
Abstract
Appreciative inquiry has become increasingly popular as a method for facilitating organisational or systemic change through focusing on the positive aspects and ‘life giving properties of a system’ as opposed to traditional ‘deficit-based’ approaches. However, there has been criticism that this process could invalidate negative experiences of organisations and/or systems. This is particularly problematic if an existing system is seen by its users as providing little value or if there is potential dissonance regarding system value among key stakeholders. Using two case studies of open appreciative inquiry by Plymouth City Council staff, this article outlines how the use of a liberally defined, human-learning-system informed, approach to appreciative inquiry has been used not to identify positive narratives so much as to surface potential dissonance and develop empathy and deeper insight conducive to systemic change. It concludes with a discussion of factors that might help organisations use appreciative inquiry where dissonance is likely to exist and a tentative labelling of this approach as “open appreciative enquiry” with an emphasis on the “e”.
Keywords
Introduction
Appreciative inquiry (AI) has been cited as a powerful means through which managers and practitioners in public services can bridge the often-crucial gaps between research, learning and practice (Hung et al., 2018). However, the perceived focus on the positive can lead to concerns it may not be suitable where a system appears to be manifestly failing. This paper explores how a local authority in England has achieved systemic change using an adapted approach to AI which could have practical applications in other organisations and settings.
Background
AI is an increasingly popular approach to facilitating organisational or systemic change (Bushe and Kassam, 2005; Cooperrider, 2013). From Cooperrider’s first presentation of AI theory to the 1985 Organisational Development Network Conference in San Franscico, AI has broken into the mainstream of organisational development (Bushe, 2012) and has been embraced by hundreds of organisations, including the UN (Cooperrider, 2013; Ludema and Fry, 2008). Definitions can vary but AI is commonly seen as focusing on the positive aspects and ‘life-giving properties’ of a system as opposed to traditional problem-solving or deficit-based approaches (Grant and Humphries, 2006; Duncan and Ridley-Duff, 2014; Sharp, 2018; Ludema and Fry, 2008), a fundamental assumption being that in ‘every group, society or organisation something works’ (Hammond 1998 cited in Trajkovski et al., 2013).
AI has been described as more a ‘philosophy’ than a ‘research method’ (Duncan and Ridley-Duff, 2014) and certainly Cooperrider was resistant to setting out a specific method for many years (Bushe and Kassam, 2005). Nonetheless, Cooperrider and Srivastva’s (1987) seminal paper emphasised four key principles. First, research should begin with appreciation, on the assumption ‘that every social system “works” to some degree’ and research should look to identify and explain those “life giving” elements of a system. Second, research should be applicable – ‘used, applied and thereby validated in action’. Third, it should be provocative in that the organisation’s members are motivated into shaping the social world through their own moral values and imaginative ideas. Finally, it should involve a collaborative relationship between the researcher and the members of an organisation. As demonstrated in Trajkovski et al.’s (2013: 1229–30) systematic review this can involve applying a range of methods including meetings, interviews and focus groups.
As Bushe and Kassam (2005: 167) note, AI is commonly associated with the 4-D cycle elaborated in Cooperrider and Whitney (1999). This starts with ‘discovery’ (appreciating the best of what is), followed by ‘dream’ (imagining how it could change for the better), ‘design’ (clarifying the ideal) and ‘destiny’ (creating positive change). Although Cooperrider and Whitney (1999) emphasised that AI is more than just the 4-D model it has at times come to be seen as an intrinsic feature of the approach. All but one of the cases in Bushe and Kassam’s (2005) meta-analysis used the 4-D model and Trajkovski et al. (2013) viewed the 4-D approach as integral to AI in their systematic review.
One advantage of AI is its ability to motivate employees who may otherwise be resistant to organisational change by engaging them in a process which builds on what is working well already rather than on problems (Johnson and Leavitt 2001). As Hung et al. (2018) note, by involving practitioners and employees in the research, AI can help break down the problematic dichotomy between knowledge and practice.
While AI has expanded beyond the discipline of organisational development, most AI exercises tend to be undertaken with staff or official stakeholders of a relevant organisation, rather than other groups such as “end-users” and citizens. Of the nine studies in Trajkovski et al.’s (2013) review, two were conducted with end users (the families of children with complex needs and older people with dementia) while the rest were with staff. Notable exceptions include Duncan and Ridley-Duff (2014) who undertook AI with Pakistani women, who they argue are one of the most excluded groups within the UK.
Criticisms of AI
Despite, or rather because of its success, AI has attracted several important criticisms. Bushe (2012) identified three waves of criticism each coming from different perspectives (traditional ‘positivist’ informed organisational development; social constructionism and critical theory with, in Bushe’s view, an ignorance of AI; and sympathetic but critical scholars). All ‘questioned the exclusive focus on the positive.’ In the case of the sympathetic third wave there is a common concern that the focus on the positive in the discovery phase could invalidate, ‘crowd out’ or repress negative organisational and systematic experiences (Bushe, 2012).
It is notable that in the case of Duncan and Ridley-Duff (2014), where the participants were Pakistani women in Sheffield, such a situation did initially occur. Having adopted an AI approach due to concerns that a problem-focused approach might reinforce feelings of powerlessness amongst participants, the researchers found themselves trying to steer the discussions towards the positive when the participants raised issues of hardship and oppression. In the end, while the use of AI was not abandoned, the research team had to modify their approach so that positive, strength-focused stories were not privileged at the expense of negative experiences. A similar issue occurred for Grant and Humphries (2006) who reflected that deflecting attention from negative participant contributions may have lost them opportunities to learn important lessons.
These criticisms of AI have stimulated some modifications in how it is conceived. Bushe (2012: 15) noted how several authors had started to emphasise ‘the generativity’ of AI as opposed to ‘the positive’ leading to a modified definition of the concept. For example, Fitzgerald et al. (2010: 221) noted how ‘what gives life’ is often conflated with ‘the positive’ in AI and suggest a looser definition of AI “as people inquiring together into the infinite potentials and varieties of human organising”. Zandee and Cooperrider (2008) meanwhile emphasised the role of appreciation in stimulating a ‘spirit of enquiry’ as opposed to a focus on the positive. More recently Sharp et al. (2018), dispensed with the term to describe their research and instead adopted a modified AI approach they called ‘Appreciative Action Research’. Recognising that ‘the focus on positivity has perhaps neglected the collaborative and experimental dimensions of the four-staged process’, their Caring Conversations Framework focuses on developing generative (rather than necessarily positive) appreciative and relational capacities. Similarly, Grant and Humphries (2006), associated by Bushe (2012) with the ‘second wave’ of AI criticism, coined the term ‘Critical Appreciative Processes’ to describe their ‘critical theory’ informed approach to AI. A central part of this concept was to expand the term ‘appreciation’ to ‘also mean to know, to be conscious of, to take full or sufficient account of.’
The ‘third wave’ criticisms of AI certainly raise questions about whether the approach can be as transformational as its advocates claim, particularly where a system may require fundamental reform. Can AI really stimulate positive change where the users of a service perceive that service, system or organisation not to be delivering anything of value to them? What changes might be needed to the approach to ensure that AI does not exclude or devalue the negative experiences that people may have?
The approach in Plymouth
The Plymouth City Council Public Health Team (PCC PHT) adopted AI as a tool to facilitate organisational and systemic change as part of its interest in the organisational change philosophy, Human Learning Systems (HLS). HLS is an alternative to the dominant paradigm of New Public Management (NPM), with its focus on ‘markets, managers and metrics’ (Brogan et al., 2021). As Head and Alford (2015) note NPM has generally been ill-suited to dealing with the complex and ‘wicked’ problems often faced by public sector managers, in part due to the fragmentation between services that it encourages. Therefore, researchers and practitioners have looked to broader ways of thinking about social problems using complexity theory and systems thinking (Head and Alford, 2015).
HLS emerged from such thinking (Lowe et al., 2021) and is based on the following principles (Brogan et al., 2021). First, the purpose of public service is to support human freedom and flourishing. Second, to understand humans, you must understand their world (i.e., the web of relationships or ‘systems’ that define who they are). Third, the complexity and changeability of a person’s life context means that learning is the only viable management strategy. Finally, the outcomes of peoples’ lives are created by the workings of complex systems and changes to such systems are required to create new outcomes (Brogan et al., 2021).
As Lowe et al. (2021) point out, HLS has provided a way of conceptualising shared but, often unseen, practices that some managers and practitioners have put in place to address the challenges complexity poses for public sector organisations. In the case of Plymouth, one of the authors had been using approaches which would later be seen as HLS as early as the turn of the century and saw the potential for AI to contribute to this approach after attending a Systems Leadership course run by the Leadership Centre in 2014/15.
As a participatory form of action research (Cooperrider and Srivastva, 1987; Trajkovski et al., 2013: 1225), involving a collaboration between researcher and participant and a focus on the latter’s part in imaginatively shaping the social world, AI has the potential to complement the ‘person’ or ‘human focused’ core of HLS. Similarly, by eliciting positive feedback, grounded in experience, AI forms a useful pedagogical tool for organisations to engage in continuous learning (Grandy and Holton 2010) using a strengths-based approach, an essential part of HLS (Lowe et al., 2021). Finally, AI understands organisations as ‘systems’ – the key unit of analysis of HLS – and recognises the need to engage the system ‘as a whole’ (Brogan et al., 2021; Cooperrider and Srivastva, 1987; Neville, 2007). As Zandee and Cooperrider (2008) point out, AI can enable the researcher to engage with the “complex, messy and emergent nature of organisational and societal life”.
However, we also note areas of divergence between AI, as typically framed, and the HLS approach. There is a potential danger that AI, concerned with finding the positives of a system or intervention could simply result in a false validation of existing practice. To be truly ‘human focused’ the experience of ‘service-users’ needs to be appreciated regardless of whether it is positive or negative. While, as noted earlier, AI has been described as a ‘philosophy’ from PCC’s perspective the philosophical foundation is HLS, with AI playing more of an instrumental and methodological role. Considering this, it is not surprising that there are some elements of PCC’s approach which distinguish it from more conventional forms of AI.
First, in terms of purpose, some of the ways in which PCC has used AI differ from how it is conventionally applied. The below provides a short summary of the Council’s aims when using AI: (1) To get people to listen to people without preconditions/service-based assumptions (2) To use the process to build empathy between people (3) As an ‘easy’ way to check how ‘experiments’ (often an integral part of implementing HLS) are going and learning is captured (4) As a means to resolve ‘disputes’ about what is important
There is also an understanding that a key learning point from the practice of AI is that it can reveal or surface dissonance within systems. Often this is dissonance between what NPM suggests is the situation (e.g. a system is working because the targets are met) and the experiences of people involved (e.g. the system is not helping). This may reflect differences in how ‘systems’ themselves are defined. As Boulton et al. (2015) point out, part of the complexity around human systems relates to the ambiguity around how they are interpreted and defined by different people, necessitating what Ison (2008) refers to as ‘boundary judgements’. While practitioners may use a performance target, identified need or type of service when defining a ‘system’, HLS uses the individual and their web of relationships as the starting point. For example, practitioners may define the system to support families struggling with childhood obesity to be limited to targeted support around nutritional advice. However, the feedback from the families themselves may suggest this issue depends on a much larger system, including employment, mental health support and other areas (see Example 1 below). As such, AI has often been used as a gateway to HLS thinking within the Council both in terms of revealing the inadequacies of an NPM approach and in providing a tool through which HLS can start to be embedded amongst staff.
While most of the four aims listed above sit comfortably with Cooperrider and Srivastva’s (1987) principles of AI, the first, around listening without preconditions, is perhaps controversial given the assumption, inherent in the first principle of AI that something in every “social system” works. Moreover, the focus on dissonance appears to run counter to AI’s emphasis on avoiding ‘deficit-based’ approaches and building a positive case for change. We will consider this issue further in the discussion below but for now it is best to emphasise that a distinction should be drawn between the use of appreciation as a method, and the surfacing of dissonance as an aim.
A second difference regarding PCC’s approach to AI relates to method. AI as practiced by PCC tends to be more informal and indeed has often been defined as “appreciative enquiry” rather than “inquiry.” The 4-D model has only been used for some of the projects and tends to be applied as a tool to help prompt and guide, rather than lead the discussion. The interviews are often very open in the sense that there is minimal structure and they never start with a service based question. This provides more opportunity for the participants to shape the conversation with their perspectives, dreams and indeed problems, exemplifying principles of ‘authentic’ co-production including the current roll-out through the public health team of ABCD approaches (i.e. training of elected members, staff and community builders) (Knowles et al., 2021; Russel 2020). Consequently, the difficulty of suppressing potentially negative feedback, noted by Duncan and Ridley-Duff (2014), is reduced.
In addition, while no one AI exercise is the same, Plymouth’s approach tends to involve some innovations that are not necessarily present in conventional AI. One is the practice of sending practitioner-researchers out in pairs, with one person asking the questions and the other listening and taking notes. Often people from different places in the hierarchy or different teams/organisations are paired to help develop their empathy for each other as well as for the individual being interviewed, a key requirement of HLS (Brogan et al., 2021). A group of practitioners (those who have collected stories, and sometimes those who have not) is then convened to share the stories which they are encouraged to read in the first person, again to build empathy. This in turn generates the energy and motivation among practitioners to explore how services can be transformed to address the issues arising in the interviews. In some cases, this can even lead to subsequent innovations which themselves are tested using AI, creating a cyclical learning approach (as outlined in Chart 1). AI cycle at Plymouth City Council.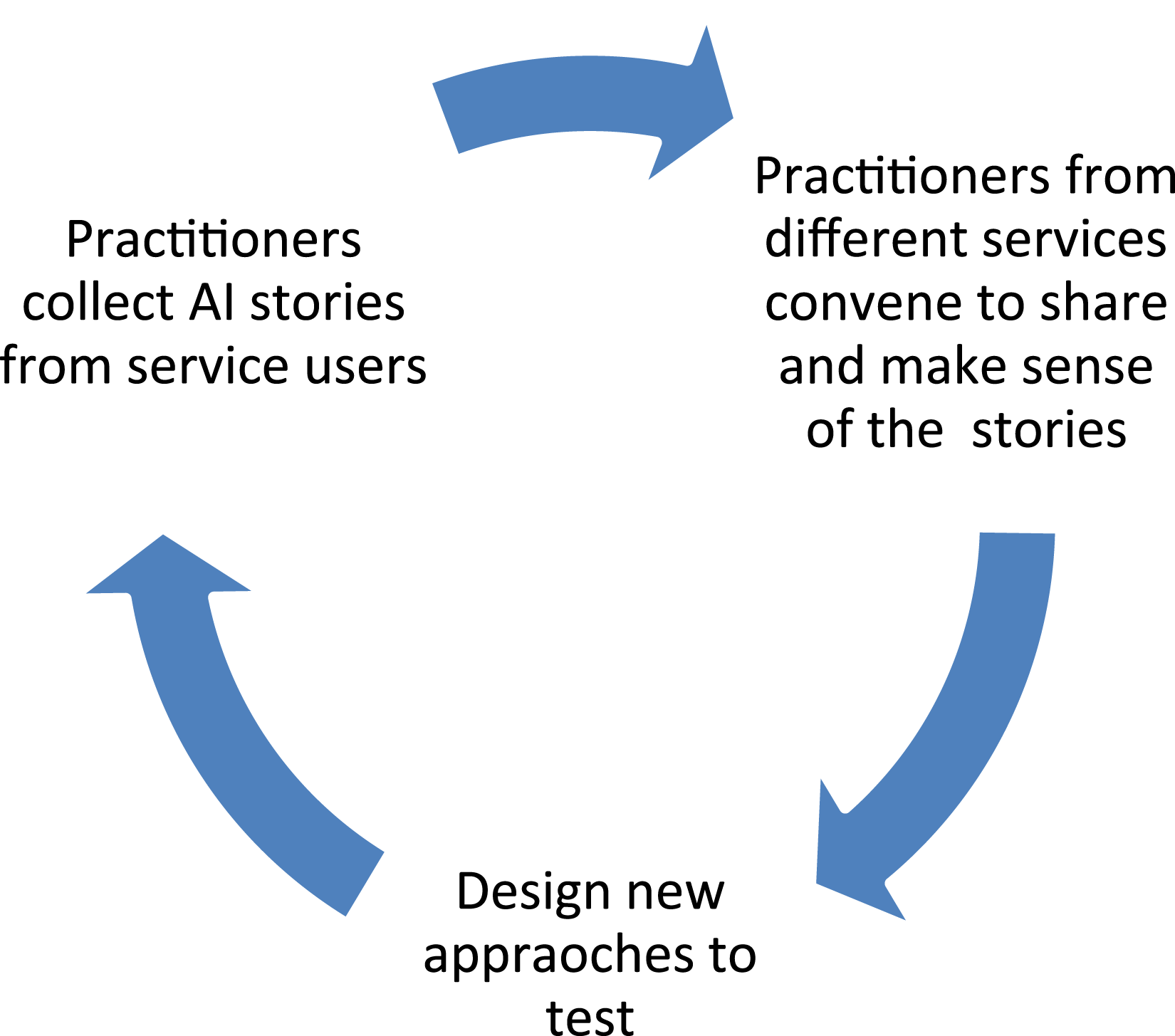
An important outcome of this approach is the way in which it changes the attitudes, values and freedoms of staff themselves. Box 1 provides reflections from two of the authors, both members of the Council staff, about how appreciative enquiry has been adopted within the Council. “We have been on a ‘journey’ in Plymouth. The drive for integration and the fact we have colleagues willing to take risks and experiment has provided opportunities to create an environment where this approach can flourish. There is a lot of trust and relationship-based decision making that has created conditions for not just the use of AI but to be able to act on what the stories tell us.” “I came from what felt like quite a bureaucratic job, and at the time I joined the Public Health team, the Council seemed to me to be driven by what I now know as a ‘New Public Management’ paradigm. Things have changed though and I think expanding the team with Advanced Practitioner posts has been a part of this. It has enabled us to build work delivering activity traditionally seen as “lower down the hierarchy” rather than strategy development, which has modelled our way of working. One of the first people to do appreciative inquiry in the wider public health team (it was already used extensively by the Plymouth Alliance – a collaboration formed to support people living with complexities such as homelessness, substance misuse and poor mental health) went into schools to talk to with kids about their weight, I decided to go with her and saw appreciative inquiry in action, which inspired me to shift more towards that way of working.”Box 1: Perspectives on appreciative inquiry
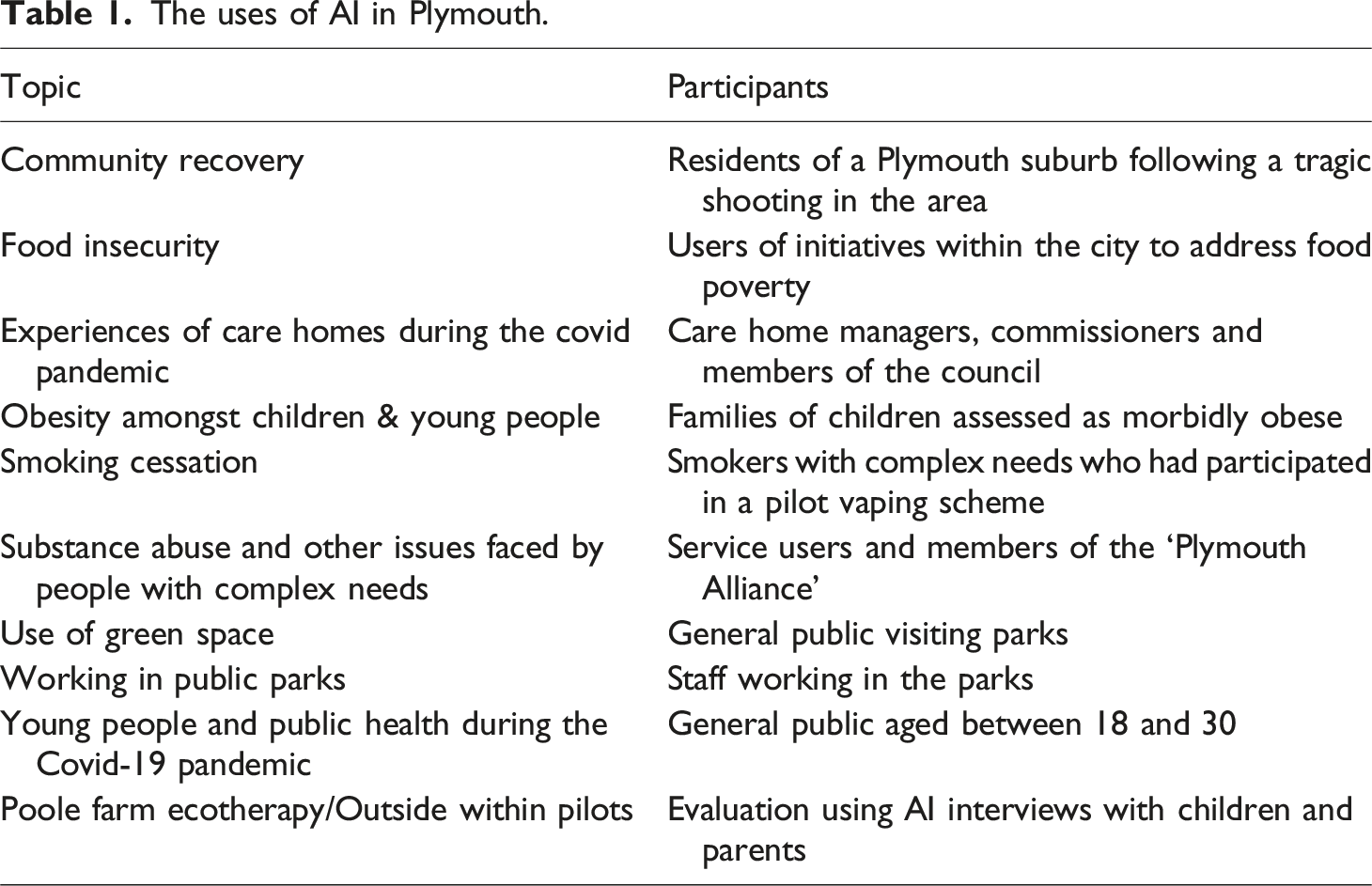
The uses of AI in Plymouth.
AI in practice in Plymouth: Two case studies
To allow depth of exploration, we focus below on just two of these examples: childhood obesity and smoking cessation, to provide an insight into the forms and functions of PCC’s approach.
Example 1 – Refocusing the service offer for child obesity
A third of children leaving primary school in England are overweight or obese (NHS England, 2023), making them more vulnerable in the future to a range of conditions including type 2 diabetes, high blood pressure, high cholesterol and an increased risk of respiratory, musculoskeletal and liver diseases. For years PCC, like most local authorities, had been trying to deal with this issue by providing highly specialised, dietetics focused, services to the families of children identified as being at risk of severe obesity (the Tier 2 Weight Management Service). Despite considerable investment and effort, the council could not recruit or retain families on the course and therefore help children to lose weight.
Despite the lack of success with the intervention there were obstacles to organisational reform, not least resistance from existing commissioners, some of whom were reluctant to move away from an existing strategy they had been proud to contribute towards. Additionally, there was a fear that the alternative to existing practice was to do nothing. Indeed, should AI have been undertaken in the traditional way with staff or the commissioners, the focus on ‘discovering’ the positives might have hindered the possibility of organisational change. A common response to the problem from the medical profession was to request an increase in the number of dieticians.
Instead, the Public Health Team (PHT) decided to undertake an AI exercise with the families themselves with the aim of developing narratives that could explain why the current childhood obesity intervention was not working. Rather than generate change by focusing on the positive, the PHT sought to amplify existing dissonance by providing a voice to the people the service was supposed to be helping but was failing. It also looked to develop their testimonies into a powerful set of narratives that would generate empathy and genuine engagement about service change.
The first step was to train School Nurses and Health Visitors in AI methods. Ten families were subsequently interviewed by two practitioners, one to listen and the other to make notes. For this exercise, the traditional 4-D method was used, albeit to provide an overall framework and set of prompts for the conversations rather than a specific set of questions. However, during the initial ‘discovery’ phase (where participants are invited to ‘appreciate what is’) the prompts focused not on what was good about the system but instead their own family (e.g., ‘what you most enjoy/respect in your son/daughter?,’ ‘what was your most triumphant moment as a family’). Importantly, while most of the prompts tended to emphasise the positive, the conversations were kept open to enable the emergence of different perspectives.
The stories that were written up highlighted several significant issues linked to the subject of childhood obesity including poverty, domestic abuse and mental health. They also highlighted the suspicion of many families towards authority, especially linked to worry about having their children taken away from them. Perhaps most significantly, the families valued the relational skills and qualities of professionals more than anything and it was only when such skills were evident that they would also value recommended therapeutic approaches.
Having collected the stories from the families, the next step involved a process where the stories were shared with the wider children’s health system and read aloud as a group. The first round of stories was completed with the PHT, followed by managers from children’s social care and children’s health. Participants were split into pairs and given one of the stories, which one of the pair read out, while the other made notes on themes. Importantly the reader had to read the story in the first person so as to help build empathy. As mentioned above, this is an approach PCC commonly uses for AI and provides a demonstration of how AI can not only help develop a collaborative (and non-hierarchical) relationship between the researcher and participant (along the lines of Cooperrider and Srivastva’s (1987) fourth principle) but also with policymakers and other stakeholders.
Partly as a consequence of the empathy developed through the AI sessions, PCC and its partners developed a new approach – the Compassionate Approach to Children and Young People’s Health & Weight: Strategic Action Plan (Plymouth City Council, 2023). The plan includes several features informed by the AI sessions such as supporting those who require the most help, cost public services the most money and face multiple issues which require generalist bespoke support as opposed to specialist help in one narrow area (like dietetics). Another key aspect was the conscious move away from any language associated with shaming and judgement as well as confrontational or business-like terms, all of which can be counter-productive when addressing weight issues. Instead, a more positive focus is demonstrated by the very plan’s title with its focus on ‘health’ and ‘weight’ as opposed to ‘obesity.’
Importantly the plan explicitly embraces a whole systems approach through HLS. Rather than, as previously, relying on one or two specialist services, the plan maps a system centred around the individual (the starting point for HLS) including not only specialist services (e.g. dieticians, social workers and consultant and specialist nurses) and generic children and young person services but also communities and families. Hence, the AI informed a more expansive definition of what Ison (2008: 143) would call the ‘system of interest’ which the Council and partners agreed to work with. This approach is also reflected in the actions which range from creating healthier food environments, to support for breastfeeding, increasing active travel and working with schools and childcare settings. Thus, the plan explicitly recognises that the complexity of human systems means that meaningful change will take time and adopts an approach of continued learning and improvement over its 10-year timeline (Plymouth City Council, 2023: 6).
The first annual report was promising with a school in the relatively deprived area of Barne Barton reporting how the whole-system and collaborative approach is starting to directly benefit their pupils (Plymouth City Council, 2024). Further details of the impact of AI on the strategic approach are contained in Box 2 which includes the perspectives of one of the authors involved in the strategy. “The transformational consequence of AI was clear in the strategic direction and policy decision making. The sense checking of the discussions, the themes identified and lived experience captured clearly demonstrated the need to address this issue in a very different way. Given my proximity to the development of this work it is very clear that these AI stories helped reframe the thinking on how we should address this issue; emboldened those of us working on this to be brave and provided powerful evidence for senior leaders and strategic groups to ‘take the risk’ of going down a very ambitious ‘new’ approach. It was these elements - taken together - that has created the change. The underpinning of a compassionate approach and the focus on relational working were also central to this work and again these flowed from the AI. Outputs and outcomes we are seeing now are directly down to this approach.”Box 2: Perspectives on appreciative inquiry
Example 2 – Stepping out of the guidelines for smoking cessation for people with complex needs
Smoking is the number one cause of preventable death in England and is a powerful driver of health inequalities (Public Health England, 2016). However conventional smoking cessation services, which are set-up to support people who have already decided they want to quit, struggle to successfully engage with people with complex needs who may be, among other things, more heavily dependent on tobacco.
This was certainly the experience for PCC prior to 2019 when their smoking cessation offer was largely limited to a NICE Guidance based service where, typically, three behavioural sessions over 12 weeks were, and indeed still are, offered, alongside the provision of either nicotine replacement therapy or vapes for people prepared to set a ‘quit date’.
In November 2019, the PCC PHT organised an ‘experiment’ with the help of two VCSE partners, whereby free vapes were provided to citizens with complex needs who smoked irrespective of whether they consciously wanted to quit. A vape kit, with a choice of flavours and instructions on how to use it was offered to 30 individuals of whom 27 accepted. Despite the participants having no conscious intention of quitting smoking data from the 5-week follow-up found that 22 of the 27 participants had reduced or ceased smoking since joining the scheme.
To understand what might be working well with the ‘experiment’, AI interviews were undertaken with five of the recipients. The interviews were very open (the 4-D approach was not utilised and the two questions were simply ‘tell me about your life?’ and ‘how you are getting on with the vaping?’), with a focus on exploring the positives as opposed to problem-solving. Despite this the interviews did elicit some negative feedback regarding traditional smoking cessation services, as noted in the short reflection from one of the authors, who was involved in the delivery of the AI (see Box 3). “Some of (the AI attendees) told us they felt like they wouldn’t go to a service on smoking because they expected people would look down on them and would tell them things they already knew about health, rather than give them realistic options about what they could do. There was this overriding and sometimes apparently subconscious feeling of stigma.”Box 3: Perspectives on appreciative enquiry
In contrast participant feedback on the pilot project was highly positive noting that, in contrast to a conventional smoking cessation scheme, there were “no strings attached” to the vaping scheme and that they didn’t feel they were being judged for being smokers. In their meta-case analysis of appreciative inquiries Bushe and Kassam (2005) note that the ability of AI to introduce generative metaphors that facilitate change is a key distinction between AI and more conventional organisational development techniques. The term “no strings attached,” which emerged from the interviews and was subsequently used as the title of an ongoing project based on the pilot is an excellent example of such a metaphor. The project, which was first rolled out at the start of the pandemic is ongoing and provides the Council with a smoking cessation offer to people with complex needs which previously did not exist. Monitoring data has shown that the 5-week ‘quit rate’ is higher in ‘No Strings Attached’ than traditional treatment and the intervention is considerably less expensive.
Whilst PCC continues to provide a NICE-based conventional smoking cessation offer to those able and willing to set a quit date, the roll-out of the “No Strings Attached” offer marked a step change in PCC’s smoking cessation services for people with complex needs. This has recently been expanded to other communities with which the conventional structured support offer routinely and traditionally failed to engage with. The AI stories and success of the offer also led to a new focus on improving self-efficacy as well as to the roll-out of AI training to other staff in the One You Plymouth (health improvement) team, which was used to spread the HLS approach. Interest in this more proactive, relational and human-centred approach, which seeks to engage with citizens whilst avoiding stigma, has also spread to other local authorities.
Discussion
While AI can be a force for stimulating transformational change in a system, there are legitimate concerns that its focus on identifying the positives within a system or organisation could crowd-out negative experiences, particularly from marginalised communities, and contribute towards organisational inertia. In particular, there is a question about how AI can operate where a system or service is manifestly failing to do what it is set up for. The case studies from PCC demonstrate that this need not be the case - that AI can identify dissonance as a way of positively embracing the need and appetite for change. This raises two questions. First, what is it with the AI approach of PCC that has enabled them to use it for transformation and second, in what sense is this approach still AI?
Regarding the first question, our experience suggests there are several factors arising from PCC’s approach that could help facilitate using AI for transformational change.
First, it is important to choose the right “system” to appreciate. In the case of the child obesity case study, the “system” participants were being asked to appreciate was not the Council’s conventional support for child obesity but their own family relationships and the provision of social support more generally. The fact that participants appreciated different things (e.g., non-stigmatising relationships) to what practitioners may have been expecting revealed a dissonance which could be translated into a call for action. In the case of smoking cessation, the “system” being appreciated was also not the existing smoking cessation support service (which was not used by the participants), but a pilot project that appeared to be having successful engagement. If AI is seen as more expansive in terms of what system is being appreciated and enquired about then there could be more emancipative and transformational opportunities. Of-course this does raise questions as to who decides on the “system” or the boundaries of the “system” to appreciate. This is why the openness of the approach is so critical because the process of AI itself can and needs to enable participants to implicitly influence the way interviewers and policy-makers perceive the boundaries of a system.
Second, it is critical to ensure that the AI process is as inclusive as possible so that a range of voices, including those who may often be marginalised, are involved in the appreciation. PCC is not the first organisation to use AI with ‘service users’/’marginalised communities’ as opposed to organisational members/staff and stakeholders but involving such groups in the process has certainly been critical to initiating change in the system.
Third, the practitioners and policymakers who have a role in the decisions who continually recreate the system should be involved in the process themselves, either through undertaking AI interviews themselves or at the very least being involved in the sensemaking and storytelling. While they were not professional researchers themselves, Public Health practitioners were all involved in collecting the AI above while policymakers and commissioners took part in the reading of the narratives in the first person, spreading appreciative understanding across the system. This way, even practitioners who are emotionally and professionally invested in a particular way of working can, through the development of empathy, and the creation of dissonance, come to understand the need for system change. As one of the authors of the paper has stated AI ‘is the fuel and sensemaking is the engine for systemic change.’ The specific area of sensemaking will be the topic of a future paper.
This aspect of AI has also helped to break down the gap between research and practice, by demonstrating to practitioners the value of engaging in research. In recognition of the importance of research, the Council recently successfully worked with the University of Plymouth and voluntary and community sector partners to secure a Health Determinants Research Collaboration (HDRC) award from the NIHR. The Plymouth HDRC will build upon the work of the Council in bridging the research-practice divide by establishing what Hesselgreaves et al. (2021) might describe as a ‘learning partner’ relationship, using the embedded researcher model. The previous AI work discussed above, and the staff members it has engaged, has already provided a valuable basis on which to develop this partnership. This also involves developing a more robust ethical framework and a resource bank for the use of AI. While ethical considerations (e.g. protecting anonymity) mean it has not been possible to share the actual narratives from the AI exercises in Table 1 more widely, broader case studies have and are being developed through the Plymouth HDRC.
These points also help with the second question, noted above, about whether the approach that PCC has taken really could be considered AI or whether another term should be used. Like Grant and Humphres’ (2006) expanded definition of appreciation, having a broader view of the “system” being appreciated could suggest that PCC’s approach is a form of AI. However, there are aspects of the approach, including the openness and informality of some of the interviews which distinguish PCC’s work from the conventional AI approach. To reflect this, the Plymouth HDRC project has started to use the term “open appreciative enquiry” with an emphasis on the “e” in “enquiry” the British-English spelling for an informal inquiry. This allows for the less formal, more flexible way in which AI is applied by the Council and intentionally builds in the variance of approach depending on context.
Further work is needed to fully define how “open appreciative enquiry” is different to conventional AI, but one way to start would be to amend Cooperrider and Srivastva’s (1987) original principles so they fit within the ethos of open appreciative enquiry. The below provides an initial starting point for discussion, with the italics emphasising the specific features defining open appreciative enquiry. Such an approach can be used exploratively at the beginning of experimentation, or evaluatively at any stage of experimentation: • The research begins with appreciation in the sense that the research looks to identify and explain the “life giving” elements of the participant’s “system,” but how that system is defined is understood by the participant not the researcher. • The research is applicable – ‘used, applied and thereby validated in action’ and this is demonstrated by the involvement of practitioners and policymakers in the process, either at the data collection and/or sensemaking stages. • It should be provocative not only in the sense that the interviewees are provoked into shaping the social world through their own moral values and imaginative ideas, but also in the sense that the researchers and practitioners are provoked into engaging with these moral values and appreciating the dissonance that may exist between these values and those of the formal organisation or system which is involved. • It should involve a collaborative, human-to-human, and, to the extent it is possible, non-hierarchical relationship between the researcher/interviewer, the policymakers and the participants.
Conclusion
As shown above, while AI has become an increasingly popular means of facilitating systemic change, its emphasis on the positive has brought legitimate concerns regarding the potential suppression of negative discourse. Informed by HLS, together with an appreciation of dissonance, PCC’s more open, compassionate, variable and informal approach, provides an example of how AI can be utilised to bring about substantive positive change even where the original context is one of considerable systemic failure.
Footnotes
Acknowledgements
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the National Institute for Health and Care Research (NIHR) Plymouth Health Determinants Research Collaboration [grant number 151310] with support from the NIHR Applied Research Collaboration – South West Peninsula (PenARC) [grant number 200167]. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.