
Abstract

Professionals providing educational services to individuals with visual impairments or deafblindness are often consulted about the behavior of these individuals with multiple disabilities. An area of specific interest is the possible presence of autism spectrum disorders (hereafter, autism) in this population. Autism is a developmental disorder characterized by impairments in social communication, interaction, and restricted and repetitive behavior patterns or stereotyped behavior (American Psychiatric Association, 2013). Behavioral characteristics that are typical for autism are also prevalent in individuals with combined intellectual disabilities and visual impairment or deafblindness (Belote & Maier, 2014; Dammeyer, 2014; de Vaan et al., 2013; Evenhuis et al., 2009; Hoevenaars-van den Boom et al., 2009; Probst & Borders, 2017). Both autism and deafblindness affect the way sensory information is accessed and processed. As Dammeyer (2014, p. 1095) pointed out, “The main consequences of congenital sensory impairment, being barriers for communication, language and social interaction development, may lead to symptoms of autism.” For example, in the area of communication and interaction, both an intellectual disability and a visual impairment can cause a delay in the development of language or odd language use, especially for social purposes (Tadić et al., 2010; Tager-Flusberg et al., 2005; Warren, 1994). A visual impairment, and particularly blindness, can also lead to difficulties in nonverbal communication, such as the inability to make eye contact, follow gaze direction, and perceive facial expressions and gestures. Individuals with intellectual disabilities also show stereotypical behaviors frequently (Militerni et al., 2002). Examples of such behaviors are fidgeting with hands and fingers, rocking the body, and moving the head. In persons with visual impairment and deafblindness, specific stereotyped behaviors are also frequent, such as eye poking or pressing and echolalia (Tröster et al., 1991), notwithstanding that these behaviors may serve a completely different purpose in individuals who are blind than in persons with autism (Andrews & Wyver, 2005; Probst & Borders, 2017). A comprehensive overview of overlapping characteristics is given by Belote and Maier (2014).
Difficulties in diagnosing autism
Because of the topographical overlap in behavioral characteristics, it can be difficult to diagnose autism in this complex group of individuals with combined sensory and intellectual disabilities (for an overview, see Thurm et al., 2019). Several diagnostic instruments and tools for screening for autism are available. Two of the most widely used instruments are the Autism Diagnostic Observation Schedule (Lord et al., 1999) and Autism Diagnostic Interview–Revised (Rutter et al., 2003). Some instruments are even specifically developed for use with people with intellectual disabilities, such as the Pervasive Developmental Disorder in Mental Retardation Scale: (PDD-MRS; Kraijer, 1999). However, there are no instruments for screening and diagnosing autism in individuals with intellectual disabilities combined with visual impairment or deafblindness. In fact, widely used instruments in the diagnostic process of autism appear unsuitable for this target population due to a lack of norms and many nonapplicable and unsuitable items. The latter stems from a sensory bias in item construction, where items do not consider that sensory impairments could lead to the same behavior as autism (de Vaan, Vervloed, Hoevenaars-van den Boom et al., 2016).
The development and use of Observation of Autism in People with Sensory and Intellectual Disabilities (OASID)
To address the validity issues, OASID (de Vaan, Vervloed, Peters-Scheffer, et al., 2016; de Vaan et al., 2018; de Vaan, Vervloed, Knoors & Verhoeven, 2019) was recently developed. OASID is specifically developed for the population of individuals with moderate to profound intellectual disabilities, combined with visual impairments or deafblindness. It is an elaboration of the Observation of Characteristics of Autism in Persons with Deafblindness of Hoevenaars-van den Boom et al. (2009) that was designed for people with deafblindness and profound intellectual disability. All items consider sensory and intellectual disabilities during the administration of items and interpretation of behavior. OASID consists of a semi-structured play session. Sessions last between 30 and 60 min and consist of five tasks administered in a playful manner. The administrator can adjust the type and level of both communication and play to the participant’s individual possibilities and impairments. For example, it was asked if the participant responded to initiations for contact or sought the researcher’s attention, whether by eye contact or alternative means if the participant was blind. Additional examples of seeking contact in an alternative way were given (e.g., “taking the researcher’s hand” or “talking to the researcher”). Figures 1 –3 show examples of this process using a simple shape puzzle for which the level of difficulty varies. There are four different degrees of difficulty that could be adjusted to the participant’s cognitive and motor abilities. Communication about the puzzle was achieved through spoken language, sign language, tactile sign language, or by simply presenting puzzle pieces, depending on the participant’s communication style.

Puzzle Levels 1 and 2 can be played with or without the lid. Contains symmetrical shapes only.

Puzzle Level 3 contains symmetrical and asymmetrical shapes.

Puzzle Level 4 contains more complex pieces besides the symmetrical and asymmetrical shapes.
The administrator will offer the puzzle to the participant and invite him to play with it. First, the participant explores the puzzle, and then the administrator will invite the participant to play together. Table 1 shows two example questions and scoring rules for “no,” “mild,” and “severe” behavior typical in autism. In total, there are 40 items to be scored for the five tasks. The last 11 items do not concern a specific task but ask for reflection on the assessment in general. Items had three possible scores, ranging from 0 to 2, reflecting absent, intermediate, or full presentation of features of autism. To keep the presentation of items as standard as possible, it was decided not to change materials within an item depending on the age of the participant. Although it might seem that some of the materials are not age-appropriate for older participants, there were no problems with any of the toys, not even with participants with only moderate intellectual disabilities.
OASID example items.
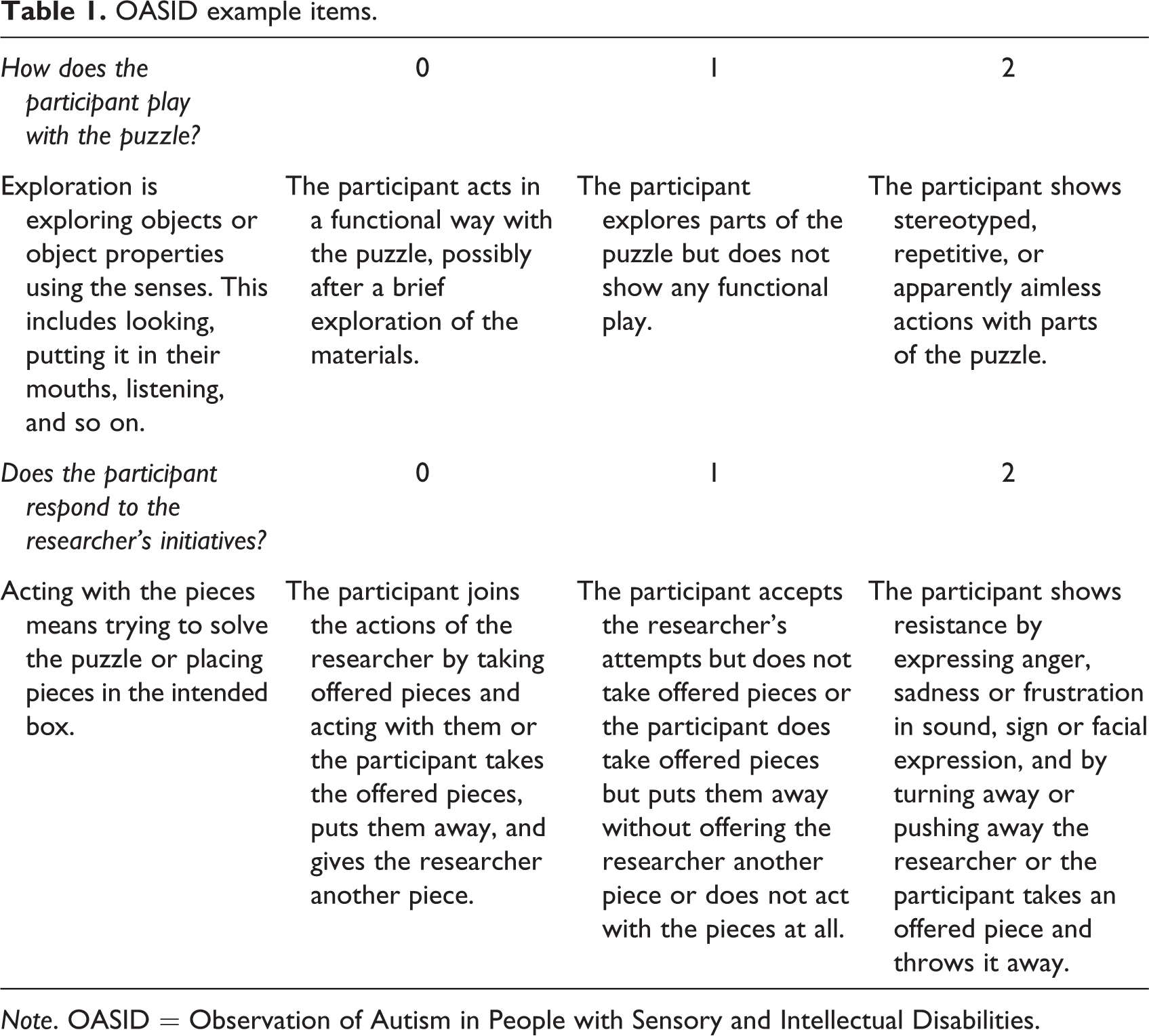
Note. OASID = Observation of Autism in People with Sensory and Intellectual Disabilities.
An important strength of OASID is that the administration is not stressful. Stress was measured by comparing three samples of saliva cortisol levels on the test day and comparing it to a control day (de Vaan, Beijers, et al., 2020). Anecdotal information showed that most participants even enjoyed the assessment. OASID is scored off-line (i.e., afterward) using the video recording of the session. Scoring of the session lasts about 30–90 min per participant. Direct online scoring is not recommended because diffuse on- and offset of behaviors make it hard to score items directly. Off-line, one can rewind the video recordings.
Scoring rules of OASID are based on the Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5). Contrary to most instruments, where item scores add up to one total score, OASID works with two total scores on two separate domains: “social behavior and communication” and “repetitive and stereotyped behavior.” These scales are in line with the diagnostic criteria and domains for autism in the DSM-5. Symptoms in both of these domains have to be present in order to be diagnosed with autism (American Psychiatric Association, 2013). The manual has specific reference points that correspond with specific interpretations regarding the severity of autism symptoms (de Vaan et al., 2018). Additionally, similar to the DSM-5, OASID takes into account that autism symptoms occur on a spectrum instead of on a dichotomy. Therefore, OASID scores lead to an interpretation of no, mild, severe, or profound autism symptoms instead of only a label of autism or no autism.
Psychometric properties
Two studies established the psychometric properties of OASID, a pilot study with 18 participants and a follow-up study with 60 participants. Both studies showed that OASID was able to differentiate between participants with few symptoms of autism and participants with many symptoms of autism (de Vaan, Vervloed, Peters-Scheffer, et al., 2016; de Vaan et al., 2018).
These studies showed good inter-rater reliability (correlations ranged from 0.82 to 0.93, with an intra-class correlation of 0.63) and excellent intra-rater reliability (89% exact agreement and weighted kappa = .89) and a good internal consistency of the scales (Crohnbach’s alpha = .91 and .85 for, respectively, the scales “Social Behavior and Communication” and “Repetitive and Stereotyped Behavior”). The construct validity was established by comparing OASID to other instruments that measure the same construct (convergent validity), namely the PDD-MRS (Kraijer, 1999) and the Childhood Autism Rating Scale, second edition (CARS-2; Schopler et al., 2010). A small significant correlation was found between total scores on OASID and the PDD-MRS, ρ = .243, p = .038. The total scores on OASID were moderately to highly significantly correlated with the total scores on the CARS-2 for two observers, ρ = .652, p < .001, and ρ = .801, p < .001, respectively. OASID was also compared to an instrument measuring a different construct (divergent validity) that can lead to similar symptoms: attachment problems, measured with the list of behavioral signs of disturbed attachment (Boris & Zeanah, 2005). As desired, there was no significant correlation between OASID scores and the list of disturbed attachment, r = 0.46 (p = .57). Finally, sufficient criterion validity was found by comparing OASID results to independent judgments of two experts in the field. There was a moderately strong Spearman-rank correlation between OASID scores and the ranks formed by the combined expert judgments regarding the presence of autism, ρ = .67, p < .001 (de Vaan, Vervloed, Peters-Scheffer, et al., 2016; de Vaan et al., 2018).
Recommendations for clinical practice
The manual for OASID is freely available for use in clinical practice for professionals working with people with a moderate to profound intellectual disability combined with a visual impairment or deafblindness (de Vaan et al., 2019). At this moment, no specific training or certificate is required to administer OASID. However, it is recommended that only professionals with sufficient diagnostic training and knowledge and experience with the target population use OASID. Preferably, the consensus judgment of two experts is reached. Before using OASID, it is important to study the manual thoroughly, collect a set of material that is the same or closely similar to the original materials depicted in the manual, and practice the administration beforehand.
It is important to realize that OASID only gives an indication of the presence and severity of autism symptoms, and it does not replace a full diagnostic assessment. Along with the recommendations of the Dutch Psychiatric Association (2009) and American Psychological Association (2019), a full diagnostic assessment of autism should always include a broad assessment, looking at all problematic behaviors and possible concerns, history taking, multiple tests, and behavioral observations, more than one informant and a multidisciplinary assessment team (Carnaby, 2007; Oosterling et al., 2010). Ideally, clinical judgment is supported by diagnostic instruments, of which OASID can be one. Finally, for a proper classification of autism, it is important to develop a full profile of the individual, including strengths and weaknesses, case history, sensory assessments, intelligence, and other potentially presenting disorders (Dutch Psychiatric Association, 2009).
Conclusion
OASID is a semi-structured observational assessment that can indicate the presence and severity of autism symptoms in individuals with moderate to profound intellectual disabilities combined with a visual impairment or deafblindness. Strengths of OASID are that it takes into account and adjusts for sensory impairments, something that current widely used instruments for the diagnosis of autism are unable to do. Additionally, the assessment was found not to be stressful for participants, and OASID was found to be valid and reliable. The scoring and interpretation of OASID is in line with the most recent definition of autism described in the DSM-5.
Footnotes
Authors’ note
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by grants to Mathijs P. J. Vervloed by Royal Visio, Bartiméus, Royal Kentalis, ZonMW (# 94308001), Stichting tot verbetering van het lot der Blinden, and the Behavioural Science Institute of Radboud University.