
Abstract
Nonsuicidal self-injury (NSSI) by proxy is the intentional destruction of one’s own body tissue through the elicitation of another being’s actions. Despite its clinical relevance, research on NSSI by proxy is limited and there are no available measures of this behavior. This research aimed to characterize NSSI by proxy among young adults and provide preliminary data on the validity of a new self-report measure, the NSSI by Proxy Questionnaire (NSSIBPQ). Two nationwide community samples of young adults (one general community sample and one with a history of traditional NSSI and suicidality) completed online studies. NSSI by proxy was reported by 18% of the general community sample and 45% of the self-injuring sample. Findings support the clinical relevance of NSSI by proxy and its potential to meet criteria for an NSSI disorder diagnosis. Results also provide preliminary support for the internal consistency and convergent, discriminant, and concurrent validity of the NSSIBPQ.
Introduction
Nonsuicidal self-injury (NSSI) is the deliberate destruction of one’s body tissue without suicidal intent and for purposes not socially sanctioned (Chapman et al., 2006; Gratz, 2001; International Society for the Study of Self-Injury, 2018; Nock, 2009). Prototypical NSSI behaviors include cutting, burning, skin-carving, and severe scratching. Although rates of NSSI among the general population range from 3% to 6% (Klonsky, 2011; Liu, 2023; Plener et al., 2016; S. V. Swannell et al., 2014), rates are higher among adolescents (17%–27%; Monto et al., 2018; S. V. Swannell et al., 2014; Zetterqvist et al., 2021), young adults (13%–18%; Kiekens et al., 2023; S. V. Swannell et al., 2014), and clinical populations (11%–81%; Auerbach et al., 2014; Clarkin et al., 1983; Gunderson & Ridolfi, 2001; Selby et al., 2012). Further, NSSI is a behavior of considerable clinical concern. Specifically, in addition to the fact that NSSI may result in clinically significant distress and functional impairment (Gratz et al., 2015), this behavior has been found to have strong prospective associations with both suicide attempts and death by suicide (Asarnow et al., 2011; Franklin et al., 2017; Guan et al., 2012; Ribeiro et al., 2016). Moreover, recurrent NSSI was included as a “condition for further study” within the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; American Psychiatric Association, 2013), with the diagnostic criteria for NSSI disorder (NSSID) including engagement in NSSI on at least 5 days in the past year (Criterion A); the expectation that NSSI will regulate emotions and/or resolve interpersonal difficulties (Criterion B); the experience of negative feelings or thoughts immediately prior to NSSI, and/or preoccupation with or frequent thoughts related to NSSI (Criterion C); and the presence of significant distress or impairment (Criterion E), among others.
Although inclusion of NSSID within the DSM-5 is expected to bring additional attention to NSSI as a clinical concern in need of targeted intervention and investigation (Wilkinson & Goodyer, 2011), the potential clinical and research benefits of this diagnosis will be limited to the extent that overly restrictive definitions of NSSI result in the exclusion of clinically significant NSSI behaviors. For example, Green and Jakupcak (2016) have identified how relevant NSSI behaviors more common among men (e.g., wall/object punching) have often been overlooked in the literature and excluded from NSSI assessment instruments, resulting in an underestimation of the prevalence of NSSI among men (see Kimbrel et al., 2018). Likewise, current operational definitions of NSSI have generally excluded behaviors that, while self-directed and associated with self-injurious intentions, are not self-inflicted (i.e., NSSI by proxy). Notably, however, recent literature has called attention to the clinical relevance of this form of NSSI, documenting NSSI by proxy as an important form of NSSI in need of further empirical and clinical attention (see Mann et al., 2022).
Specifically, NSSI by proxy has recently been defined as the deliberate destruction of one’s own body tissue through the elicitation of another being’s (e.g., human, animal) actions that is absent of suicidal intent and for purposes not socially sanctioned (Mann et al., 2022), including behaviors such as initiating injury via tattooing or body piercing (performed by a trained professional), via an animal (e.g., by purposely provoking a pet to bite or scratch themselves), or by instigating a physical fight. Although the use of another being to inflict the injury allows for an external attribution of the injury, this behavior is conceptualized as self-driven because of the agency of the person being injured in initiating, continuing, and terminating the behavior, as well as determining the specific nature of the injury (e.g., when, where, duration, etc.). Moreover, NSSI by proxy may also meet the criteria for NSSID described above, as this behavior is often described as being used to regulate emotions or resolve interpersonal difficulties (Criterion B); is often preceded by interpersonal difficulties or negative thoughts or emotions and/or associated with preoccupation with or frequent thoughts about the self-injury (Criterion C); and may, with repeated engagement, result in clinically significant impairment and/or distress (Criterion E). Finally, clinical consideration of NSSI by proxy is even more important given the topographical similarities of NSSI by proxy (vs. traditional NSSI) to socially sanctioned behaviors (e.g., tattoos, sports injuries), which may obscure the self-injurious intentions of the behavior and increase the likelihood that it will be overlooked, understudied, and undertreated. Thus, given that NSSI by proxy is a clinically relevant behavior that has historically been overlooked in research on and assessment of NSSI, further consideration of this behavior as a distinct form of NSSI is needed.
A recent conceptual paper by Mann et al. (2022) proposed six behaviors that may be conceptualized as NSSI by proxy, including initiating injury (1) via tattooing and body piercing, (2) via an animal, (3) via sexual activity with a partner, (4) by instigating a physical fight, (5) via sports, and (6) by engaging in elective or cosmetic medical procedures. Notably, all of these behaviors are similar in that they require an “other” to cause the injury (e.g., a tattoo artist, sexual partner, a pet), are self-directed, and have been described by patients and participants in clinical and empirical literature as having self-injurious intentions. Yet, despite recognition of these six behaviors as potentially clinically significant forms of NSSI, there are currently no available measures of NSSI by proxy or its associated characteristics. In order to advance research on NSSI by proxy, an empirically-supported and psychometrically sound assessment instrument for this behavior is needed.
Indeed, the development of an empirically-supported measure of NSSI by proxy has a number of important research and clinical applications. First, such a measure is necessary for the systematic progression of research in this area, including research on the prevalence of NSSI by proxy (in both the general population and specific clinical populations) and how common this behavior is relative to other health risk behaviors (e.g., traditional NSSI, substance use, suicidal behaviors). A comprehensive measure assessing not just the presence and frequency of specific NSSI by proxy behaviors but their associated characteristics (e.g., emotional and cognitive antecedents of and motives for these behaviors) could also help clarify the extent to which NSSI by proxy behaviors may qualify for a NSSID diagnosis, as well as how this particular form of NSSI fits within contemporary models of traditional NSSI (e.g., the experiential avoidance model of NSSI; Chapman et al., 2006) and other self-injurious behaviors (e.g., models identifying NSSI as a risk factor for suicidal behaviors; see Hamza et al., 2012). Finally, development of a psychometrically sound, comprehensive measure of NSSI by proxy also has important clinical implications, ensuring a more complete assessment of clinically relevant NSSI behaviors in clinical settings and, thus, facilitating identification of clinically relevant treatment targets and clinically indicated treatments. Such a measure also has the potential to improve clinical practice by providing a more accurate assessment of the scope of a client’s NSSI at different stages of the treatment process and helping clinicians differentiate clinically relevant NSSI by proxy behaviors from normative/non-pathological behaviors that are topographically similar but either not intentional (e.g., accidental animal bite) or associated with socially sanctioned motives (e.g., tattooing for self-expression).
Present Study
The present study extends the extant literature on NSSI through the development and initial validation of a questionnaire assessing the novel yet overlooked behavior of NSSI by proxy—a behavior that has generally been excluded from most extant NSSI measures. Specifically, the NSSI By Proxy Questionnaire (NSSIBPQ) was developed to assess not only the presence and frequency of a variety of clinically important yet under-examined NSSI by proxy behaviors, but characteristics of these behaviors relevant to an NSSID diagnosis, including the emotional and cognitive antecedents of and motives for these behaviors and preoccupation with and thoughts about these behaviors. This measure was examined in two community young adult samples, including one selected for a history of NSSI and suicidality.
This research had two aims. The first was to provide initial data on this understudied form of NSSI by detailing the rates, frequency, and associated characteristics of NSSI by proxy in these two samples, as well as the extent of the co-occurrence of NSSI by proxy with traditional NSSI. Differences in rates of NSSI by proxy as a function of relevant demographic characteristics (e.g., sex assigned at birth, gender identity, sexual identity, racial/ethnic background, age, annual household income, education, and U.S. geographical region of residence) were also examined. The second aim was to provide preliminary data on the internal consistency and convergent, discriminant, and concurrent validity of the NSSIBPQ by examining the associations of lifetime NSSI by proxy frequency on this measure with the lifetime frequency of traditional NSSI (relative to other health risk behaviors) and other relevant clinical constructs theoretically and empirically linked to NSSI, including suicidal ideation and planning, psychiatric symptoms, and emotion regulation difficulties.
Development of Scale Content
The specific NSSI by proxy behaviors to be assessed were identified based on the clinical experience of the authors with self-injuring patients (and repeated observations of NSSI by proxy within this population), as well as a comprehensive review of extant empirical and clinical literature on NSSI by proxy and related constructs, including traditional NSSI, sex as self-injury (SASI), indirect self-injurious behaviors (e.g., disordered eating, alcohol misuse), and other DSM-5 disorders (e.g., body-dysmorphic disorder, sexual masochism disorder, and factitious disorder). Specifically, relevant NSSI by proxy behaviors were initially identified via a detailed review of relevant clinical cases of the authors (the latter two who are experts in the treatment of self-injury), as well as published case studies and clinical descriptions in the literature (see, e.g., Anderson & Sansone, 2003; Mann et al., 2020; Møhl, 2019). This review resulted in the development of the initial parameters of the construct and a list of potential NSSI by proxy behaviors, which were further refined based on a comprehensive review of the empirical literature on NSSI by proxy and related behaviors. This review and the resultant conceptual definition of NSSI by proxy on which the NSSIBPQ is based are described in Mann et al. (2022).
Following identification of the NSSI by proxy behaviors of interest, items were developed to assess the frequency and age of onset of each behavior. These items were modeled after the Screen for Nonsuicidal Self-Injury (SNSI; Halverson et al., 2022), which assesses the lifetime and past-year presence and frequency, as well as the age of onset, of a variety of traditional NSSI behaviors. Next, given the expectation that NSSI by proxy behaviors may also meet criteria for NSSID (Mann et al., 2022), and to ensure a comprehensive assessment of the associated characteristics of NSSI by proxy relevant to an NSSID diagnosis, items were generated to assess the motives for, emotional and cognitive antecedents of, and preoccupation with and thoughts about these behaviors. These items were based on items drawn from the Clinician-Administered Nonsuicidal Self-injury Disorder Index (CANDI; Gratz et al., 2015), an empirically supported structured diagnostic interview for NSSID, supplemented by additional interpersonal motives informed by the theoretical and empirical literature on related constructs that similarly include another person in an injurious act (e.g., SASI; Fredlund et al., 2020). Specifically, items assessing the motives for NSSI by proxy behaviors captured the following motives: to decrease or distract from negative thoughts or emotions, to relieve tension, to generate positive emotions, to counteract feelings of numbness, to relieve boredom, to punish oneself, to establish a sense of control, to avoid attempting suicide, to influence others, to communicate to others, to receive help or attention from others, to feel sexual pleasure, to feel special, important, or needed, to get help from others, and to confirm or verify how bad things are. Likewise, items assessing the emotional and cognitive antecedents of NSSI by proxy assessed a variety of emotional and cognitive states, including sadness-, anger-, anxiety-, hurt-, shame-, and happiness-related emotions; feelings of burdensomeness, helplessness, desperation, loneliness, numbness, and isolation; and the sense that one deserves punishment. Finally, items assessing preoccupation with and thoughts about NSSI by proxy behaviors focused on the frequency, duration, and intensity (including difficulties resisting thoughts) of preoccupation with NSSI by proxy behaviors (consistent with items from the CANDI).
Finally, in order to provide a more detailed understanding of the nature and phenomenology of NSSI by proxy, additional items were generated to assess unique features of NSSI by proxy (relative to traditional NSSI), including the proxy’s awareness of the individual’s self-injurious intentions and motives, whether the respondent was able to conceal their injury behind social norms, and (for individuals who endorsed both NSSI by proxy and traditional NSSI) the respondent’s preference for traditional NSSI versus NSSI by proxy and the reasons for any indicated preference. These items were initially developed by the first author based on the aforementioned review of the empirical and clinical literature on NSSI by proxy, and then finalized by the second and third authors based on their clinical experience and theoretical knowledge enhanced by the conceptual review.
Study 1
Method
Participants
Participants were part of a larger study examining self-injurious thoughts and behaviors among sexual minority young adults. As part of the larger study, participants were recruited through Prolific Academic, an online research platform that has been shown to be superior to Amazon’s Mechanical Turk in participant honesty and diversity, as well as overall data quality (Peer et al., 2017). The sample was restricted to young adults aged 18 to 35 who were U.S. residents and proficient in English. Further, as part of the larger study, potential participants were screened based on their sexual identity and sexual attraction and selected to fall into one of three groups: (1) sexual majority identity-attraction concordance (i.e., individuals who identify as heterosexual and endorse only other gender sexual attraction, n = 157), (2) sexual minority identity-attraction concordance (i.e., individuals who identify as a sexual minority and do not exclusively endorse other gender sexual attraction, n = 146), and (3) sexual identity-attraction discordance (i.e., individuals who identify as heterosexual yet endorse sexual minority attraction or who identify as a sexual minority yet endorse only sexual majority attraction, n = 145).
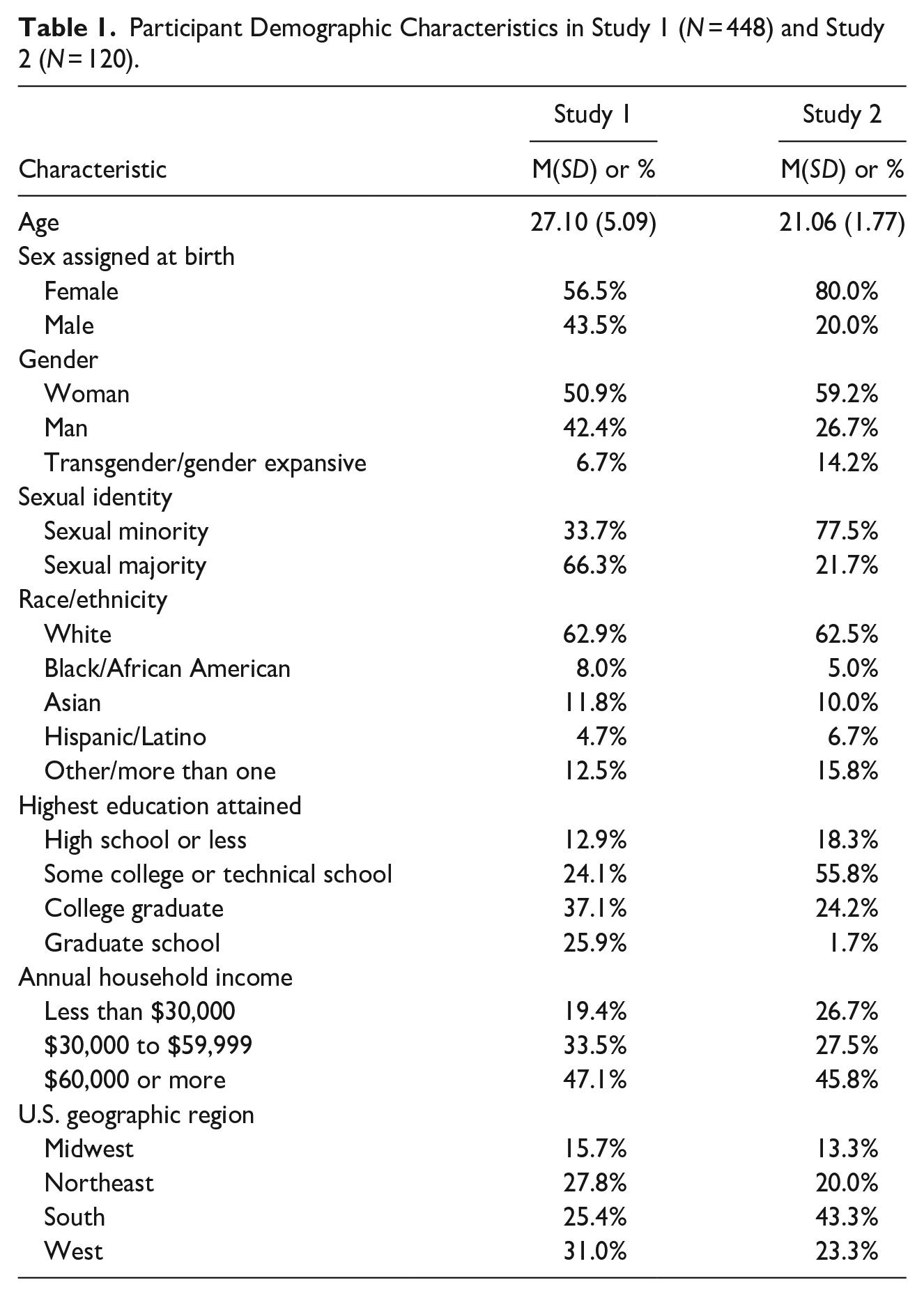
The final sample consisted of 448 participants (M age = 27.10 ± 5.09; 56.5% female sex assigned at birth; 43.5% male sex assigned at birth). With regard to participant gender identity, 50.9% identified as a woman, 42.4% identified as a man, and 6.7% identified as transgender/gender expansive. With regard to racial/ethnic background, just under two-thirds of the participants identified as White (62.9%), followed by Asian (11.8%), more than one race (10.5%), Black/African American (8.0%), and Latinx (4.7%). The majority of participants (63.0%) reported having obtained a college degree or higher, and almost half (47.1%) reported an annual household income of $60,000 or more. Participants represented 43 of 50 U.S. states, with 31.0% from the West, 25.4% from the South, 27.8% from the Northeast, and 15.7% from the Midwest. Detailed data on participant demographic characteristics are reported in Table 1.
Participant Demographic Characteristics in Study 1 (N = 448) and Study 2 (N = 120).
Measures
The Nonsuicidal Self-Injury By Proxy Questionnaire (NSSIBPQ) is a 55-item self-report questionnaire assessing the presence, frequency, and associated characteristics of NSSI by proxy behaviors. The NSSIBPQ asks about lifetime and past year engagement in and frequency of 8 NSSI by proxy behaviors (i.e., initiating injury via tattooing, body piercing, branding or scarification, an animal, sexual activity with a partner, sports, instigating a physical fight, and engaging in elective medical or cosmetic procedures), as well as an “Other” category for participants to include a novel NSSI by proxy behavior. Participants are specifically instructed to endorse the presence of a behavior during the relevant time frame (lifetime or past-year) “. . .only if you did the behavior intentionally, or on purpose, to hurt yourself. Do not respond yes if your intent was not to injure yourself in some way, even if you accidentally got injured (e.g., you accidentally broke your arm while playing a contact sport).” For any behaviors they endorse, follow up questions ask about the frequency of those behaviors, as well as the age of onset (i.e., “How old were you when you first did this for the purpose of injuring yourself?”). Additionally, the NSSIBPQ assesses the motives for and emotional and cognitive antecedents of each behavior (where tattooing, piercing, and scarification/branding are grouped together into one body modification item), the level of preoccupation with and difficulties resisting thoughts about the behaviors, the proxy’s awareness of the individual’s self-injurious intentions and motives, and whether the respondent was able to conceal their injury behind social norms. Finally, the NSSIBPQ asks whether the participant has engaged in traditional NSSI and, if so, their preference for traditional NSSI versus NSSI by proxy and the reasons for any indicated preference.
The Deliberate Self-Harm Inventory (Gratz, 2001) is a 17-item self-report measure that assesses the lifetime history of various aspects of NSSI, including NSSI frequency, duration, age of onset, and method (e.g., cutting, burning). For the purpose of the present study (to ensure that all relevant traditional NSSI behaviors were assessed), the DSHI was modified to assess the additional NSSI behavior of wall/object punching (in addition to the 16 methods included in the original DSHI). The DSHI has been found to demonstrate adequate split-half (r = .78) and test-retest (rs ≥ 0.91) reliability (Fliege et al., 2006; Gratz, 2001), convergent validity with other measures of NSSI (k = 0.63, ICC = 0.79, rs ranging from 0.35 to 0.96; Fliege et al., 2006; Gratz, 2001; Qu et al., 2022; Vigfusdottir et al., 2022), and concurrent validity with respect to relevant clinical constructs theoretically and empirically linked to NSSI, including borderline personality pathology (rs ranging from .37 to .45; Assavedo & Anestis, 2016; Cerutti et al., 2011; Somma et al., 2017) and emotion regulation difficulties (rs = .33–.57; Bjureberg et al., 2016; Kaufman et al., 2016; Somma et al., 2017). Consistent with past research (Dixon-Gordon et al., 2014; Gratz & Tull, 2012; Turner et al., 2013), a dichotomous lifetime NSSI status variable was created by assigning a “1” to participants who reported a lifetime history of NSSI and a “0” to participants who denied any history of NSSI, and a lifetime NSSI frequency variable was computed by summing the total number of NSSI acts reported. The DSHI was used to assess the convergent validity of the NSSIBPQ.
The self-report version of the Self-Injurious Thoughts and Behaviors Interview—Revised (SITBI-R; Fox et al., 2020) was used to assess suicidal ideation (both past year frequency and average intensity), suicide planning (both lifetime frequency and average intensity), and lifetime suicide attempt status. Specifically, participants were asked: (1) “In the past year, how often did you have thoughts of killing yourself?” (rated on a 5-point Likert-type scale ranging from 0 “Never” to 4 “At least once a week”); (2) “On average, how intense were your thoughts of killing yourself?” (rated on a 5-point Likert-type scale ranging from 0 “Mild” to 4 “Severe”); (3) “How many separate times in your life have you made a suicide plan?”; (4) “On average, how seriously did you consider acting on the plan?” (rated on a 5-point Likert-type scale ranging from 0 “Not Seriously” to 4 “Very Seriously”), and (5) “Have you ever made an actual attempt to kill yourself in which you had at least some intent to die?.” The SITBI-R was adapted from the original SITBI (Nock et al., 2007) and has been found to demonstrate adequate test-retest reliability (average k = 0.78; Fox et al., 2020) and convergent validity with other measures of suicidal ideation, suicide planning, and suicide attempts (ks ≥ 0.54; Fox et al., 2020). In addition, the self-report version of the SITBI-R has been found to demonstrate strong alternate forms reliability with the interview version, including for items focused on past-year frequency of suicidal ideation (ICC = 0.78, 95% CI [0.68, 0.85], lifetime frequency of suicide planning (ICC = 0.64, 95% CI [0.50, 0.74], and lifetime suicide attempt status (ICC = 0.72, 95% CI [ 0.61, 0.81]; Fox et al., 2020). The SITBI-R was included to assess the discriminant and concurrent validity of the NSSIBPQ, with the former assessed by examining the association between lifetime NSSI by proxy frequency and lifetime suicide attempt status and the latter assessed by examining the associations of lifetime NSSI by proxy frequency with suicidal ideation and planning.
The Drug Use Questionnaire (DUQ; Hien & First, 1991) was used to assess past-year frequency of overall substance use. The DUQ requires participants to rate the frequency with which they used 12 specific substances (e.g., cannabis, alcohol, cocaine, ecstasy, stimulants, sedatives, heroin, hallucinogens, PCP, inhalants, prescription drugs not as prescribed, and crystal meth) over the course of the past year on a 6-point Likert-type scale. A total score representing past-year frequency of overall substance use was calculated (α = .77 in this sample). The DUQ demonstrates adequate test-retest reliability (r = .77; Tull et al., 2015), acceptable concurrent validity with respect to clinical constructs theoretically and empirically linked to substance use, such as risky behaviors (r = .44; Weiss et al., 2018) and criminal justice system involvement (r = .32; Moore et al., 2017), and acceptable convergent validity with substance use disorder diagnoses obtained from structured interviews (Lejuez et al., 2007). The DUQ was used to assess the discriminant validity of the NSSIBPQ.
The McLean Screening Instrument for Borderline Personality Disorder (MSI-BPD; Zanarini et al., 2003) was used to assess borderline personality disorder (BPD) symptoms. The MSI-BPD is a 10-item self-report measure of the presence versus absence of DSM BPD criteria. Participants are asked to indicate if each item (e.g., “Have you been extremely moody?”; “Have any of your closest relationships been troubled by a lot of arguments or repeated breakups?”) applies to them by responding yes (scored as 1) or no (scored as 0). Items are summed to create a continuous BPD symptom variable reflecting the overall number of endorsed BPD symptoms (α = .85 in this sample). The MSI-BPD has been widely used in both community (Patel et al., 2011) and clinical (Noblin et al., 2014) samples. The MSI-BPD demonstrates adequate test-retest reliability (ρ = 0.72 [Zanarini et al., 2003]; rs ≥ .63 [Gratz et al., 2022]), strong convergent validity with other well-established interview and self-report measures of BPD features and symptoms (as evidenced by correlations ranging from.62 to .85; DeShong et al., 2015; Gardner & Qualter, 2009; Glenn et al., 2009; van Alebeek et al., 2017), and good concurrent validity with respect to BPD-relevant clinical constructs (e.g., emotion regulation difficulties, interpersonal problems, and depression; rs ≥ .47; Glenn & Klonsky, 2009; Gratz et al., 2022; Keng et al., 2019; Leung & Leung, 2009). The MSI-BPD was used to examine the concurrent validity of the NSSIBPQ.
The 9-item Physicians’ Health Questionnaire (PHQ-9; Kroenke et al., 2001) was used to assess depression symptoms (α = .92 in this sample). Derived from the DSM criteria for major depressive disorder (American Psychiatric Association, 1994; Choi et al., 2014), the PHQ-9 has been found to demonstrate good test-retest reliability (r = .84; Kroenke et al., 2001), acceptable convergent validity with both a clinician-administered diagnostic interview for major depression (AUC = 0.84–0.87; Cannon et al., 2007) and self-report measures of depression (rs ≥ .62; Martin et al., 2006; Sun et al., 2020; Titov et al., 2011), and adequate concurrent validity with respect to measures of social, physical health, and mental health functioning (rs ≥ .37; Kroenke et al., 2001; Martin et al., 2006). The PHQ-9 was used to examine the concurrent validity of the NSSIBPQ.
The Difficulties in Emotion Regulation Scale (DERS; Gratz & Roemer, 2004) was used to assess individuals’ typical levels of emotion regulation difficulties across six domains: emotional nonacceptance, difficulties engaging in goal-directed behaviors when distressed, difficulties controlling impulsive behavior when distressed, limited access to effective emotion regulation strategies, lack of emotional awareness, and lack of emotional clarity. Participants rate each item on a 5-point Likert-type scale ranging from 1 (almost never) to 5 (almost always). Responses to items are summed, with higher scores indicating greater emotion regulation difficulties (α = .96 in this sample). The DERS demonstrates acceptable test-retest reliability (ρ = 0.88; Gratz & Roemer, 2004), good convergent validity with other self-report (rs ≥ .60; Cole et al., 2023; Gratz & Roemer, 2004) and behavioral (r = −.63; Gratz et al., 2006) measures of emotion regulation difficulties, and strong concurrent validity with respect to measures of clinical difficulties theorized to be driven by emotion regulation difficulties (e.g., BPD symptoms, eating disorder symptoms, and depression and anxiety symptoms; rs ≥ .46; Burton et al., 2022; Cooper et al., 2014; Salsman & Linehan, 2012; Somma et al., 2017). The DERS was used to assess the concurrent validity of the NSSIBPQ.
Finally, a demographic form collected information on age, sex assigned at birth, gender identity, racial/ethnic background, sexual identity, annual household income, educational attainment, and state of residence.
Procedure
Prior to the start of data collection, all procedures and study materials were approved by the university’s institutional review board. Members of the community were recruited via Prolific Academic. After completing a screener, all participants completed a series of self-report questionnaires. To ensure data quality, validity and attention check items embedded within the survey were reviewed, with the plan to exclude participants who failed two or more validity/attention checks throughout the study; no participants met this criterion and, thus, none were excluded for this. Although all participants were screened internally by Prolific for age (18–35 years old), three participants reported an age over 35 years within the survey and, thus, were excluded (resulting in the final sample of 448 participants).
Data Analysis Plan
Descriptive statistics were calculated to provide descriptive data on NSSI by proxy and its associated characteristics within this sample. Next, a series of chi-square analyses and analyses of variance were conducted to examine differences in rates of lifetime NSSI by proxy behaviors as a function of relevant demographic characteristics. Internal consistency of the NSSIBPQ was examined in several ways. First, internal consistency of the items assessing the motives for, antecedents of, and preoccupation with and thoughts about NSSI by proxy behaviors was examined by calculating Cronbach’s alphas for relevant subsets of items (for reference, αs ≥ .70 are considered acceptable, αs between .60 and .69 are considered questionable, and αs < .60 are considered poor or unacceptable; see George & Mallery, 2003). Next, internal consistency of the items assessing the presence of the eight NSSI by proxy behaviors included in the NSSIBPQ was examined by calculating both split-half reliability and the average inter-item correlation (as Cronbach’s alpha is considered less applicable to a behavioral checklist than items assessing a unitary latent construct; see Streiner, 2003). For reference, inter-item correlations between .15 and .50 are considered acceptable (Clark & Watson, 1995). Split-half reliability coefficients ≥.30 are considered medium in magnitude and those ≥.50 are considered large in magnitude (Cohen, 1988).
To examine the convergent and discriminant validity of the NSSIBPQ, correlation analyses examining the associations of lifetime frequency of NSSI by proxy with lifetime frequency of traditional NSSI, lifetime suicide attempt status, and past-year substance use frequency were conducted, followed by Fisher’s z transformations to examine differences in the strength of the correlations of NSSI by proxy with traditional NSSI versus the other two health risk behaviors (Lee & Preacher, 2013; Steiger, 1980). Support for the convergent and discriminant validity of the NSSIBPQ would be provided by findings of a significant positive association between lifetime frequency of NSSI by proxy on the NSSIBPQ and lifetime frequency of traditional NSSI, as well as findings that this correlation was significantly higher than the correlations between NSSI by proxy and the two other health risk behaviors. To examine the concurrent validity of the NSSIBPQ, correlation analyses examining the associations of both lifetime frequency of NSSI by proxy and lifetime frequency of traditional NSSI with relevant clinical constructs theoretically and empirically linked to NSSI (including suicidal ideation and planning, BPD and depression symptoms, and emotion regulation difficulties; see Chapman et al., 2006; Liu, 2023; Nock et al., 2006) were conducted, followed by a series of Fisher’s z transformations to examine differences in the strength of the correlations of NSSI by proxy versus traditional NSSI with these clinical constructs. Support for the concurrent validity of the NSSIBPQ would be provided by findings of significant positive associations between lifetime frequency of NSSI by proxy on the NSSIBPQ and these clinical constructs of interest (for reference, a correlation of .10 is considered small, a correlation of .30 is considered medium, and a correlation of .50 is considered large; see Cohen, 1988) and/or findings that the correlations between NSSI by proxy and these clinical constructs were comparable in magnitude (i.e., did not differ significantly from) the correlations between lifetime frequency of traditional NSSI and these constructs.
Results
Preliminary Analyses
All continuous variables fell within the acceptable range of normality (Tabachnick & Fidell, 2013), with the exception of past-year substance use frequency and lifetime frequency of NSSI by proxy, traditional NSSI, and suicide planning (skewness ≥3.64). Following Blom transformation, these variables approximated normal distributions (skewness ≤2.05).
Descriptive Data on NSSI by Proxy
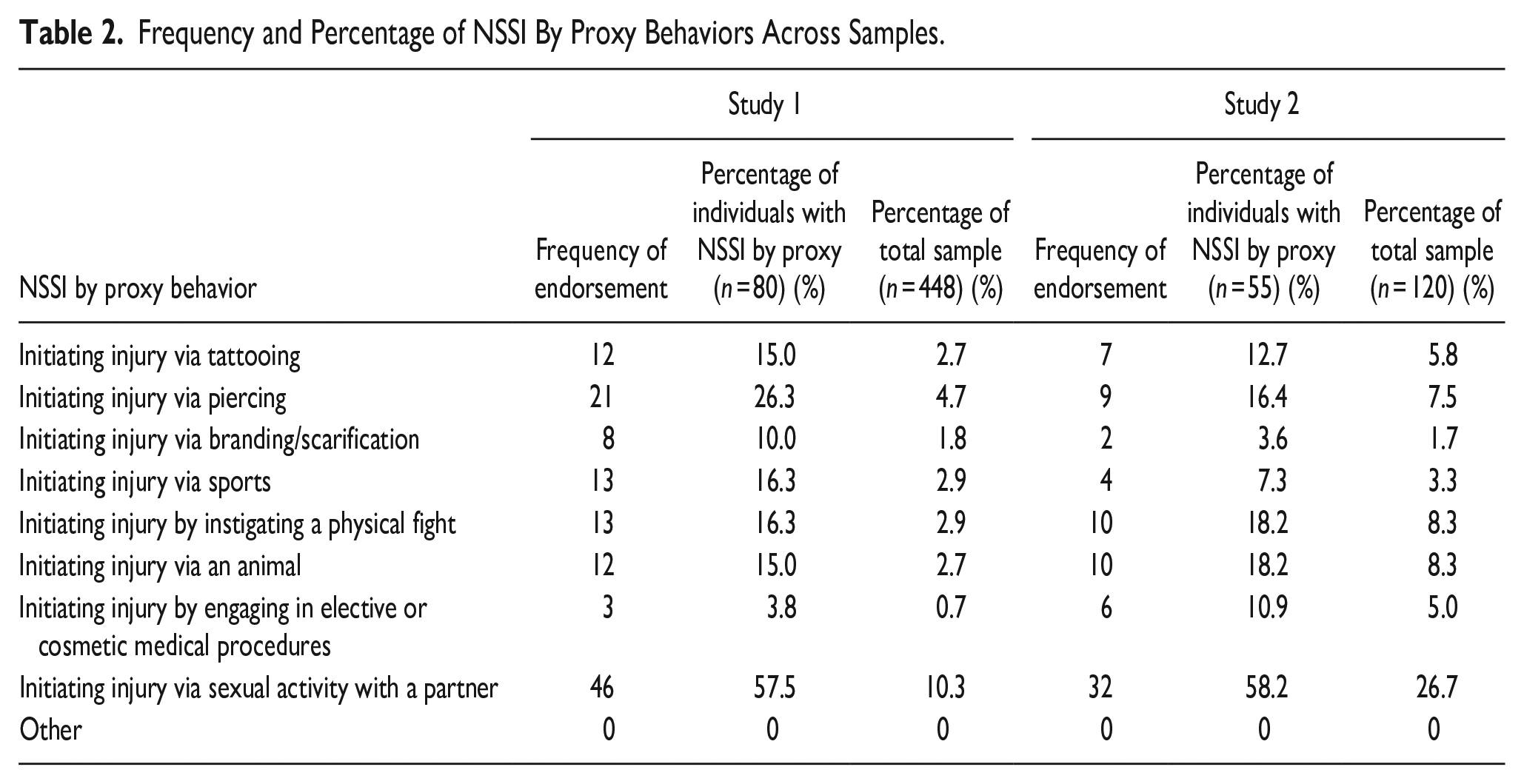
Eighteen percent (n = 80) of the sample reported a history of NSSI by proxy (compared to 57.4% [n = 257] who reported a history of traditional NSSI). Of these 80 participants, 83% (n = 66) reported more than one act of NSSI by proxy, 59.5% (n = 47) reported at least 5 acts, 40.5% (n = 32) reported at least 10 acts, and 11.4% (n = 9) reported at least 100 acts. Participants with NSSI by proxy reported an average of 41.33 (SD = 130.50) lifetime NSSI by proxy acts and an average of 1.60 (SD = 1.01) different NSSI by proxy behaviors. The past-year rate of NSSI by proxy was 8% (n = 36), of whom 70.6% (n = 24) reported more than one past-year act and 44% (n = 15) reported ≥5 past-year acts. With regard to individual NSSI by proxy behaviors, the most frequently reported were initiating injury via sexual activity with a partner (10.3%; n = 46) and body piercing (4.7%; n = 21). Detailed information on the rates of endorsement of all assessed NSSI by proxy behaviors is presented in Table 2.
Frequency and Percentage of NSSI By Proxy Behaviors Across Samples.
There was considerable overlap between traditional NSSI and NSSI by proxy. Of those reporting a history of NSSI by proxy, 87.5% (n = 70) also endorsed lifetime traditional NSSI, whereas 27.2% (n = 70) of those with a history of traditional NSSI also reported a history of NSSI by proxy. However, it is important to note that 12.5% (n = 10) of participants with a history of NSSI by proxy denied any history of traditional NSSI. Notably, the average age of onset for NSSI by proxy was 18.63 (SD = 4.54), whereas the average age of onset for traditional NSSI was 12.62 (SD = 4.45). Comparison of the average age of onset for these behaviors revealed significant differences, with traditional NSSI beginning at a significantly younger age than NSSI by proxy, t (331) = 10.34, p < .001, SE = 0.58.
Associated Characteristics of NSSI by Proxy
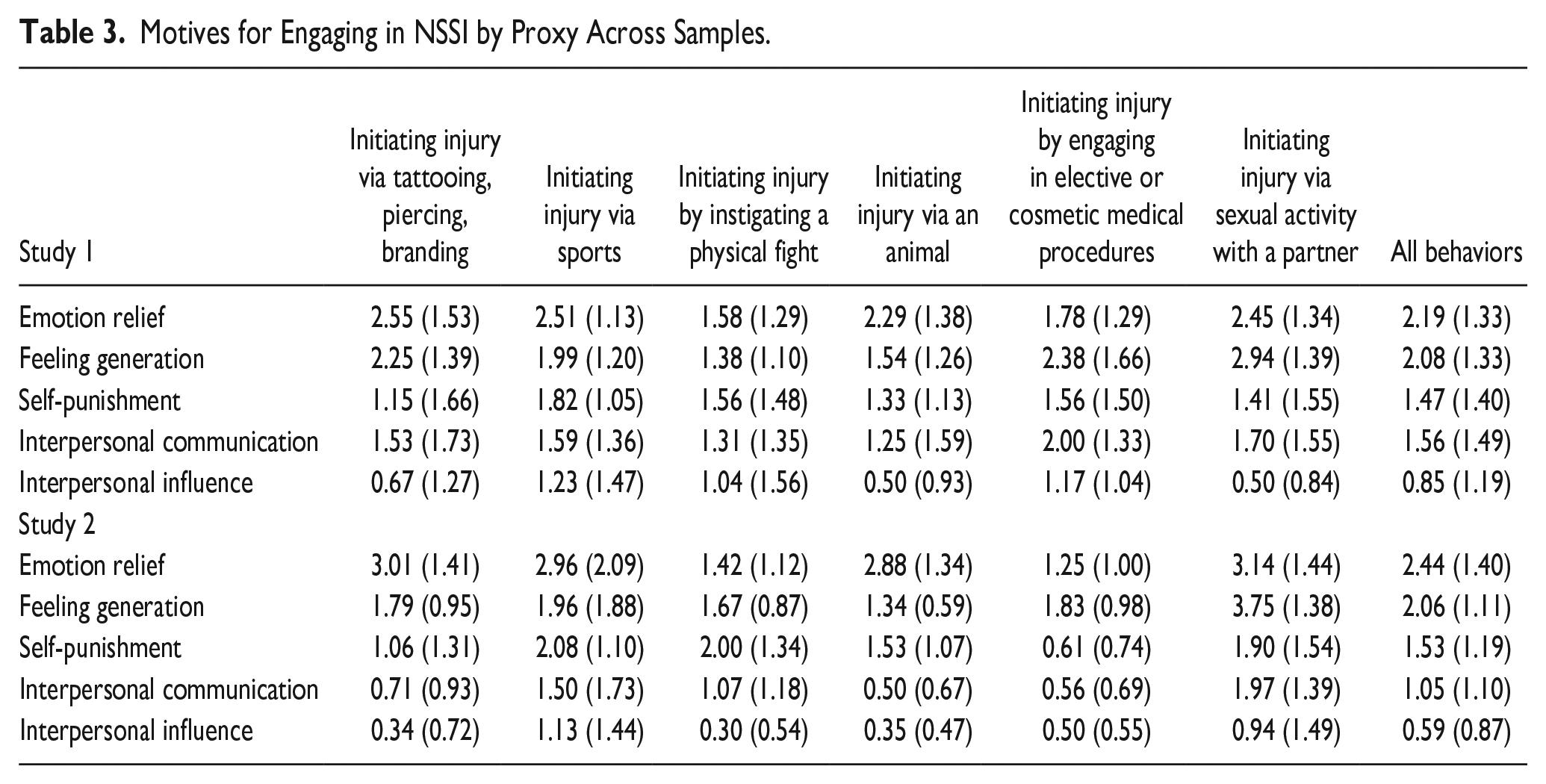
Consistent with research emphasizing the importance of emotion regulation motives to NSSI (Turner et al., 2012; Zetterqvist et al., 2013), the most commonly reported motives for NSSI by proxy were emotion relief (endorsed by 96.3% of participants; n = 77) and feeling generation (endorsed by 95% of participants; n = 76), followed by interpersonal communication (endorsed by 72.5%; n = 58), self-punishment (endorsed by 71.3%; n = 57), and interpersonal influence (endorsed by 32.5%; n = 26). Data on the mean level of endorsement of each of these motives across each NSSI by proxy behavior are presented in Table 3.
Motives for Engaging in NSSI by Proxy Across Samples.
Almost all participants (98.2%; n = 79) reported negative thoughts and/or feelings prior to engaging in NSSI by proxy behavior. Additionally, 75% (n = 60) of participants endorsed preoccupation with NSSI by proxy prior to engaging in the behavior, and 47.5% (n = 38) reported having thoughts about NSSI by proxy that were at least moderate in intensity and somewhat difficult to resist. Finally, with regard to the frequency and duration of thoughts about NSSI by proxy, 68.8% (n = 55) of participants reported thoughts about this behavior at least monthly and 75% (n = 60) reported that these thoughts lasted longer than a minute (with 20% [n = 16] reporting that these thoughts lasted 4 or more hours).
Of those with NSSI by proxy, 76.3% (n = 61) reported that the person injuring them was not aware of their self-injurious intentions. Of the 23.7% (n = 19) of participants whose proxy was aware of their self-injurious intentions, 31.6% (n = 6) reported that their proxy was not aware of their motives for self-injury.
With regard to the degree to which participants believed they were able to conceal the self-injurious intentions of their NSSI by proxy behavior behind social norms, 92.5% (n = 74) endorsed being able to conceal their intentions to a moderate degree and 35.0% (n = 28) of participants reported that they were fully able to conceal the self-injurious intentions of their behavior; only one participant (1.3%) denied any ability to conceal their self-injurious intentions.
Of the 61 participants who reported both NSSI and NSSI by proxy behaviors, 59% (n = 36) reported a preference for NSSI, 21.3% (n = 13) reported a preference for NSSI by proxy, and 19.7% (n = 12) reported no preference for either behavior. The most commonly endorsed reasons for preferring NSSI by proxy were that the behavior was more practical (61.5%; n = 8), more socially acceptable (53.8%; n = 7), and easier to do (46.2%; n = 6). The most commonly endorsed reasons for preferring traditional NSSI to NSSI by proxy were that traditional NSSI was easier to hide (86.1%; n = 31), more in their control (80.6%; n = 29), easier to do (72.2%; n = 26), and more immediate (72.2%; n = 26).
Demographic Differences in Rates of NSSI by Proxy
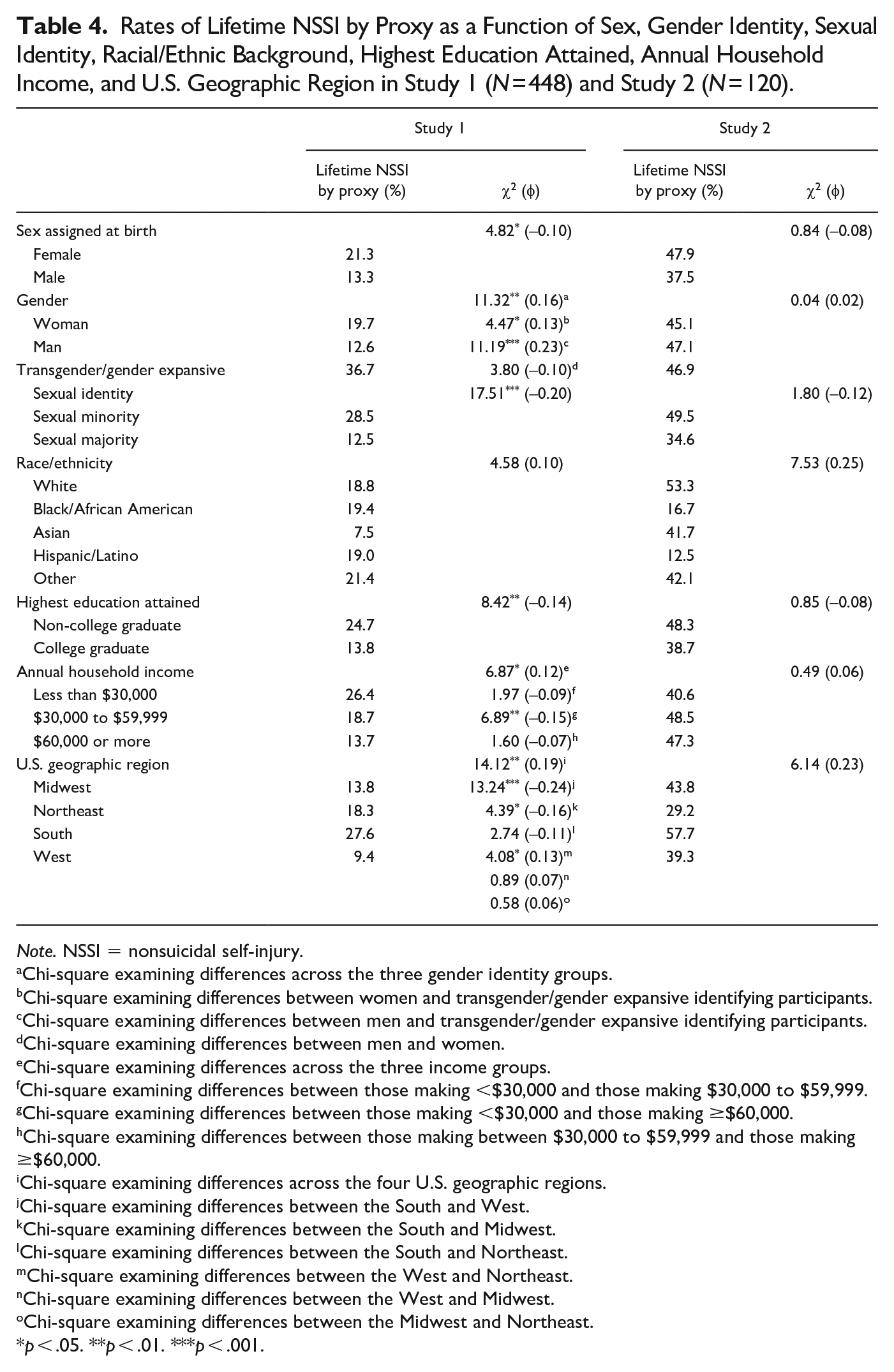
Differences in rates of lifetime NSSI by proxy as a function of relevant demographic characteristics are presented in Table 4. Rates of lifetime NSSI by proxy differed significantly between participants assigned female versus male sex at birth, such that female participants were more likely to report a history of NSSI by proxy than male participants. Rates of lifetime NSSI by proxy also differed significantly as a function of gender identity, such that transgender/gender expansive identifying participants were more likely to report a history of NSSI by proxy than cisgender men or women, whereas cisgender men and women did not differ significantly in rates of lifetime NSSI by proxy. Additionally, rates of lifetime NSSI by proxy differed significantly as a function of sexual identity, with participants identifying as a sexual minority reporting higher rates than those identifying as heterosexual. Rates of lifetime NSSI by proxy also differed significantly as a function of education and income, such that lower rates were reported by individuals with (vs. without) a college degree and those with an annual household income of at least $60,000 (vs. an annual income of less than $30,000). Finally, rates of NSSI by proxy differed significantly as a function of U.S. geographic region, such that participants living in the South were more likely to report a history of NSSI by proxy than those living in the West and Midwest and those living in the Northeast were more likely to report a history of this behavior than those living in the West. Rates of NSSI by proxy did not differ significantly as a function of age (F [17,447] = 0.66, p = .84) or racial/ethnic background (see Table 4). Differences in rates of specific NSSI by proxy behaviors as a function of sex assigned at birth, gender identity, sexual identity, racial/ethnic background, highest education attained, household income, and U.S. geographic region can be found in Supplemental Table 1.
Rates of Lifetime NSSI by Proxy as a Function of Sex, Gender Identity, Sexual Identity, Racial/Ethnic Background, Highest Education Attained, Annual Household Income, and U.S. Geographic Region in Study 1 (N = 448) and Study 2 (N = 120).
Note. NSSI = nonsuicidal self-injury.
Chi-square examining differences across the three gender identity groups.
Chi-square examining differences between women and transgender/gender expansive identifying participants.
Chi-square examining differences between men and transgender/gender expansive identifying participants.
Chi-square examining differences between men and women.
Chi-square examining differences across the three income groups.
Chi-square examining differences between those making <$30,000 and those making $30,000 to $59,999.
Chi-square examining differences between those making <$30,000 and those making ≥$60,000.
Chi-square examining differences between those making between $30,000 to $59,999 and those making ≥$60,000.
Chi-square examining differences across the four U.S. geographic regions.
Chi-square examining differences between the South and West.
Chi-square examining differences between the South and Midwest.
Chi-square examining differences between the South and Northeast.
Chi-square examining differences between the West and Northeast.
Chi-square examining differences between the West and Midwest.
Chi-square examining differences between the Midwest and Northeast.
p < .05. **p < .01. ***p < .001.
Internal Consistency
Internal consistency of the items assessing motives for, antecedents of, and preoccupation with and thoughts about NSSI by proxy behaviors were generally acceptable, with Cronbach’s αs ≥.83 for the motives items and ≥.78 for the items assessing preoccupation with and thoughts about these behaviors and antecedents of most of the specific NSSI by proxy behaviors examined in this measure, with two exceptions: the antecedents items for the behaviors of initiating injury via instigating a physical fight (α = .60) and engaging in elective or cosmetic medical procedures (α = .67) were questionable. Likewise, internal consistency of the items assessing the presence of the eight NSSI by proxy behaviors included in the NSSIBPQ was acceptable (split-half correlation: ρ = .68; average inter-item correlation: r = .19).
Validity of the NSSIBPQ
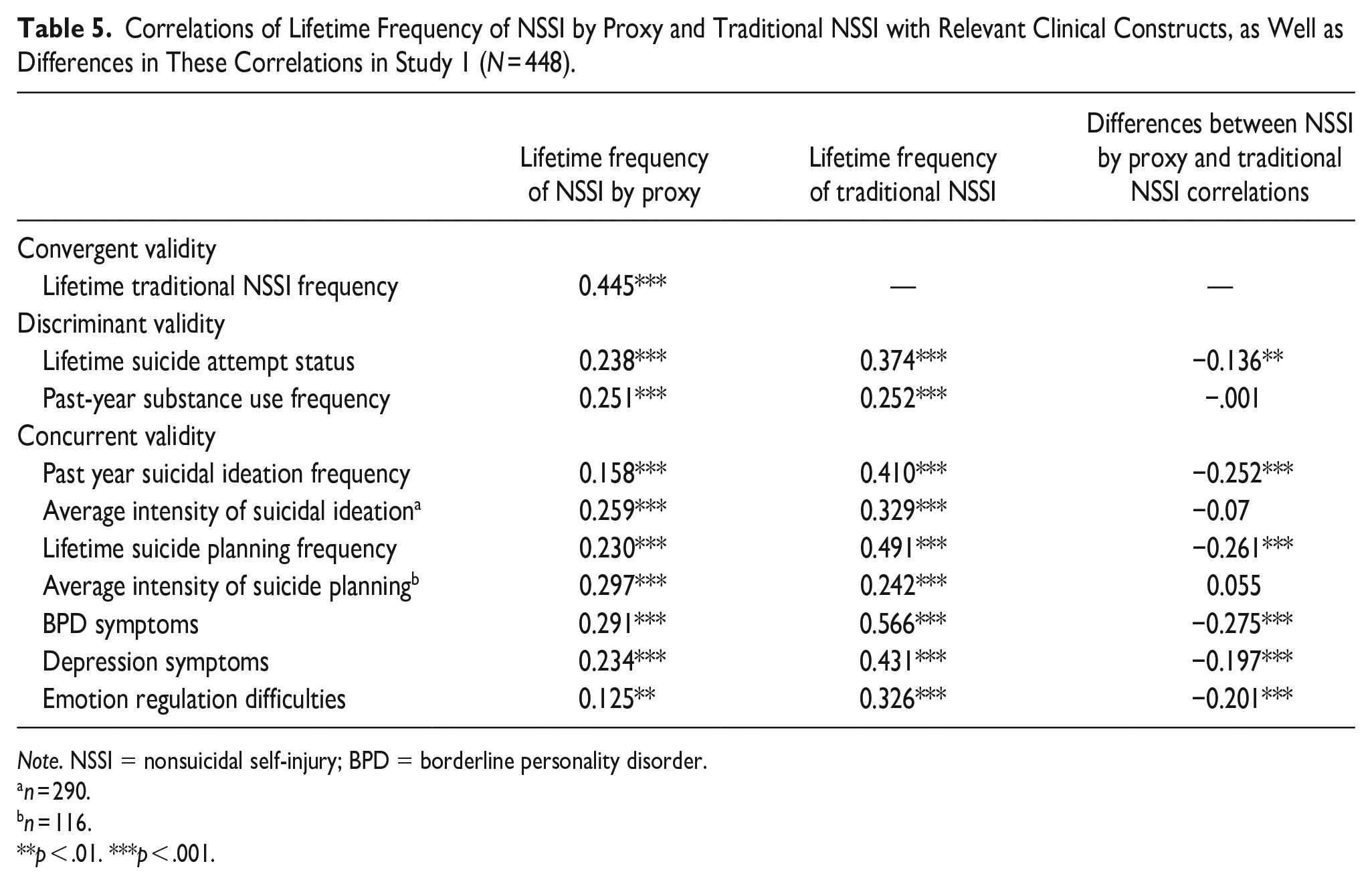
Correlations of lifetime frequency of NSSI by proxy with lifetime frequency of traditional NSSI, lifetime suicide attempt status, past-year substance use frequency, and the clinical constructs of interest (including suicidal ideation and planning, BPD and depression symptoms, and emotion regulation difficulties) are presented in Table 5. For comparison purposes, the correlations of lifetime frequency of traditional NSSI with these constructs are also presented, along with the results of analyses comparing the strength of the associations of lifetime frequency of NSSI by proxy versus traditional NSSI with these other constructs.
Correlations of Lifetime Frequency of NSSI by Proxy and Traditional NSSI with Relevant Clinical Constructs, as Well as Differences in These Correlations in Study 1 (N = 448).
Note. NSSI = nonsuicidal self-injury; BPD = borderline personality disorder.
n = 290.
n = 116.
**p < .01. ***p < .001.
Convergent and Discriminant Validity
Providing support for the convergent and discriminant validity of the NSSIBPQ, lifetime frequency of NSSI by proxy on the NSSIBPQ was significantly positively associated with lifetime frequency of traditional NSSI on the DSHI (r = .45). Moreover, this correlation was significantly higher than the correlations between lifetime frequency of NSSI by proxy and the other health risk behaviors examined in this study: lifetime suicide attempt status (r = .24, z = 4.28, p < .001) and past-year substance use frequency (r = .25, z = 3.69, p < .001).
Concurrent Validity
Providing support for the concurrent validity of the NSSIBPQ, lifetime frequency of NSSI by proxy on this measure was significantly positively associated with past year frequency and average intensity of suicidal ideation, lifetime frequency and average intensity of suicide planning, BPD symptoms, depression symptoms, and emotion regulation difficulties. Further, the correlations between lifetime frequency of NSSI by proxy and average intensity of both suicidal ideation and suicide planning were comparable in magnitude to the correlations between lifetime frequency of traditional NSSI and these constructs. Conversely, the correlations between lifetime frequency of traditional NSSI and the frequency of suicidal ideation and planning, BPD and depression symptoms, and emotion regulation difficulties were significantly higher than the correlations between these constructs and lifetime frequency of NSSI by proxy (see Table 5).
Discussion
This study aimed to extend extant research on NSSI by examining the presence, frequency, and associated characteristics of NSSI by proxy within a large nationwide community sample of young adults and providing preliminary data on the internal consistency and convergent, discriminant, and concurrent validity of a new measure of NSSI by proxy: the NSSIBPQ. Findings support the clinical relevance of NSSI by proxy within this population, revealing a comparable rate of this behavior within this sample (18%) to rates of traditional NSSI among other young adult samples (see Kiekens et al., 2023; S. V. Swannell et al., 2014). Likewise, providing support for the conceptualization of NSSI by proxy as a distinct form of NSSI, results revealed both considerable overlap of NSSI by proxy with more traditional forms of NSSI and a subset of participants (12.5%) for whom NSSI by proxy was their only form of NSSI. Moreover, examination of the associated characteristics of NSSI by proxy provided support for both the characteristics considered unique to NSSI by proxy (vs. traditional NSSI; i.e., concealment and social acceptability) and those expected to overlap with NSSI (e.g., those pertinent to an NSSID diagnosis). For example, findings revealed that the motives for NSSI by proxy are comparable to those reported for NSSI in past research (Turner et al., 2012; Zetterqvist et al., 2013), and most commonly involved emotion regulation. Likewise, the antecedents of NSSI by proxy were comparable to those reported for traditional NSSI, with 98.2% of participants who engaged in NSSI by proxy reporting negative thoughts and/or feelings prior to engaging in this behavior.
With regard to the reliability and validity of the NSSIBPQ, this measure demonstrated adequate internal consistency across most items. In addition, results provided preliminary support for the convergent and discriminant validity of this measure, revealing a significantly stronger correlation between lifetime frequency of NSSI by proxy on this measure and lifetime frequency of traditional NSSI on the DSHI than the correlations between lifetime frequency of NSSI by proxy and either lifetime suicide attempt status or past-year substance use frequency. Moreover, providing support for the concurrent validity of the NSSIBPQ, lifetime frequency of NSSI by proxy on this measure was significantly positively associated with all the clinical constructs theoretically and empirically linked to NSSI, including suicidal ideation and planning, BPD and depression symptoms, and emotion regulation difficulties.
Despite providing initial evidence in support of the clinical importance of NSSI by proxy and validity of the NSSIBPQ, this study was limited by the use of a single community sample of young adults. In particular, the extent to which these findings would generalize to samples with more severe clinical difficulties remains unclear. Further research examining this behavior and measure within a more clinically relevant sample is needed.
Study 2
Study 2 aimed to extend the findings of Study 1 by examining the presence, frequency, and associated characteristics of NSSI by proxy within a more clinically relevant sample of young adults with current NSSI and suicidality, as well as explore the internal consistency and validity of the NSSIBPQ within this sample. Additionally, Study 2 expanded upon Study 1 by assessing the distress and impairment associated with NSSI by proxy behaviors and comparing this to the levels of distress and impairment associated with traditional NSSI. In so doing, this study has the potential to speak to the rates and characteristics of NSSI by proxy, as well as the validity of the NSSIBPQ, within a more clinically severe sample likely to be at elevated risk for NSSI by proxy and resultant distress and functional impairment.
Methods
Participants
Participants in Study 2 included 120 emerging adults from the community recruited through Prolific Academic for a larger study on NSSI and suicide. To be eligible for the larger study, participants were required to be 18 to 25 years of age and report current suicidal ideation (i.e., endorsement of serious thoughts of killing oneself in the past year), no history of a suicide attempt, at least five lifetime acts of traditional NSSI with at least one act in the past year, U.S. residency, and English proficiency.
Participants ranged in age from 18 to 25 (M age = 21.06 ± 1.77), and most (80%) were assigned female sex at birth (20% assigned male sex at birth). With regard to participants’ gender identity, the majority of participants identified as women (59.2%), followed by transgender/gender expansive (26.7%), and men (14.2%). Moreover, the majority of participants (77.5%) endorsed a sexual minority identity. With regard to racial/ethnic background, most participants identified as White (62.5%), followed by more than one race (12.5%), Asian (10%), Latinx (6.7%), and Black/African American (5.0%). Most participants (81.7%) reported some education beyond high school, and almost half (45.8%) reported an annual household income of $60,000 or more. Participants represented 30 of 50 states in the U.S., with 43.3% from the South, 23.3% from the West, 20.0% from the Northeast, and 13.3% from the Midwest. Detailed data on participant demographic characteristics are reported in Table 1.
Measures
The Nonsuicidal Self-injury By Proxy Questionnaire (NSSIBPQ) was once again used to assess the presence, frequency, and associated characteristics of NSSI by proxy.
The Deliberate Self-Harm Inventory (DSHI; Gratz, 2001) was again used to assess the presence, frequency, and age of onset of traditional NSSI behaviors. As in Study 1, the DSHI was modified to include wall/object punching, and the variables of lifetime NSSI status, lifetime NSSI frequency, and age of onset were calculated in the same way as in Study 1. The DSHI was used to assess the convergent validity of the NSSIBPQ in this sample.
The Drug Use Questionnaire (DUQ; Hien & First, 1991) was used again to assess past year substance use frequency (α = .64 in this sample). As in Study 1, this measure was included to examine the discriminant validity of the NSSIBPQ.
The Body-focused Self-damaging Behavior Expectancies Questionnaire (BSBEQ; Forbes et al., 2022) was used to assess the yearly frequency of self-damaging behaviors other than NSSI, including disordered eating behaviors (i.e., food restriction, purging, and binging), hair-pulling, and problematic exercise. For the purpose of this study, the yearly frequency of each of these behaviors was summed to create an overall index of the yearly frequency of self-damaging behaviors in general. The BSBEQ demonstrates adequate test-retest reliability (rs ranging from .61 to .89; Forbes et al., 2022) and convergent validity in a community sample (as evidenced by significant associations with measures of self-damaging behaviors; rs ranging from .31 to .43; Forbes et al., 2022). This measure was included to examine the discriminant validity of the NSSIBPQ in the present sample.
The self-report version of the Self-Injurious Thoughts and Behaviors Interview—Revised (SITBI-R; Fox et al., 2020) was again used to assess suicidal outcomes. However, given the restricted range in both suicidal ideation and suicide attempts within this sample due to study inclusion criteria (with all participants required to endorse serious past-year suicidal ideation and no history of suicide attempts), only the suicide planning variables (both lifetime frequency and average intensity) were examined in this study. These variables were operationalized in the same way as in Study 1. The SITBI-R was used to examine the concurrent validity of the NSSIBPQ in this sample.
The Personality Assessment Inventory-Borderline Features Scale (PAI-BOR; Morey, 1991) was used in this study to assess BPD features, in order to examine the concurrent validity of the NSSIBPQ. This 24-item self-report questionnaire assesses four domains of BPD features (affective instability, identity problems, negative relationships, and self-harm) and yields both overall and subscale scores. The overall score was used in this study (α = .88 in this sample). The PAI-BOR demonstrates good test-retest reliability (r = .77; Trull, 1995), strong convergent validity with both other self-report measures of BPD pathology (rs ≥ .85; Gardner & Qualter, 2009) and diagnostic interviews of BPD (r = .58; Jacobo et al., 2007), and good concurrent validity with respect to associations with BPD-relevant clinical difficulties (including substance use problems, eating disorders, depression, and emotion regulation difficulties (rs ≥ .41; Gardner & Qualter, 2009; Iverson et al., 2012).
The depression subscale of the Depression Anxiety Stress Scales-21 (DASS-21; Lovibond & Lovibond, 1995) was used to assess depression symptom severity. The DASS-21 is a 21-item self-report measure used to differentiate between core symptoms of depression, anxiety, and stress. Participants are asked to rate items on a 4-point Likert-type scale. The DASS-21 depression subscale demonstrates adequate test-retest reliability (r = .69; Gomez et al., 2014) and strong convergent validity with other self-report measures of depression (rs ≥ .71; Antony et al., 1998; Peters et al., 2021) and negative (r = .59; Henry & Crawford, 2005) and positive (r = −.48; Henry & Crawford, 2005) affect. The depression subscale (α = .90 in this sample) was used to examine the NSSIBPQ’s concurrent validity.
The Difficulties in Emotion Regulation Scale (DERS; Gratz & Roemer, 2004) was again used to assess emotion regulation difficulties (α = .92 in this sample), in order to examine the concurrent validity of the NSSIBPQ.
A modified version of the Sheehan Disability Scale (SDS; Sheehan, 1983) was used to examine functional impairment and subjective distress due to NSSI by proxy and traditional NSSI behaviors. The SDS is a 3-item self-report measure designed to assess overall functional impairment across the domains of work/school, social life, and home life/family responsibilities using an 11-point Likert-type scale ranging from 0 (“Not at all”) to 10 (“Extremely”). The SDS has demonstrated adequate test-retest reliability (ICC = 0.72, 95% CI [0.67, 0.77]; Coles et al., 2014) and good convergent and concurrent validity with other disability scales (rs ≥ .56; Hambrick et al., 2004) and measures of depression (rs ≥ .56; Diefenbach et al., 2007; Hambrick et al., 2004), social anxiety (r = .50; Hambrick et al., 2004), obsessive-compulsive disorder symptoms (r = .75; Diefenbach et al., 2007), attention deficit hyperactivity disorder symptoms (rs ≥ .71; Coles et al., 2014), and quality of life (r = −.47; Hambrick et al., 2004).
For the purpose of this study, the SDS was modified to assess both impairment and distress associated with engagement in traditional NSSI behaviors and NSSI by proxy behaviors. As such, participants filled out the modified SDS twice, once to assess for the level of distress and impairment due to traditional NSSI and a second time to assess the level of distress and impairment due to NSSI by proxy. To assess distress associated with these behaviors, the following questions were included: “How much distress have you experienced due to NSSI (e.g., cutting, burning, etc.)?”; and “How much distress have you experienced due to self-injury involving the actions of others?” Participants responded to these questions using a 5-point Likert scale ranging from 1 (“None”) to 5 (“Extreme, incapacitating distress”). All original SDS impairment items were also included; however, each of these items was modified to assess the level of impairment experienced in each domain as a result of NSSI or NSSI by proxy (e.g., “NSSI has disrupted your work/school work.”). Scores on the three impairment items pertaining to NSSI by proxy were averaged to create an overall index of impairment due to NSSI by proxy (α = .89 in this sample), and scores on the three impairment items pertaining to NSSI were averaged to create an overall index of impairment due to NSSI (α = .86 in this sample).
Finally, a demographic form collected information on age, sex assigned at birth, gender identity, racial/ethnic background, sexual identity, annual household income, educational attainment, and state of residence.
Procedure
All procedures and study materials were approved by the university’s institutional review board. Data for this study were collected as part of a larger prospective study examining the association between NSSI and suicide risk. Data for the current study were drawn from the baseline assessment. Participants were recruited via Prolific Academic. Participants were internally screened so that only adults aged 18 to 25 who resided in the U.S. and were proficient in the English language were able to access the study. Then, to determine eligibility for the larger study from which these data were drawn, participants were screened for current suicidality (i.e., “In the past year, have you ever had serious thoughts of killing yourself?”), lifetime and past-year frequency of NSSI, and lifetime history of suicide attempts. Participants who endorsed serious thoughts of killing themselves in the past year, ≥5 lifetime acts of NSSI (with at least one act in the past year), and no history of a suicide attempt were invited to complete a series of self-report questionnaires. To ensure data quality, validity and attention check items embedded within the survey were reviewed and participants (n = 1) who failed two or more validity/attention checks throughout the study were excluded (resulting in the final sample of 120 participants).
Data Analysis Plan
Descriptive statistics were calculated to provide descriptive data on NSSI by proxy and its associated characteristics within this sample. Next, a series of chi-square analyses and analyses of variance were conducted to examine differences in rates of lifetime NSSI by proxy behaviors as a function of relevant demographic characteristics. Internal consistency of the NSSIBPQ items assessing the motives for, antecedents of, and preoccupation with and thoughts about NSSI by proxy behaviors was once again examined by calculating Cronbach’s alphas for relevant subsets of items, whereas internal consistency of the items assessing the presence of the specific NSSI by proxy behaviors included in the NSSIBPQ was examined by calculating both split-half reliability and average inter-item correlations.
To examine the convergent and discriminant validity of the NSSIBPQ within this sample, correlation analyses examining the associations of lifetime frequency of NSSI by proxy with lifetime frequency of traditional NSSI, past-year substance use frequency, and yearly frequency of self-destructive behaviors other than NSSI were conducted, followed by Fisher’s z transformations to examine differences in the strength of the correlations of NSSI by proxy with traditional NSSI versus the other two health risk behavior outcomes. Support for the convergent and discriminant validity of the NSSIBPQ would be provided by findings of a significant positive association between lifetime frequency of NSSI by proxy on the NSSIBPQ and lifetime frequency of traditional NSSI, as well as findings that this correlation was significantly higher than the correlations between NSSI by proxy and the two other health risk behavior outcome variables. To examine the concurrent validity of the NSSIBPQ, correlation analyses examining the associations of both lifetime frequency of NSSI by proxy and lifetime frequency of traditional NSSI with relevant clinical constructs theoretically and empirically linked to NSSI (including suicide planning, BPD features, depression symptoms, and emotion regulation difficulties) were conducted, followed by a series of Fisher’s z transformations to examine differences in the strength of the correlations of NSSI by proxy versus traditional NSSI with these clinical constructs. Support for the concurrent validity of the NSSIBPQ would be provided by findings of significant positive associations between lifetime frequency of NSSI by proxy on the NSSIBPQ and these NSSI-relevant clinical constructs and/or findings that the correlations between NSSI by proxy and these clinical constructs were comparable in magnitude (i.e., did not differ significantly from) the correlations between lifetime frequency of traditional NSSI and these constructs.
Results
Preliminary Analyses
All continuous variables fell within the acceptable range of normality (Tabachnick & Fidell, 2013), with the exception of lifetime frequency of NSSI by proxy and suicide planning (skewness >5.02). Following Blom transformation, these variables approximated normal distributions (skewness ≤1.06).
Descriptive Data on NSSI by Proxy
Among this sample of participants with a history of NSSI, 45.8% (n = 55) reported a lifetime history of NSSI by proxy. Of these participants, 87.3% (n = 48) reported more than 1 act of NSSI by proxy, 50.9% (n = 28) reported at least 5 acts, and 27.3% (n = 15) reported at least 10 acts. Participants with NSSI by proxy reported an average of 10.33 (SD = 16.96) lifetime NSSI by proxy acts and an average of 1.45 (SD = 0.63) different NSSI by proxy behaviors. The past year rate of NSSI by proxy was 24% (n = 29), of whom 79.3% (n = 23) reported more than 1 past-year act, 31.0% (n = 9) reported at least 5 past-year acts, and 17.2% (n = 5) reported more than 10 past-year acts. The most frequently reported NSSI by proxy behaviors were initiating injury via sexual activity with a partner (26.7%; n = 32), via an animal (8.3%; n = 10), and by instigating a physical fight (8.3%; n = 10). Detailed information on the rates of endorsement of all assessed NSSI by proxy behaviors is presented in Table 2.
Consistent with the findings of Study 1, results revealed a significant difference in the average age of onset of NSSI by proxy versus traditional NSSI, t (173) = 8.57, p < .001, with traditional NSSI beginning at a significantly younger age (mean = 12.57; SD = 3.51) than NSSI by proxy (mean = 17.22; SD = 2.90).
Associated Characteristics of NSSI by Proxy
Consistent with the results of Study 1, the most commonly reported motives for NSSI by proxy were emotion relief and feeling generation (each endorsed by 96.4% of participants; n = 53), followed by self-punishment (endorsed by 87.3%; n = 48), interpersonal communication (endorsed by 69.1%; n = 38), and interpersonal influence (endorsed by 41.8%; n = 23). Data on the mean level of endorsement of each of these motives across each NSSI by proxy behavior are presented in Table 3.
All participants (100%; n = 55) endorsed the presence of negative thoughts or feelings prior to engaging in NSSI by proxy. Further, 98.2% (n = 54) of participants endorsed preoccupation with NSSI by proxy prior to engaging in the behavior, and 70.9% (n = 39) reported having thoughts about NSSI by proxy that were at least moderate in intensity and somewhat difficult to resist. With regard to the frequency and duration of thoughts about NSSI by proxy, 74.5% (n = 41) of participants reported thoughts about this behavior at least monthly and 92.7% (n = 51) reported that these thoughts lasted longer than a minute (with 14.5% [n = 8] reporting that these thoughts lasted four or more hours).
Of those with NSSI by proxy, 92.7% (n = 51) reported that the person injuring them was not aware of their self-injurious intentions. However, of the 7.3% (n = 4) of participants whose proxy was aware of their self-injurious intentions, all (100%; n = 4) reported that their proxy was also aware of their motives for self-injury.
With regard to the degree to which participants believed they were able to conceal the self-injurious intentions of their NSSI by proxy behind social norms, 90.9% (n = 50) endorsed being able to conceal their intentions to a moderate degree and 45.5% (n = 25) of participants reported that they were fully able to conceal the self-injurious intentions of their behavior; only one participant (1.8%) denied any ability to conceal their self-injurious intentions.
Of the 55 participants who reported both NSSI and NSSI by proxy behaviors, 87.3% (n = 48) reported a preference for NSSI, 7.3% (n = 4) reported a preference for NSSI by proxy, and 5.5% (n = 3) reported no preference for either behavior. The most commonly endorsed reasons for preferring NSSI by proxy were that it is easier to do (100%; n = 4), easier to hide (100%; n = 4), more socially acceptable (100%; n = 4), and results in less guilt and shame afterward (75%; n = 3). For individuals who preferred traditional NSSI, the most commonly endorsed reasons were that it is more in their control (93.8%; n = 45), easier to do (81.3%; n = 39), more immediate (81.3%; n = 39), and takes less planning (77.0%; n = 37).
On average, participants reported mild to moderate distress from both traditional NSSI (mean = 2.78, SD = 0.79) and NSSI by proxy (mean = 2.42, SD = 0.79), although the level of distress associated with traditional NSSI was significantly higher than that associated with NSSI by proxy, t (173) = 2.80, p = .006. Further, 45.5% (n = 25) of participants reported moderate to severe distress associated with NSSI by proxy (relative to 69.1% [n = 83] of participants who reported moderate to severe distress associated with NSSI). Likewise, although the level of reported functional impairment due to both NSSI by proxy (mean = 2.22, SD = 2.29) and traditional NSSI (mean = 3.19, SD = 2.36) was relatively low (corresponding to an average score of just over mild impairment on the 0–10 scale), the mean level of impairment due to traditional NSSI was significantly higher than that reported for NSSI by proxy, t (173) = 2.55, p = .01. Moreover, 14.5% (n = 8) of participants endorsed at least moderate impairment due to NSSI by proxy (compared to 23.3% [n = 28] of participants who endorsed at least moderate impairment due to traditional NSSI).
Demographic Differences in Rates of NSSI by Proxy
Differences in rates of lifetime NSSI by proxy as a function of relevant demographic characteristics are presented in Table 4. Rates of lifetime NSSI by proxy did not differ significantly as a function of sex assigned at birth, gender identity, sexual identity, racial/ethnic background, highest education attained, annual household income, or U.S. geographic region of residence (ps > .10). Likewise, there were no significant differences in age between participants with versus without a history of NSSI by proxy, F (1,119) = 0.15, p = .70. Differences in rates of specific NSSI by proxy behaviors as a function of these demographic characteristics can be found in Supplemental Table 2.
Internal Consistency
Internal consistency of the items assessing motives for, antecedents of, and preoccupation with and thoughts about NSSI by proxy behaviors were generally acceptable, with Cronbach’s αs ≥.73 for the antecedents items across specific NSSI by proxy behaviors and ≥.86 for most of the motives items (with the exception of the items assessing motives for the behaviors of initiating injury via sports [α = .40] and engaging in elective or cosmetic medical procedures [α = .60]). In this sample, Cronbach’s α for the items assessing preoccupation with and thoughts about NSSI by proxy was questionable (α = .67). Likewise, internal consistency of the items assessing the presence of the eight NSSI by proxy behaviors included in the NSSIBPQ in this sample was lower than in Study 1 (split-half correlation: ρ = .32; average inter-item correlation: r = .09).
Validity of the NSSIBPQ
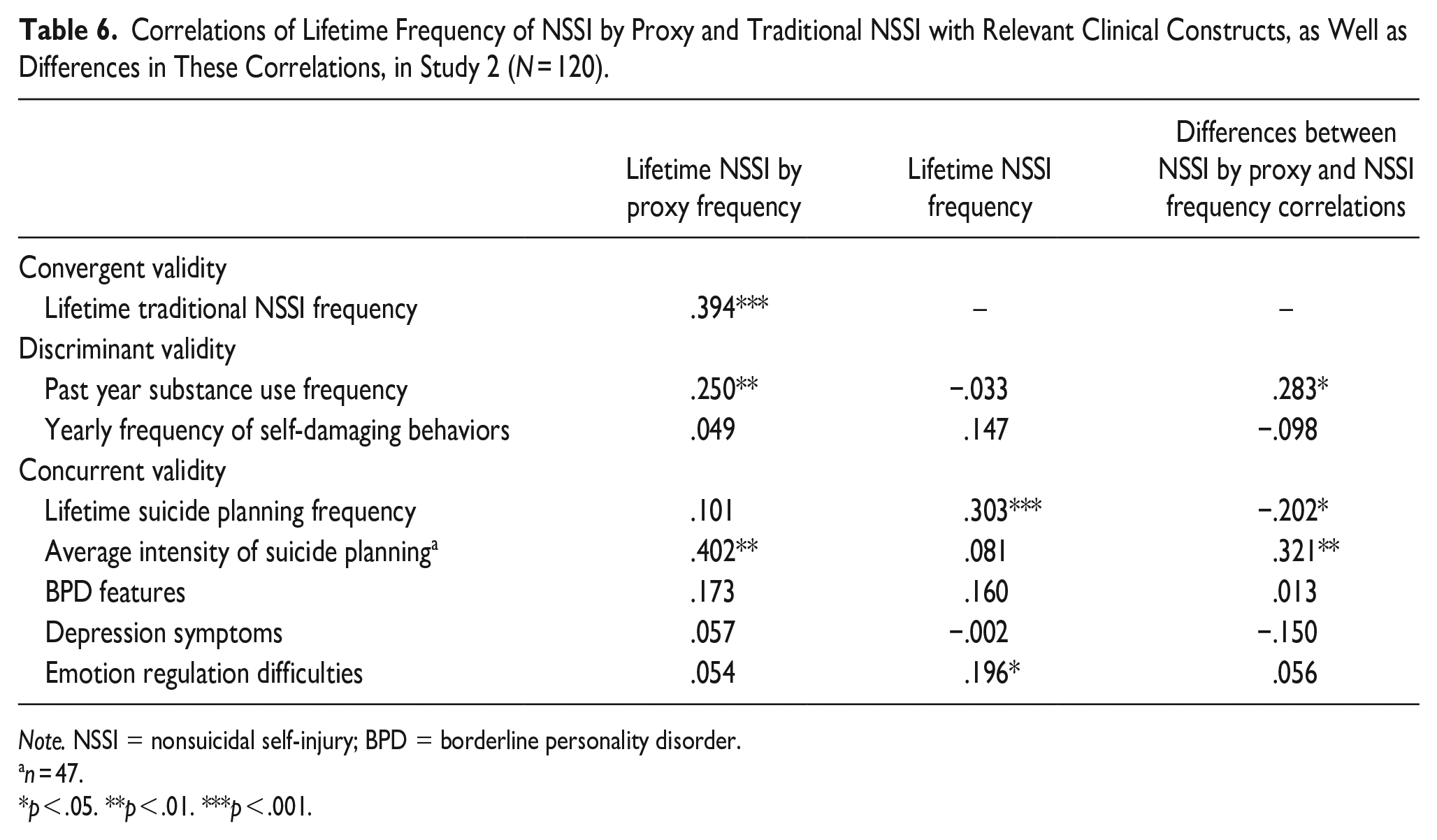
Correlations of lifetime frequency of NSSI by proxy with lifetime frequency of traditional NSSI, past-year substance use frequency, yearly frequency of self-destructive behaviors other than NSSI, and the clinical constructs of interest (including suicide planning, BPD features, depression symptoms, and emotion regulation difficulties) are presented in Table 6. For comparison purposes, the correlations of lifetime frequency of traditional NSSI with these constructs are also presented, along with the results of analyses comparing the strength of the associations of lifetime frequency of NSSI by proxy versus traditional NSSI with these other constructs.
Correlations of Lifetime Frequency of NSSI by Proxy and Traditional NSSI with Relevant Clinical Constructs, as Well as Differences in These Correlations, in Study 2 (N = 120).
Note. NSSI = nonsuicidal self-injury; BPD = borderline personality disorder.
n = 47.
p < .05. **p < .01. ***p < .001.
Convergent and Discriminant Validity
Providing some support for the convergent and discriminant validity of the NSSIBPQ, lifetime frequency of NSSI by proxy on the NSSIBPQ was significantly positively associated with lifetime frequency of traditional NSSI on the DSHI (r = .39). Moreover, this correlation was significantly higher than the correlation between lifetime frequency of NSSI by proxy and the frequency of other self-destructive behaviors (r = .05; z = 3.03, p = .003). Although it was also higher than the correlation of lifetime NSSI by proxy frequency with past year substance use frequency (r = .25), the difference between these correlations was not significant (z = 1.19, p = .236).
Concurrent Validity
Providing partial support for the concurrent validity of the NSSIBPQ, lifetime frequency of NSSI by proxy on this measure was significantly positively associated with the average intensity of suicide planning (although correlations with BPD features, depression symptoms, and emotion regulation difficulties were not significant in this sample; see Table 6). Notably, the absence of significant correlations between NSSI by proxy and these clinical constructs may be due to the more severe nature of this sample vis-à-vis NSSI and, thus, a restricted range on some of these variables, as traditional NSSI frequency also was not significantly associated with BPD features or depression symptoms within this sample. Moreover, the magnitude of the correlations of these clinical constructs with the lifetime frequency of both NSSI by proxy and traditional NSSI did not differ significantly (see Table 6). Further, the correlation between lifetime frequency of NSSI by proxy and average intensity of suicide planning was significantly higher than the correlation between this construct and the lifetime frequency of traditional NSSI (see Table 6).
Discussion
Utilizing a clinically relevant sample of emerging adults with current NSSI and suicidality, this study sought to characterize the nature and extent of NSSI by proxy within this sample and provide further data on the internal consistency and convergent, discriminant, and concurrent validity of the NSSIBPQ. Findings that 45% of this self-injuring sample endorsed a history of NSSI by proxy provide further support for the clinical relevance of this behavior, as well as its overlap with traditional NSSI. Indeed, consistent with the results of Study 1, findings revealed that the motives for and antecedents of NSSI by proxy are comparable to those found for traditional NSSI, with 96.4% of the sample endorsing emotion regulation motives for this behavior and 100% reporting the presence of negative thoughts and/or feelings prior to engaging in this behavior. Furthermore, and extending the results of Study 1, findings suggest that NSSI by proxy may be associated with clinically relevant levels of distress and impairment. Specifically, although NSSI by proxy was associated with mild to moderate levels of distress and functional impairment on average among all participants with a history of this behavior (lower than the levels of distress and impairment associated with traditional NSSI within this sample), almost half of the participants with NSSI by proxy reported moderate to severe levels of distress associated with this behavior and 14.5% reported at least moderate functional impairment due to this behavior. Thus, for a subset of individuals with NSSI by proxy, it appears that this behavior may cause clinically significant distress and/or impairment, consistent with an NSSID diagnosis.
Notably, results also revealed some differences in the associated characteristics of NSSI by proxy within this self-injuring sample (relative to the general community sample in Study 1), suggestive of the greater severity of NSSI by proxy within this sample. Specifically, almost all participants in this sample (98.2%) endorsed preoccupation with NSSI by proxy and 70.9% reported having thoughts about this behavior that were somewhat difficult to resist (relative to 75% and 47.5%, respectively, of the general community sample). Likewise, almost all the participants who reported engaging in NSSI by proxy within this sample (92.7%) reported that the person injuring them was not aware of their self-injurious intentions (relative to 76.3% of the general community sample).
Although generally acceptable for items assessing the associated characteristics of NSSI relevant to an NSSID diagnosis, internal consistency of the items assessing the presence of the specific NSSI by proxy behaviors included in the NSSIBPQ in this sample was lower than in Study 1, with one indicator suggesting a moderate association among the items and another indicating low internal consistency of these items. This may be due to the smaller sample size and resultant lower frequency of endorsement of these behaviors within this sample (relative to the sample in Study 1), as internal consistency estimates can be influenced by sample size (Clark & Watson, 1995; Streiner, 2003). Finally, results provided additional support for the convergent and discriminant validity of the NSSIBPQ, revealing a significantly stronger correlation between the frequency of NSSI by proxy on this measure and the frequency of traditional NSSI (relative to the frequency of self-destructive behaviors in general). Further, although neither traditional NSSI frequency nor NSSI by proxy frequency was significantly associated with BPD features or depression symptoms within this more severe self-injuring sample, findings of a significant association between frequency of NSSI by proxy and average intensity of suicide planning provide some support for the concurrent validity of this measure.
General Discussion
Although NSSI by proxy has recently been conceptualized as a clinically relevant form of NSSI, the use of another being (human or animal) to inflict the injury (albeit self-directed) has resulted in the exclusion of this behavior from most NSSI assessments, as well as research on NSSI (see Mann et al., 2022). Consequently, little is known about the rates of this behavior or its associated characteristics, and there are currently no validated measures assessing this behavior. Thus, the aims of this research were to characterize the nature and extent of NSSI by proxy in two nationwide community samples of young adults and provide preliminary data on the internal consistency reliability and validity of a new self-report measure of NSSI by proxy.
Providing support for the importance of continuing to assess NSSI by proxy in clinical and research settings, findings from both studies suggest that NSSI by proxy is a relatively common form of NSSI, with rates of this behavior in the general community sample (i.e., 18% lifetime and 8% past-year) approximating rates of traditional NSSI previously found in young adult community samples (see Kiekens et al., 2023; S. V. Swannell et al., 2014). Moreover, and supporting the conceptualization of NSSI by proxy as a clinically relevant form of NSSI, more than one quarter of the participants who engaged in traditional NSSI in both studies also endorsed a history of NSSI by proxy.
Findings from both studies also support the clinical relevance of NSSI by proxy and the potential for this behavior to meet criteria for an NSSID diagnosis. Specifically, and consistent with the research on motives for traditional NSSI (Turner et al., 2012; Zetterqvist et al., 2013), emotion regulation motives were the most commonly reported motives for NSSI by proxy across both studies. Moreover, all participants in the self-injuring sample and all but one in the general community sample reported the presence of negative thoughts and/or feelings prior to engaging in NSSI by proxy. Further, the vast majority of participants in both studies endorsed preoccupation with NSSI by proxy, and a substantial proportion of participants reported thoughts about NSSI by proxy that were at least somewhat difficult to resist. Finally, although the rates of at least moderate distress and impairment associated with NSSI by proxy were lower than the corresponding rates reported for traditional NSSI, it is important to note that nearly half of the participants with NSSI by proxy in the self-injuring sample reported moderate to severe levels of distress associated with this behavior and 14.5% reported at least moderate functional impairment due to this behavior. The comparatively lower functional impairment and subjective distress associated with NSSI by proxy (vs. traditional NSSI) may be due to the social acceptability of the behavior (thereby resulting in lower social impairment) and/or reduced severity of injury due to constraints of the proxy and social context. Future research exploring risk and protective factors for functional impairment and subjective distress among individuals who engage in NSSI by proxy versus traditional NSSI may clarify the reasons for these differences. Regardless, these findings suggest that a sizable subset of individuals with NSSI by proxy could meet criteria for NSSID on the basis of this particular form of NSSI alone.
Mann et al. (2022) proposed that the use of a proxy to inflict the injury in NSSI by proxy, as well as the topographical similarity of many NSSI by proxy behaviors to socially sanctioned behaviors, may allow for an external attribution of the injury and, thus, concealment of one’s self-injurious intentions. Findings from both studies support the centrality of concealment of self-injurious intentions and non-socially sanctioned motive(s) to NSSI by proxy. Across both samples, the vast majority of participants with NSSI by proxy reported that their proxy was unaware of their self-injurious intentions. Moreover, over 90% of participants in both studies reported being able to conceal the self-injurious intentions of their NSSI by proxy behind social norms to at least a moderate degree. The ability to conceal the self-injurious intentions of NSSI by proxy behaviors from society as a whole and the proxy injurer may also help explain the relatively lower functional impairment associated with NSSI by proxy versus traditional NSSI in this sample, as this likely has implications for the interpersonal consequences of NSSI by proxy. Indeed, the attribution model (Corrigan et al., 2003) suggests that behaviors perceived to be caused by others are viewed more favorably than behaviors for which the individual is perceived as bearing greater responsibility. Moreover, research has found that traditional NSSI is viewed more negatively than tattooing and nonintentional disfigurement (Burke et al., 2019). Thus, findings that the vast majority of participants were able to conceal the self-injurious intentions of their NSSI by proxy both in general and from their proxy specifically may lessen the social impairment associated with NSSI by proxy relative to traditional NSSI (ultimately accounting for findings of lower functional impairment due to NSSI by proxy vs. traditional NSSI).
Consistent with Mann et al.’s (2022) suggestion that it may be more likely for NSSI by proxy to follow traditional NSSI in time, findings across both studies revealed a significantly earlier age of onset for traditional NSSI versus NSSI by proxy. One explanation may be that individuals transition from NSSI to NSSI by proxy due to the stigma associated with traditional NSSI behaviors and the greater ability to hide the self-injurious intentions of their behaviors in the context of NSSI by proxy. Alternatively, many of the assessed NSSI by proxy behaviors are associated with cultural or legal age restrictions that may hinder initial exposure to these behaviors. For example, in the United States, there are laws restricting the ability to get a tattoo among individuals under the age of 18. Although further research is needed to clarify the developmental trajectories of these behaviors within individuals, these findings suggest that traditional NSSI may be more likely to precede NSSI by proxy than vice versa.
Notably, despite evidence that NSSI by proxy serves similar functions to traditional NSSI while allowing an individual to conceal the self-injurious intentions of the behavior (arguably making it more socially acceptable), there was a preference for traditional NSSI over NSSI by proxy among individuals with both types of NSSI behaviors across the two studies (with this preference being particularly strong among the sample selected to have a history of repeated NSSI). The top four reasons for preferring traditional NSSI to NSSI by proxy were consistent across samples and focused on the perception of traditional NSSI as more in the respondent’s control, easier to do, easier to hide, and more immediate. Conversely, for the small subset of participants who reported preferring NSSI by proxy, one of the most commonly endorsed reasons for this preference across both studies was the perception of NSSI by proxy as more socially acceptable, consistent with Mann et al.’s (2022) proposal that NSSI by proxy may be preferred by some individuals because it is viewed as more socially acceptable than traditional NSSI. As noted above, it is possible that the perception of NSSI by proxy as more socially acceptable could, for some individuals, lead to a transition from traditional NSSI to NSSI by proxy over time (within or outside the context of therapy). Given the distress and impairment that may be associated with NSSI by proxy, it is important for clinicians working with self-injuring clients to ensure that ongoing assessments of NSSI include both traditional NSSI behaviors and NSSI by proxy (so that clinically relevant forms of this behavior are not missed in the context of treatment).
Within the general community sample in Study 1, rates of NSSI by proxy were higher among female (vs. male) participants, transgender/gender expansive (vs. cisgender) participants, sexual minority (vs. heterosexually identifying) participants, and participants with lower (vs. higher) education and income levels. These differences are consistent with research on demographic differences in traditional NSSI, which demonstrates disproportionately high rates of NSSI among sexual and gender minorities (Liu et al., 2019; S. Swannell et al., 2016), female adolescents and young adults (Bresin & Schoenleber, 2015), and individuals of lower socioeconomic backgrounds (Baetens et al., 2014; Liu, 2023; Park et al., 2022; Robinson et al., 2017). Although rates of NSSI by proxy did not differ significantly as a function of any examined demographic characteristics in Study 2, this is likely due to the characteristics of this sample (i.e., the fact that all participants were specifically selected for recent repeated NSSI). Thus, the results within this sample may be more accurately described as an absence of demographic differences between individuals with co-occurring traditional NSSI and NSSI by proxy versus those with only traditional NSSI.
Finally, results of both studies provide preliminary support for the convergent, discriminant, and concurrent validity of the NSSIBPQ. Specifically, across both studies, lifetime frequency of NSSI by proxy on the NSSIBPQ was more strongly associated with lifetime frequency of traditional NSSI than with the presence and frequency of other health risk behaviors (including lifetime suicide attempt status, past-year substance use frequency, and yearly frequency of self-destructive behaviors). Moreover, findings of significant associations between the lifetime frequency of NSSI by proxy and relevant clinical constructs (including suicidal ideation and planning, BPD and depression symptoms, and emotion regulation difficulties in Study 1 and suicide planning in Study 2) provide initial support for the concurrent validity of the NSSIBPQ. Findings that NSSI by proxy was significantly associated with the average intensity of suicidal ideation and planning in both samples (and that the strength of these associations was comparable to or greater than the associations of these constructs with traditional NSSI) highlight the clinical relevance of NSSI by proxy and the importance of continuing to direct clinical and research attention to this understudied behavior. Indeed, although NSSI is considered antithetical to suicidal behaviors (Muehlenkamp & Kerr, 2010), growing research indicates a strong association between NSSI and suicide risk (Hamza et al., 2012). The results of this study suggest that NSSI by proxy may have a comparable relationship to some facets of suicide risk and constitutes an important clinical target for assessment and intervention.
Limitations and Future Directions
Results of these studies must be considered in the context of study limitations. First, given that there are no available measures of NSSI by proxy with which to compare the NSSIBPQ, we were only able to assess the convergent validity of this measure with respect to an established measure of a different form of NSSI (i.e., traditional NSSI), relative to measures of other health risk behaviors. In addition, all constructs were assessed via self-report measures, which may be limited by social desirability biases or recall difficulties. Future research should incorporate structured clinical interviews and/or timeline follow-back procedures to provide a more rigorous assessment of the construct validity of the NSSIBPQ. Furthermore, the inclusion criteria for Study 2 (including the presence of serious suicidal ideation and repeated NSSI, and the absence of suicide attempts) resulted in a unique sample that, while relevant to an investigation of NSSI by proxy, likely influenced the observed associations among NSSI by proxy and the other clinical constructs of interest and precluded examination of the associations of NSSI by proxy frequency to suicidal ideation and suicide attempts within this sample. The modest sample size in Study 2 may have further influenced our ability to identify significant associations between NSSI frequency (both traditional NSSI and NSSI by proxy) and the clinical constructs of interest, influencing findings pertaining to the concurrent validity of the NSSIBPQ. Future research using larger and more nationally representative samples of individuals with NSSI by proxy is needed. In addition to facilitating a more comprehensive investigation of the construct validity of the NSSIBPQ, the use of a larger sample with greater endorsement of NSSI by proxy behaviors would permit more sophisticated analyses of the psychometric properties of the NSSIBPQ, including examination of the factor structure of this measure using exploratory and confirmatory factor analysis. Prospective research is also needed to examine the predictive validity of the NSSIBPQ with regard to the examined clinical constructs (e.g., suicide risk) and other clinical difficulties theoretically linked to NSSI, as well as establish the reliability of this measure for assessing NSSI by proxy over time.
Likewise, the focus on young adults within both samples limits the generalizability of the findings to adolescents and older adults and necessitates future research examining NSSI by proxy within these populations as well. In addition, although the use of two nationwide community samples was a strength of this research (providing more diverse samples than often used in NSSI research and, for the general community sample in Study 1, allowing us to better approximate the rate of NSSI by proxy among community young adults), findings may not generalize to more severe samples, including clinical samples of patients with severe NSSI and/or suicidality. Additionally, the general community sample intentionally oversampled sexual minority individuals, whereas the self-injuring sample (likely by virtue of the focus on NSSI and suicidality) was comprised of a large proportion of individuals identifying as a sexual minority. The overrepresentation of sexual minority individuals within both samples may limit the generalizability of the findings to heterosexual young adults, particularly since sexual minority individuals consistently report greater rates and levels of traditional NSSI than their sexual majority peers (Liu et al., 2019; S. Swannell et al., 2016). However, the racial/ethnic and gender diversity of both samples is a strength of this research and increases the likelihood that results will generalize to diverse young adults. Nonetheless, future research should investigate the presence, frequency, and associated features of NSSI by proxy within different populations (e.g., adolescents, patients in inpatient and outpatient settings, individuals with different psychiatric disorders), as well as in nationally representative samples to ascertain the prevalence of this behavior.
Conclusion
Given that NSSI by proxy has only recently been identified as a distinct form of NSSI in need of systematic empirical and clinical attention, there have been no systematic studies of NSSI by proxy or its associated characteristics, and there are no available measures of this construct to guide research or clinical assessment. Consequently, this research sought to examine and validate a new questionnaire of NSSI by proxy—the NSSIBPQ—within both a general community sample and self-injuring community sample of young adults. Results provide preliminary support for the internal consistency and convergent, discriminant, and concurrent validity of the NSSIBPQ within this population, and suggest its utility as a research and clinical tool for examining NSSI by proxy. Findings also highlight the clinical relevance of NSSI by proxy among young adults, underscoring the need to further investigate this behavior.
Supplemental Material
sj-docx-1-bmo-10.1177_01454455231191710 – Supplemental material for Examining the Presence, Frequency, and Associated Characteristics of Nonsuicidal Self-Injury by Proxy: Initial Validation of the Nonsuicidal Self-Injury by Proxy Questionnaire (NSSIBPQ)
Supplemental material, sj-docx-1-bmo-10.1177_01454455231191710 for Examining the Presence, Frequency, and Associated Characteristics of Nonsuicidal Self-Injury by Proxy: Initial Validation of the Nonsuicidal Self-Injury by Proxy Questionnaire (NSSIBPQ) by Adam J. D. Mann, Matthew T. Tull and Kim L. Gratz in Behavior Modification
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by funding from the Department of Psychology at the University of Toledo, Toledo, OH, USA.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.