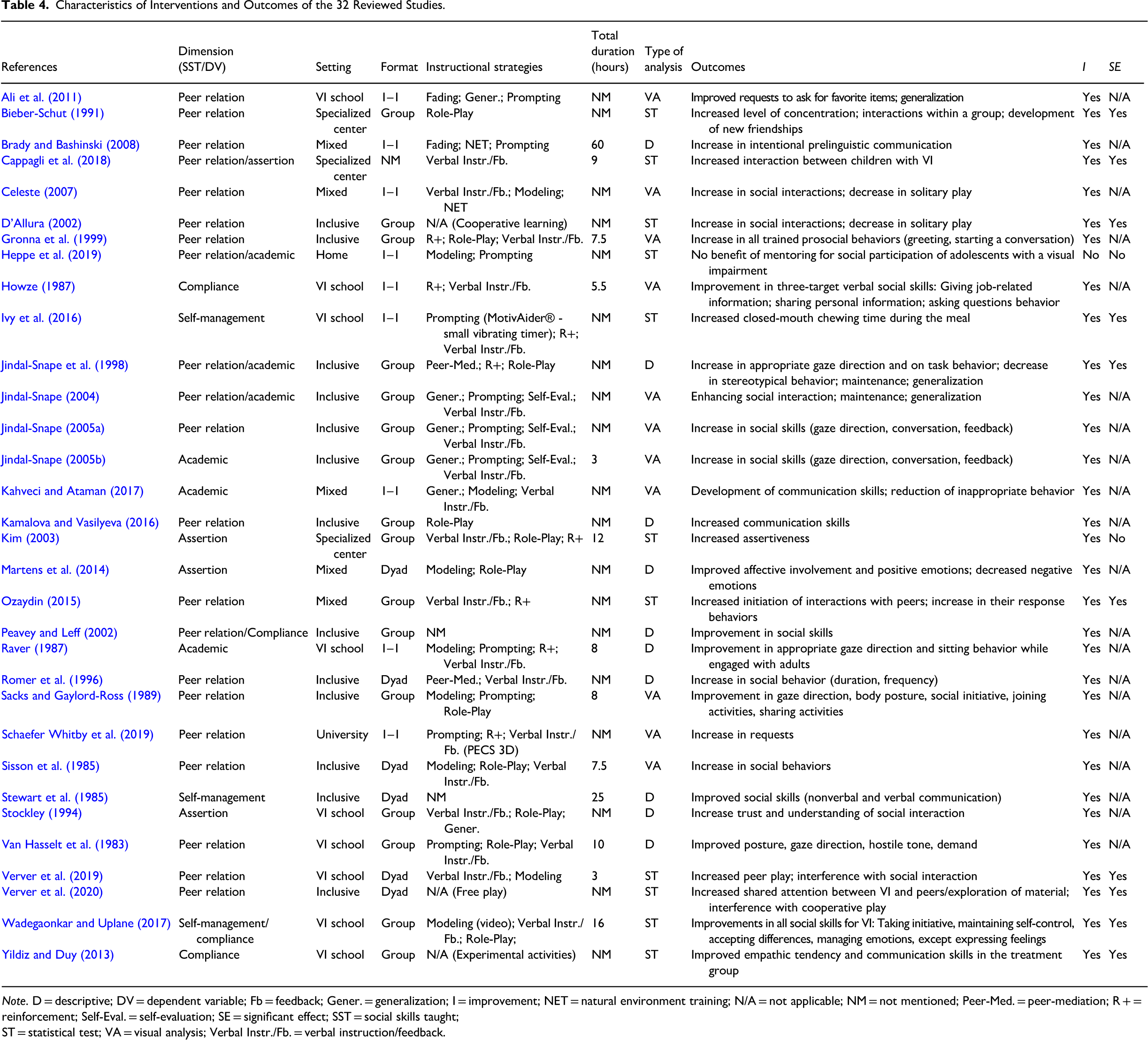
Note. D = descriptive; DV = dependent variable; Fb = feedback; Gener. = generalization; I = improvement; NET = natural environment training; N/A = not applicable; NM = not mentioned; Peer-Med. = peer-mediation; R + = reinforcement; Self-Eval. = self-evaluation; SE = significant effect; SST = social skills taught; ST = statistical test; VA = visual analysis; Verbal Instr./Fb. = verbal instruction/feedback.
Settings
The intervention programs took place in different locations such as schools for students with visual impairments (n = 9), inclusive schools (n = 13), specialized centers (n = 3), university clinic (n = 1), home (n = 1), and mixed settings including different locations (n = 5). Of the 32 studies reviewed, 10 included sighted children in the intervention.
Social Skills Targeted and Teaching Format
Categorization of the interventions was done according to Caldarella and Merrell's dimensions (1997). In several studies, skills from more than one dimension were taught. The majority of the studies targeted the domain of peer relation (n = 21), while the other domains were relatively less addressed: Self-management (n = 3), academic skills (n = 6), assertion (n = 4), and compliance skills (n = 4). Several teaching formats were present among the studies, such as group (n = 16), 1-to-1 teaching (n = 10) or dyad (n = 6).
Duration
The duration of social skills training varied considerably across studies. Depending on the study, the intervention was delivered between 1 and 5 times a week, and during 1–12 months. The total duration of interventions was reported in various ways (e.g., number of sessions, number of days, number of hours), and many authors did not report this information (n = 20). Among the 12 studies where the duration could be calculated, the average total amount of hours was 14 h (SD = 15 h, min 3 h, max 60 h), whereas most studies included between 1 and 10 h of total intervention time.
Instructional Strategies
The authors used a wide variety of intervention strategies to teach social skills goals. The most commonly used strategies were verbal instruction or feedback, prompting, role-playing, modeling, and peer mediation. Figure 2 shows the teaching strategies used in the selected studies.
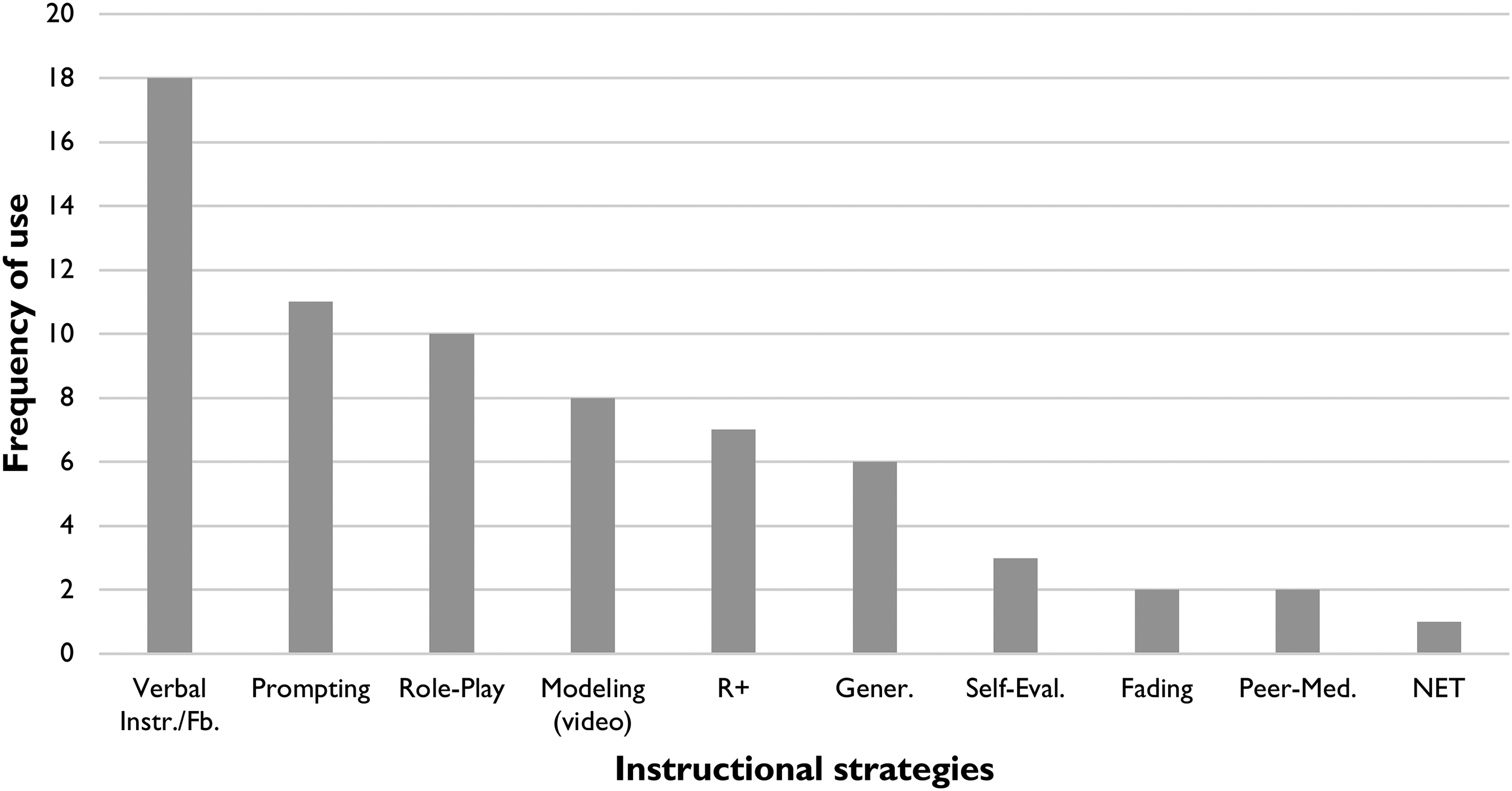
Frequency of instructional strategies used among the 32 studies reviewed. Note. Gener. = generalization; NET = natural environment training; Peer-Med. = peer-mediated; R + = reinforcement; Self-Eval. = self-evaluation; Verbal Instr./Fb = verbal instruction/feedback.
Effects of the Intervention
Type of Analysis and Effects
Among the 32 studies reviewed, 30 found improvement in the targeted social skills. Fifteen studies have analyzed data from group studies (with experimental and quasi-experimental design) and 17 from single-case design. Out of these 32 studies, 11 used statistical tests to evaluate the outcomes and 22 studies used descriptive or visual analyses or both. In the following, key findings regarding the effectiveness of the intervention in developing social skills are presented by using Caldarella and Merrell's (1997) dimensions and highlighting studies that were rated as high quality.
Peer-Relation Intervention (n = 21)
Of the 21 articles that targeted skills related to peer relation (10 group studies; 11 single-case design), 19 reported improvements in the social variables measured and two studies did not. For this dimension, 11 studies were rated as high quality. Among these, peer relationship interventions provided interesting results, such as an increase in requests (Ali et al., 2011); an increase in prosocial behaviors of greeting and initiating conversation (Gronna et al., 1999); an increase in social interaction, direction of gaze, and conversation (Jindal-Snape, 2004, 2005a, 2005b; Van Hasselt et al., 1983); and a reduction in inappropriate behaviors (Kahveci & Ataman, 2017). Two studies reported statistically significant positive effects in interventions using sound toys to increase peer relationship peer play and material exploration (Verver et al., 2019, 2020). Finally, the study by Heppe et al. (2019) compared two groups of young people (mean age: 18.3 years) with visual impairments who were participating in a community-based mentoring program, accompanied by mentors with or without visual impairments. Although the results regarding increased social participation were not significant, satisfaction with peer activities and perceived social support increased in both groups, but more so in the group accompanied by the mentor with visual impairment.
Self-Management Intervention (n = 3)
Three articles targeting self-management reported improvements through an intervention delivered by specialized teachers in school settings (two group studies; one single-case design). In the study by Ivy et al. (2016) that was rated as high quality, the prosocial behavior of chewing with the mouth closed was taught for 9 weeks to three children aged 1–14 years in the cafeteria setting of a school for children with visual impairments, using explicit instruction and prompting to promote self-talk during the meals. Results indicated a significant increase in intervals chewing with a closed mouth, and this behavior was maintained for up to one month after the intervention.
Academic Intervention (n = 6)
Of the six studies targeting skills on this dimension (one group study, five single-case design), five reported improvements in the social variables measured and one showed no effect. Five studies were classified as high quality, with various outcomes such as improvement in social interactions (Jindal-Snape, 2004, 2005b; Kahveci & Ataman, 2017), gaze direction (Jindal-Snape, 2005b; Raver, 1987), sitting behavior (Raver, 1987) and a decrease of inappropriate and stereotypic behaviors (Kahveci & Ataman, 2017).
Compliance Intervention (n = 4)
The four studies targeting skills on this dimension reported improvements in the dependent variables measured (two group studies; two single-case design). Howze (1987) investigated social skills training as a strategy for improving verbal behaviors in job interviews of four young adult males. Results indicated improvement in three targeted verbal social skills: Giving job information, sharing personal information, and asking questions.
Assertion Intervention (n = 4)
Of the four studies addressing assertiveness (three group studies; one single-case design), three reported improvements and two were rated as high quality. Kim (2003) investigated the effects of assertiveness training to enhance the social and assertiveness skills of 26 adolescents (mean age: 16.4 years) for 12 weeks. Results from social skills scales were compared and different perspectives were documented (youth, parents, and teachers). Although there were improvements after the intervention in all scores, only the results for the parents’ scales were significant. Similarly, Martens et al. (2014) investigated the effect of the Intervention Model for Affective Involvement with four participants (mean age: 27.5 years) and their 16 communication partners in three different settings (school, daytime activities center, and home) during 20 weeks of intervention. Following the intervention, affective involvement increased for three participants, while all four participants showed an increase in positive emotions.
Discussion
Hereafter will be discussed the main findings regarding the characteristics of the studies and interventions, as well as the effects of these interventions on social skills. In addition, the main results of the scientific quality assessment and the limitations of this systematic review will be highlighted.
Regarding the characteristics of the studies, the authors did not systematically provide information on visual status, etiology of visual impairment, presence of other disabilities, or general development assessed with a standardized scale. It is particularly relevant to carefully describe the participants, both in terms of their visual and developmental status (diagnosis and tools used to establish it), since it is an important quality criterion for individual case studies, allowing for replication by other practitioners and researchers implementing interventions with similar populations (Horner et al., 2005). Moreover, this review highlights that the focus of most studies is on childhood age. Considering the social difficulties faced by adolescents with visual impairments (Huurre & Aro, 1998; Kroksmark & Nordell, 2001), this age group deserves more attention in future research.
About the social skills targeted by the interventions, the most frequently targeted dimension was peer relationship (56% of studies), while self-management (8%), academic (17%), compliance (10%), and assertion (10%) were much less studied. Observations and non-validated behavior rating scales were used in most studies as assessment tools, and one study combined the two methods. Only a few studies mentioned the psychometric properties of the instruments used and interobservation agreement was not systematic. As recommended by Sacks (2014), it is essential to focus on already existing assessment tools with good psychometric qualities (see Cordier et al., 2015 for a review). In future research, as suggested by Riley-Tillman and Burns (2009), target behavior or social skill of interest must be accurately reported, operationally defined, and ideally measured by more than one person in order to provide data on the inter-rater agreement process.
Concerning the interventions, several instructional strategies have been used to teach social skills, the most common being verbal instruction, prompting, and role play. Several studies did not meet the quality criteria regarding the detailed description of the intervention (Horner et al., 2005), as for example information on dosage (or duration of the intervention) or on the training of the implementers was frequently missing. Consequently, the fidelity of the interventions described was often not measurable. This criterion, which verifies whether the intervention was implemented as planned, is particularly important for interventions that are subject to a great deal of implementation variability (Horner et al., 2005).
Regarding the effects of intervention, most of the studies analyzed in this review (n = 30) reported an improvement in the social skills targeted by the intervention. The majority of the studies (n = 20) used descriptive and visual analysis to assess the outcomes and 11 studies used statistical tests. No study used a longitudinal design to assess the impact of interventions, a shortcoming in visual impairment research already pointed out by Bonfigliuoli et al. (2010).
The scientific quality assessment showed an average rate of 58.7% for group studies, corresponding to moderate overall quality. Among the methodological strengths of the studies analyzed, the following should be noted: Accurate description of the objectives, representativeness of the study participants, and a clear, valid, and reliable outcome measure performed among the participants. However, some general methodological weaknesses were present, such as the lack of measures of interest taken multiple times in the pre-post phases and statistical analysis taking into account the use of individual-level data to determine group-level effects. For single-case design studies, the average score of 74.5% in the scientific quality assessment corresponds to overall high quality. Several strengths were identified, such as accurate description and reliable measurement of the dependent variable, presence of an accurate and reproducible baseline, results demonstrating experimental control, and consideration of the social importance of the intervention. Nevertheless, there are two shortcomings, since most studies do not control for threats to internal validity and lack an overt measurement of implementation fidelity.
Interpretation of the results should be done with caution given the various limitations of this systematic review. First, the database selected and the language considered may exclude relevant studies, especially since it is quite common in this field for scientific works to be published in the local language. Another limitation concerns the scientific quality assessment scale used for group studies, which is not specific to the evaluation of studies published in the field of special education. Furthermore, the great heterogeneity of participants (e.g., various visual status, presence of comorbidities) was not considered in the analysis. In particular, the presence of participants with deafblindness, given their unique communication needs, may constitute a bias in the interpretation of the overall results. Finally, the inclusion criteria for interventions and assessment methods were very broad. This choice was justified by the small number of studies on this topic. Consequently, the application of these criteria generates very broad results and does not allow solid conclusions on the effects of a single type of intervention to be drawn.
Conclusion
This review analyzed the content and effects of social skills interventions for youths with visual impairments. The majority of the 32 studies reviewed reported improvements in social skills after the implementation of an intervention. Despite the general methodological limitations highlighted in the discussion, the results are encouraging and open the door for further research on the assessment and teaching of social skills to children and adolescents with visual impairments.
Practical Implications
Given the high rate of social skills difficulties reported in this population and the effect of these difficulties on all stages of development, it seems particularly relevant for practitioners to integrate social skills assessment and explicit teaching into intervention programs. This review highlights various ways of assessing and teaching social skills to children and adolescents with visual impairments in different intervention settings.
Future Research
To summarize the key insights for future research in this area, this systematic review points to several important gaps that need to be addressed: The underrepresentation of the adolescent population, the lack of longitudinal studies, the need for interventions targeting all social skill domains (rather than focusing solely on peer relationships), and larger sample sizes. More detailed information regarding the description of the participants is needed, such as the type and degree of additional disabilities, the communication and language abilities, and the presence or degree of cerebral visual impairment. In general, the validation of standardized scales, as well as the development of interventions and the evaluation of their effects through multicenter (international) studies seem necessary. In the future, researchers, stakeholders, and practitioners should work together to design, implement, and evaluate evidence-based interventions directed at improving the social skills of students with visual impairments.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.