
Abstract
Long-lasting, excessive stress exposure can have serious health consequences and consequently, to identify potentially harmful consequences, it is important to develop self-report measures of long-lasting stress in everyday life. The complexity of long-lasting excessive stress also raises questions about the efficacy of widely used single-item measures to capture such harmful stress. This study examines the psychometric quality and validity of a brief eight-item scale, measuring long-lasting stress symptoms. Using data from a nationally representative sample, comprising 15,046 working individuals from the 2014 Swedish Longitudinal Occupational Survey of Health (SLOSH), the findings suggest retaining six of the original eight items, loading on two latent factors: ‘long-lasting perceived stress’ and ‘long-lasting emotional stress’. The high correlation between the two factors suggests the potential for a unified measure to address specific research objectives. The subscales demonstrate concurrent validity with well-established stress-related measures. A single-item measure of perceived stress (‘I have days when I feel stressed all the time’) also correlated with the stress-related measures, although the correlation coefficients were slightly weaker.
Introduction
Prolonged stress – experienced during a large part of the day over more than a month – can severely impact daily life, well-being and perceived job quality, and may ultimately be detrimental to health (McEwen, 1998; Petrowski et al., 2018). Long-lasting stress, often referred to as chronic stress, can be characterized by constant stress activation along with feelings of persistent pressure and overload, sustained over a longer period (Wheaton, 1997). This type of extended stress response has been found to predict cardiovascular disease, depression, long-term sickness absence, disturbed sleep and also work-related outcomes (Duchaine et al., 2020; Kivimäki and Steptoe, 2018; Niedhammer et al., 2021; Sverke et al., 2017). Since excessive and prolonged stress can be harmful, it is important to employ methods that provide accurate and reliable estimates of long-lasting stress. However, most of the survey instruments that measure long-lasting and chronic stress focus on causes of stress (stressors as e.g., life events and occupational stress) rather than the perception of stress. Moreover, these scales are often lengthy and time consuming to answer and their psychometric properties are sometimes unknown or poorly documented (Petrowski et al., 2018; Wheaton, 1997). Accurately assessing perceived long-lasting stress is crucial both for research aiming at understanding the aetiology of stress and for evaluating interventions aimed at reducing it. Therefore, the overall aim of this study is to investigate the psychometric quality of a brief long-lasting stress scale based on symptoms of stress, and examine its correlation with established measures of work stress exposure and indicators of health impairment.
Theoretical framework
The key components of the stress concept
In psychological studies stress is often described as a process that includes two core components, namely: the stressor and the subjective stress experience (Kilby et al., 2022; Kopp et al., 2010). The stressor component refers to a challenging or threatening stimuli or situation that initiates the stress process. The relevance of measuring causes of stress (stressors) is based on the assumption that increased exposure should predict a stress response and adverse long-term consequences of stress, e.g. in relation to health. Also, the stress exposure approach assumes that the stressor generates equal amounts of stress reactions for all individuals (Cohen et al., 2016). Given that individuals differ in how they evaluate their surroundings and their own capacities, this notion does not fit with the theoretical assumption that the cognitive evaluation of the stressor is a key component in stress theory, where the subjective stress experience refers to individuals’ evaluations and appraisals of the stressor, and the emotional symptoms associated with the stressor (Lazarus and Folkman, 1984). If the stressor is perceived as negative or threatening, individuals would find the situation stressful. However, if the stressor is perceived as neutral or a challenge the stimuli might not evoke the same stress reactions. Also, given the situation is perceived as stressful, the individual’s reaction depends on the secondary appraisal, which involves evaluation of available possible coping strategies. Inadequate coping behaviours can exacerbate the stress response. The balance between the stressor, the appraisal of the stressor and the resources to cope with the stressor constitute the key factors of the transactional theory of stress (Lazarus and Folkman, 1984). Consequently, a direct ‘stressor–adverse consequences’ association could either underestimate or overestimate the overall consequences of stress. In addition, it has been suggested that measures of perceived stress mirror stress severity better than measures that assess stress exposure, and therefore should be a better predictor of health outcomes (Shields et al., 2023).
Short-term or acute stress responses are regarded as an adaptive process that prepares the individual to handle challenging, demanding or threatening situations and circumstances by increased activation of the biological stress system (McEwen, 1998). Short-term stress is a normal biological response that enhances cognitive and physical performance, and challenging situations are normally not perceived as highly stressful and will not be associated with poor health (Dhabhar, 2018). However, if a stressful situation is frequently repeated and there is no successful return to equilibrium the increased biological stress activation can be prolonged, which can lead to long-lasting or chronic stress, maladaptive biological responses and finally health risks (McEwen, 1998).
Thus, long-lasting stress can be defined as repeated activation of the stress response, accompanied by negative subjective experiences and/or insufficient resources to manage the stressor over a sustained period – preventing a return to the baseline physiological and psychological functioning. While we are aware that in research literature the term chronic stress is more common, we prefer long-lasting stress to emphasize that the condition is not necessarily permanent, but may be resolved if the stressor is removed, for example following a successful intervention. There is no consensus of how long a period must last to be considered as long-lasting or chronic. The assessment periods in previous research range from one year to the past four weeks (Petrowski et al., 2019). A one-year assessment period is probably too long and the estimates might be biased because of poor recall. However, a four-week period might be too short and some people may habituate to a temporary increase in perceived stress (Petrowski et al., 2018). If habituation occurs perceived stress may not be associated with impaired health. According to the Trier Inventory of Chronic Stress, long-lasting stress should cover a time period of three months (Petrowski et al., 2018).
In conclusion, precise assessment of long-lasting stress requires measurements of stress symptoms, which are linked to the appraisal process and the emotional responses associated with the stressor. These measurements can be complemented with measurements of stressors when the aim is to understand the cause of the stress experience.
A brief overview over methods to measure long-lasting stress
There are many scales that can be used to measure stress, but most of the instruments focus on relatively short-term stress, up to a maximum of four weeks, or the severity of stress. Kopp et al. (2010) reviewed 16 instruments to measure stress in epidemiological research, of which several assessed chronic or long-lasting stress. The instruments measured stressors such as major life events, work, marital and social stress, and psychological stress experience. A large majority of the instruments took at least 10 minutes to complete, which makes them unfeasible for large-scale epidemiological research and occupational health studies. Several of the measures included components relevant to the stress experience, such as the Perceived Stress Scale (PSS; Cohen et al., 1983). The PSS is the most widely used measure of psychosocial stress in terms of the stress experience. It emphasizes the appraisal of stressful situations and assesses whether the stressor is predictable and controllable, and whether typical stress symptoms (upset, nervous, anger) are experienced. The PSS has been translated into many languages and shows good psychometric properties. For example, a Swedish version of the PSS showed good internal reliability (Cronbach’s alpha 0.84) and good construct validity demonstrated through high correlations (range: 0.57–0.71) with measures of mental health (Nordin and Nordin, 2013). The PSS is also brief (time to complete the instrument is estimated at five minutes) and the psychometric properties are adequate. However, the time period included only covers four weeks, which is considerably shorter than the assessment period of three months suggested by the Trier Inventory for Chronic Stress.
The Trier Inventory for Chronic Stress (TICS) was psychometrically evaluated in several age groups. The TICS measures chronic stress over a three-month period (Petrowski et al., 2018). It is extensive and includes 57 items, and the scale comprises nine subscales, for example work overload, social overload, excessive demands at work and chronic worrying. Thus, the scale includes items that measure stressors as well as typical stress symptoms. A brief nine-item version of the instrument has been developed and the correlation with the full-length version was very high (r = 0.94), which suggests that the short version can be recommended in epidemiological studies (Petrowski et al., 2019).
There are also stress measures that mainly includes clinical symptoms of stress, for example the Karolinska Exhaustion Disorder Scale (KEDS; Besèr et al., 2014) and the Shirom–Melamed Burnout Questionnaire (SMBQ; Almén and Jansson, 2023; Sundström et al., 2023). These instruments have been validated with good results using data from Sweden. However, both KEDS and SMBQ are intended to be used mainly in clinical settings and can be suboptimal in non-clinical groups. For example, the KEDS measures the clinical symptoms of exhaustion disorder, which include items related to poor sleep, cognitive complaints and hypersensitivity to sensory impressions. These can be consequences of severe stress, but may not be typical stress symptoms for non-clinical, working individuals with elevated stress levels.
Finally, a few single-item measures assess perceived stress. It has been debated whether stress can be meaningfully measured using a single item, given that stress is assumed to be a multidimensional construct. Single-item measures are not recommended for multidimensional, complex constructs and may suffer from poor reliability and validity (Matthews et al., 2022). On the other hand, the benefits of single-item measures include high face validity, less item repetition and lower respondent burden (Allen et al., 2022), making single-item measures especially valuable for studies with limited space for longer instruments. The debate on single-item measures in psychology has been recently revived and a recent editorial concluded that single-item measures often are as valid and reliable as their counterparts based on multiple-item measures (Allen et al., 2022).
A study by Littman et al. (2006) evaluated the reliability and validity of two single-item measures and found promising results – their psychometric properties were comparable to those of multi-item stress instruments such as the PSS. Gilbert and Kelloway (2014) also observed that single-item measures of job stressors showed good psychometric quality. Similar findings were observed in three more recent studies (Arapovic-Johansson et al., 2017; Elo et al., 2003; Matthews et al., 2022), indicating that single items can be sufficient to measure stress experiences. However, the measure developed by Elo et al. (2003) includes a stress definition emphasizing the negative consequences of stress, such as sleep problems, which may lead to biased findings when investigating associations between single items and health impairment. Hence, it is important to evaluate whether a more neutral question with high face validity, such as ‘Do you feel stressed?’, can assess perceived stress equally well as a multiple-item measure.
Validation of the long-lasting stress measure
Validation studies of chronic and long-lasting stress have usually used indicators of stressors and health impairment as criteria for construct validity. To the best of our knowledge, the psychometric studies of the TICS have not evaluated construct validity, i.e. the association with independent measures known to be related to long-lasting stress, such as work stressors, has not been tested. However, the PSS typically shows moderate to strong correlations with various indicators of psychological distress, such as symptoms of anxiety, depression and exhaustion (Cohen et al., 1983; Kopp et al., 2010; Nordin and Nordin, 2013). In contrast, its associations with objective stressors such as life events are usually weaker (Cohen et al., 1983; Kopp et al., 2010). This pattern likely reflects the fact that perceived stress is closely linked to the appraisal process; not all individuals perceive a stressor in the same way.
Aim of the study
There are several validated instruments that measure core components of stress. However, psychometric studies evaluating instruments measuring experience of long-lasting stress symptoms developed for non-clinical groups are rare. Hence, the Long-Lasting Stress Scale (LLSS) used in the Swedish Longitudinal Occupational Survey of Health (SLOSH), which is evaluated in the current study, includes symptoms of long-term perceived stress over a three-month period and provides a measure of the total stress load after exposure to both work and non-work stressors. The intention with the LLSS was to develop a brief scale based on items measuring symptoms of stress, designed for use in both working and non-working populations.
A previous study using three of the questions in the LLSS to create a generic stress index showed promising results, as demonstrated by a strong test–retest correlation (r = 0.61, p < 0.001) and a prospective association with sleep problems (Åkerstedt et al., 2015). However, the study did not include psychometric evaluation involving factor analysis.
In sum, the aim of the present study is to examine the validity and dimensionality of the LLSS in a large sample initially representative of the working Swedish population. The dimensions of the instrument are tested using exploratory and confirmatory factor analysis. A secondary aim was to evaluate the validity of a single item with high face validity of long-lasting stress.
The construct validity of the LLSS is assessed through correlations with two well-established measures of work stress, i.e. job demands and overcommitment (defined as the inability to withdraw from work), and two validated measures of health impairment, namely emotional exhaustion (one of the core components of burnout syndrome) and disturbed sleep. The use of sleep as validation criterion is justified by a systematic review showing that several psychosocial work stressors (e.g. job demands) predict sleep problems (Linton et al., 2015), and elevated biological activation (similar to a prolonged stress response) is a core characteristic for the clinical diagnosis of insomnia (Benjamins et al., 2017).
The evaluation of the single item, phrased as ‘I have days when I feel stressed all the time’ (which is one of the items of the LLSS), is assessed through the correlation with the multiple-item LLSS, as well as the previously mentioned indicators of construct validity.
Data and methods
Sample of participants
The data were derived from SLOSH, which is approximately representative of the Swedish working population. SLOSH began in 2006 following participants of the 2003 Swedish Work Environment Survey (SWES). The present study used data from the fifth wave of SLOSH, conducted in 2014, and builds on the respondents of SWES 2003–2011. The details of the study design have been published elsewhere (Magnusson Hanson et al., 2018). To examine the dimensionality and validity of the LLSS, a total sample of 15,046 working individuals out of a total sample of 21,315 participants with no missing data on any of the LLSS items was used; 57% were women and the mean age of respondents was 51 years.
The Long-Lasting Stress Scale (LLSS)
The intention with the LLSS was to develop a brief scale based on items measuring symptoms of long-lasting perceived stress, to be used primarily in non-clinical groups. The scale should be easy to administer, have a low cognitive load, and should not be linked to specific stressors, and focus on general stress experiences rather than specific stressors or their consequences. Following the Trier Inventory of Chronic Stress (Petrowski et al., 2018), it was decided that LLSS should cover a time period of three months.
The construction of items built on the assumption that long-lasting stress can be characterized by days of constant stress activation, and feelings of persistent pressure and overload (Stanton et al., 2001). Moreover, it is important that days of constant stress activation occur over several months to be classified as long-lasting stress. Other examples of symptoms that indicate long-lasting stress are impaired recovery, that is, not feeling well-rested after days with no stress exposure and having difficulties to relax. Furthermore, long-lasting and chronic stress is often characterized by persistent negative emotions such as having worrying thoughts and feeling tense (Petrowski et al., 2018). Finally, it was decided to have one item with high face validity, i.e. feeling stressed all the time. This item can also be evaluated as a single item of long-lasting stress. Also, it should be possible to respond to the items regardless of whether the respondent is working or not. Finally, the overlap with scales measuring clinical stress disorders, such as exhaustion syndrome and burnout, should be as low as possible.
The LLSS originally included eight items, as presented in Table S1 (supplementary online Appendix). Before the list of items, respondents were given an instruction. This was phrased as follows: ‘Read each statement and mark the answer that comes closest to how you have felt in the last three months.’ Each item is measured on a Likert-scale with the response alternatives ‘not at all’ (scored as 1), ‘sometimes’ (2), ‘quite often’ (3) and ‘almost always’ (4). Item number 8 (‘I have days when I feel stressed all the time’) was used as a single-item measure.
Measures of work stressors and stress-related health impairment
Emotional exhaustion, overcommitment at work, sleep problems and psychological job demands are known correlates of the overall construct of stress, and are used here to assess the construct validity of the true score of the extracted factors from the stress scale being studied. All the variables are measured on Likert-scales, and are operationalized as means of the items included in each of the variables. Table S2 (online Appendix) presents the distributions of mean scores for each stress-related correlate.
Sleep problems were measured with the disturbed sleep index (Åkerstedt et al., 2015). The index is based on four questions and the participants reported whether they experienced difficulty falling asleep, repeated awakenings, premature awakening with difficulties getting back to sleep and restless sleep, using a six-point scale ranging from ‘never’ (1) to ‘always/five times or more a week’ (6). Emotional fatigue was measured with six questions from the Shirom–Melamed Burnout Questionnaire (Melamed et al., 1992). All items are answered on a seven-point scale ranging from ‘almost never’ (1) to ‘almost always’ (7). Overcommitment was measured by a short version of the Effort–Reward Imbalance Questionnaire (Leineweber et al., 2010). Items are answered on a four-point Likert-scale ranging from ‘agree totally’ (1) to ‘do not agree at all’ (4). Job demands were measured using a subscale of the Swedish Demand-Control-Support Questionnaire (Theorell et al., 1988) and validated on the Swedish Longitudinal Occupational Survey of Health (Chungkham et al., 2013). Items are answered on a Likert-scale ranging from ‘often’ (1) to ‘never/almost never’ (4). The time frame for the sleep questions was three months, whereas there was no time frame for the other variables.
Statistical analyses
As the factor structure of the LLSS questionnaire has not yet been established, the present study used exploratory factor analysis (EFA) to understand the dimensionality of the instrument. Selecting the optimal number of factors to retain is crucial in EFA (Nichols and Edlund, 2023). We adopted parallel analysis (PA) (Horn, 1965) to determine the optimal number of factors in the initial EFA along with several fit indices and theoretical considerations. Parallel analysis (Horn, 1965) is a widely recommended technique for determining the optimal number of factors to retain in EFA. This method compares the eigenvalues obtained from the actual dataset with those generated from randomly simulated data with the same sample size and number of variables. Factors are retained if their eigenvalues exceed those of the simulated data, as they indicate meaningful variance rather than random noise. Nichols and Edlund (2023) provides a detailed account of a comparative view of the approaches.
Data suitability and sampling adequacy to conduct factor analysis was checked by the Kaiser–Meyer–Olkin (KMO) (Kaiser, 1974) value and Bartlett’s test of sphericity (Bartlett, 1951). The goodness of fit was evaluated through several fit indices (Brown, 2015). Acceptable model fit was defined by standardized root mean square residual (SRMR) values ⩽ 0.08 (Ogasawara, 2001), root mean square error of approximation (RMSEA) values < 0.05 (McNeish and Wolf, 2021) and with comparative fit index (CFI) and Tucker–Lewis index (TLI) values ⩾ 0.95 (Bentler, 1990; Tucker and Lewis, 1973). Once a plausible factor structure was obtained, a confirmatory factor analysis (CFA) was performed to confirm the factor structure in EFA using structural equation modelling. To achieve this, the whole sample was divided into two subsamples comprising 70% (subsample A) and 30% (subsample B) of the total cases. Subsample A was used for exploring the model based on EFA using oblimin rotation for correlated factors in psych package (Revelle, 2024) in R (R Core Team, 2024), with subsample B used for the CFA validation of the model suggested in the EFA. The EFA on subsample A was followed by CFA to assess the acceptability of factor structure and also for possible model modification. The internal consistencies of the scales are evaluated by calculating Cronbach’s alpha coefficients (Cronbach, 1951). In addition to Cronbach’s alpha, the composite reliability (CR) and average variance extracted (AVE) were calculated, as Cronbach’s alpha underestimates the reliability (Trizano-Hermosilla and Alvarado, 2016; Zumbo et al., 2007). The parameters of the CFA were estimated by the method of weighted least squares adjusted for mean and variance (WLSMV) to account for the ordinal response structure in items (for details see DiStefano and Morgan, 2014) using lavaan (Rosseel, 2012) in R (R Core Team, 2024).
Construct validity analysis
In the final stage of analysis, we assessed the construct validity of the established factor structure through convergent and discriminant validity to check how well the observed variables represent the underlying latent constructs. Convergent validity ensures that latent constructs measuring the same factor are theoretically related, while discriminant validity observes the degree to which they remain discriminated. The convergent validity is assessed through the standardized factor loadings (>= 0.70), average variance extracted (AVE >= 0.50) and composite reliability (CR >= 0.70) (Fornell and Larcker, 1981; McDonald, 1999). The discriminant validity is evaluated through the Fornell–Larcker criterion (Fornell and Larcker, 1981) and the heterotrait-monotrait (HTMT) criterion (Henseler et al., 2015). Finally, we tested how well the factor structure correlated with two stress exposure variables (stressor) commonly used in psychological research, and two indicators related to health (for details please see above). As the LLSS items measure feelings of overload and pressure, which are known to be associated with mental health, we hypothesize that LLSS scores would show stronger correlations with indicators of health impairment – emotional exhaustion and disturbed sleep – than with work stressors (job demands and overcommitment). To this end, correlation coefficients are calculated between the mean scores of each of four stress-related variables and each of factor scores obtained from the CFA.
Results
Distribution of items
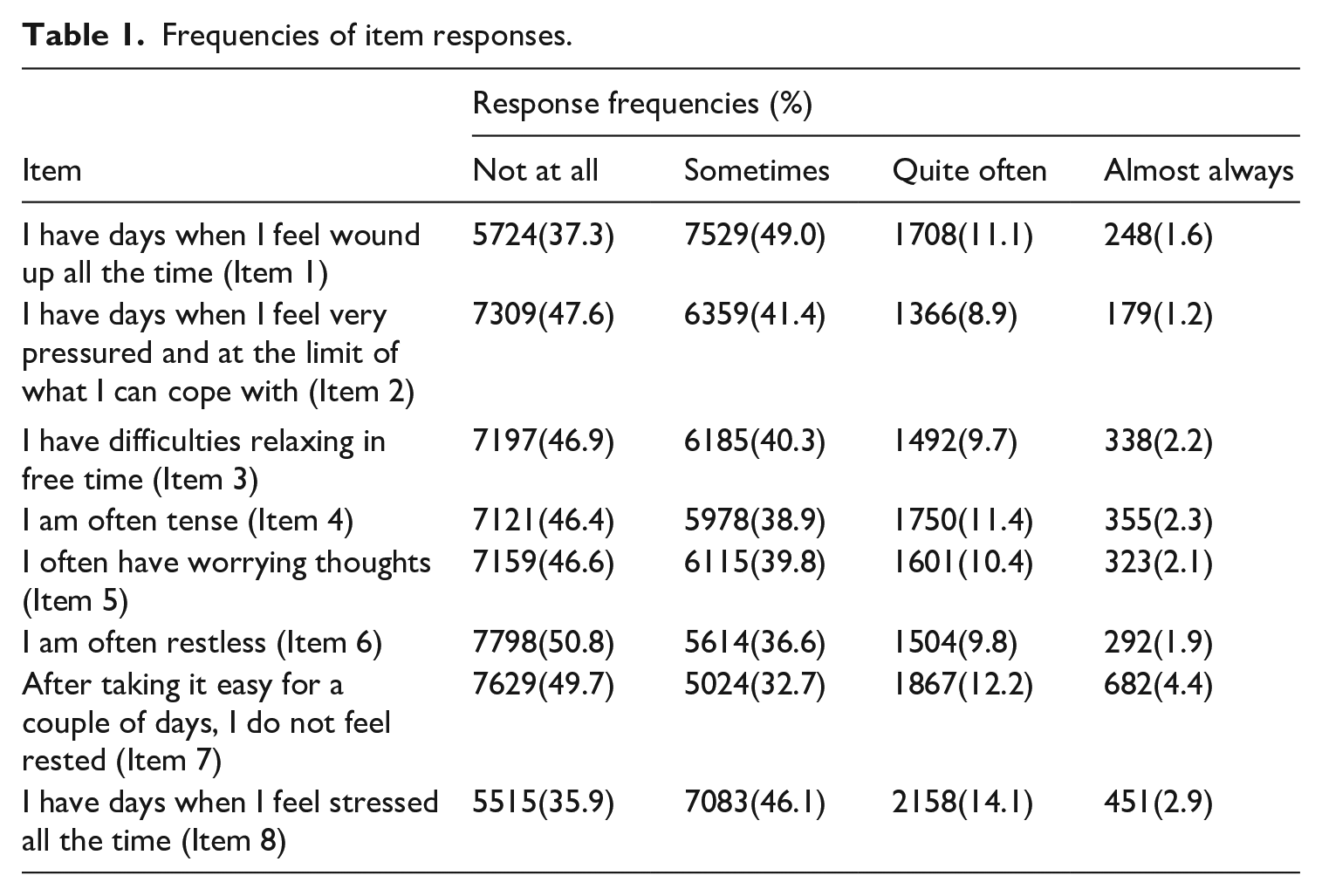
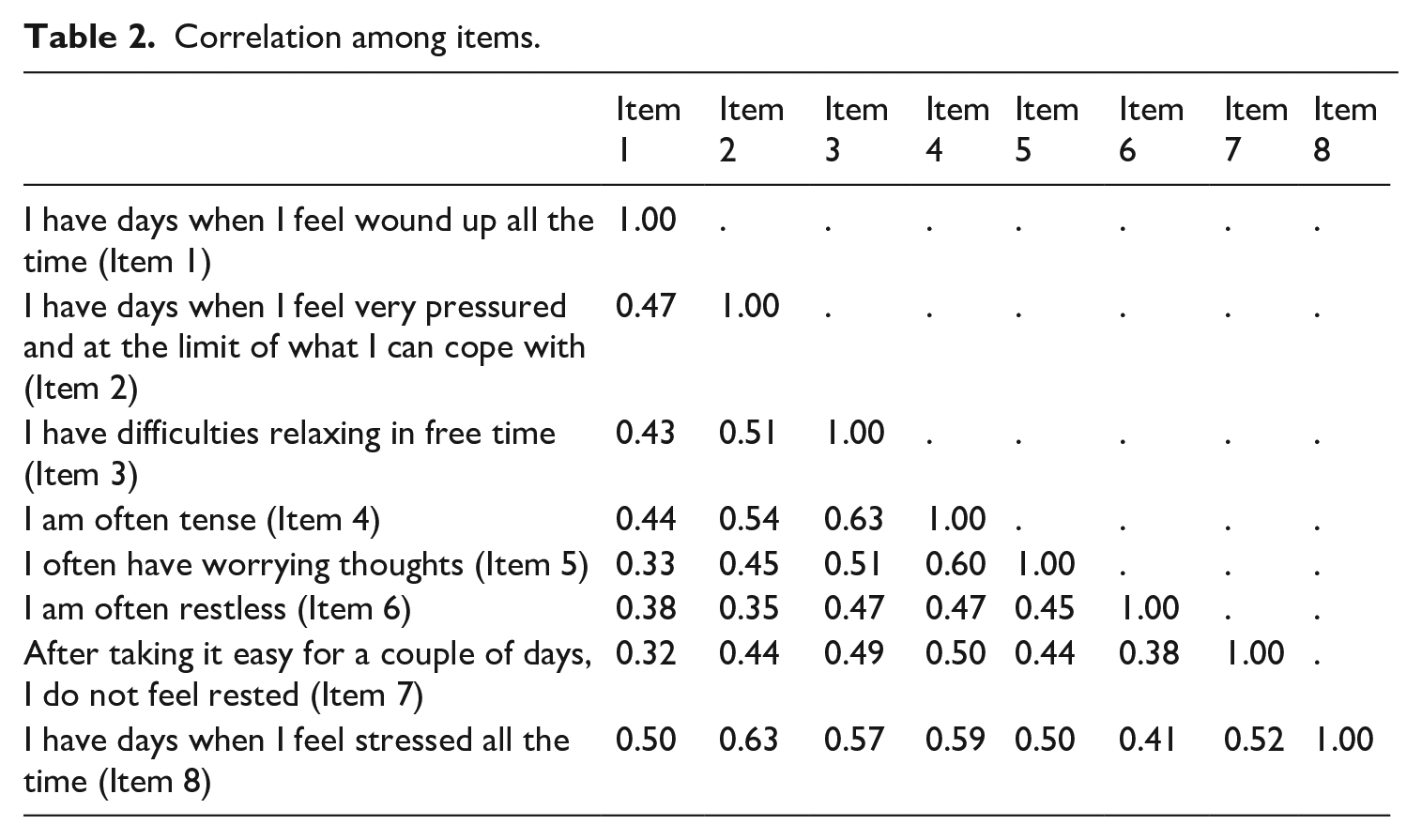
As can be seen from Table 1, in regard to the LLSS the most common response option was ‘not at all’ for all of the items, demonstrating skewness in each of the distribution of response options. This indicates that the normal distribution is unsuitable in structural equation modelling of factor structure in later stages of the analyses. The pairwise polychoric correlations among items show a moderate strength ranging from a low of 0.32 to a high of 0.64 (Table 2).
Frequencies of item responses.
Correlation among items.
Exploratory and confirmatory factor analyses
The KMO statistic of 0.917 suggests that factor extraction was suitable for the data we used. Furthermore, Bartlett’s test of sphericity (χ2[28] = 47149.04, p < 0.001) also confirmed the adequacy of data for factor extraction. By adopting the parallel analysis on the full eight items, the scree plot in Figure S1 (online Appendix) suggested a three-factor solution. The results of the analysis from the EFA are shown in Table S3 (online Appendix). The results suggested a cross-loading of item 7 on factor 1 and factor 2 with a small communality of 0.403 (< 0.50). So, in order to have a purer factor structure, we removed item 7 and ran parallel analysis. The scree plot, as shown in Figure S2 (online Appendix), still suggested a three-factor structure. The results of the three-factor analysis without item 7 are shown in Table 3. It can be seen that items 1, 2 and 8 constitute factor 1, items 3, 4 and 5 constitute factor 2, and item 6, factor 3. However, we find also a slight cross-loading of item 6 on both factor 2 and factor 3 and the communality is just 0.50. Thus, in the next step we removed item 6 and performed parallel analysis on the remaining six items. The scree plot (Figure S3, online Appendix) clearly suggested a two-factor solution, and hence we explored a two-factor EFA. The results are shown in Table 3. The second block of Table 3 provides the estimated parameters along with several fit indices. The results suggested a clear two-factor solution with items 1, 2 and 8 forming factor 1 and items 3, 4 and 5 forming factor 2. Fit indices are good, and the communalities are all above 50% except for item 1, which is only 42%. To gain better understanding of the factor structure, we tested a two-factor solution excluding item 1 (results not shown). The model without item 1 (even though its communality is slightly less than 50%) provides nearly perfect fit indices, which hints for a possible overfitting. The model may lack generalizability and could be capturing noise rather than the true structure. Therefore, we decided to retain the two-factor solution with six items. The first factor is formed by item 1, item 2 and item 8, and seems to measure ‘long-lasting perceived stress’. The standardized factor loadings for the factor ranges between 0.667 and 0.724. Item 3, item 4 and item 5 formed the second factor – ‘long-lasting emotional stress’. The factor loadings for the second factor are in the range of 0.580–0.840. The established two-factor EFA model is fitted on the same subsample A under the CFA using the structural equation modelling (SEM) framework. The standardized factor loadings along with measurement errors from the two-factor CFA model are shown in Figure 1. We found a high correlation of 0.88 between the two factors (see Figure 1). All the model fit indices have shown a good model fit criterion. The final two-factor CFA is again validated on subsample B. The results show very similar estimates and good model fit indices (CFI = 0.997, TLI = 0.994, RMSEA = 0.059 (90%CI: 0.058, 0.068), SRMR = 0.018), the standardized factor loadings for item 1, item 2 and item 8 on factor 1 are 0.711, 0.866 and 0.907. Factor loadings for item 3, item 4 and item 5 on factor 2 are 0.858, 0.915 and 0.784. We therefore regarded the two-factor EFA model as validated and accepted it as the final model.
Standardized factor loadings and fit measures from competing exploratory factor models.
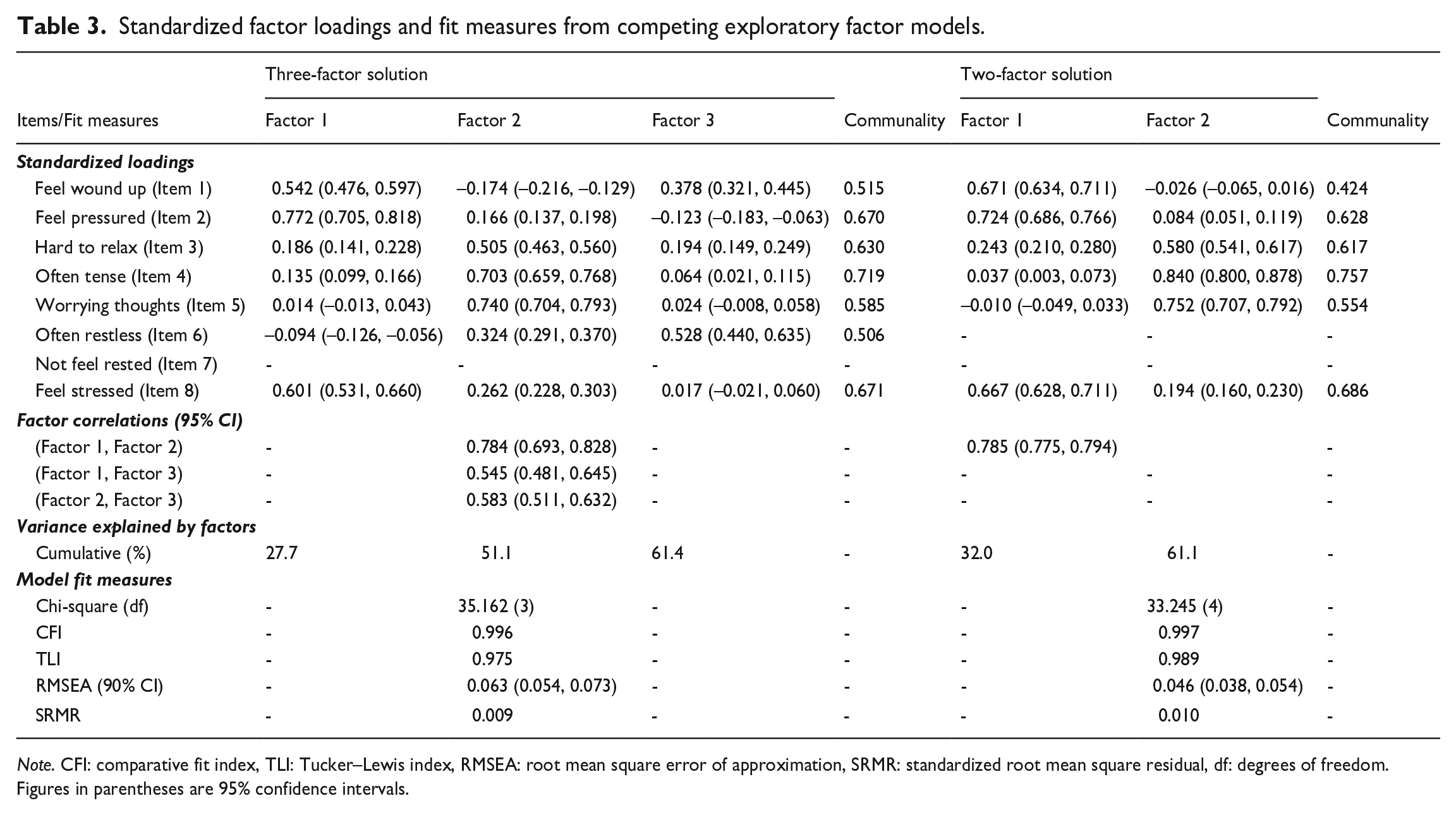
Note. CFI: comparative fit index, TLI: Tucker–Lewis index, RMSEA: root mean square error of approximation, SRMR: standardized root mean square residual, df: degrees of freedom. Figures in parentheses are 95% confidence intervals.
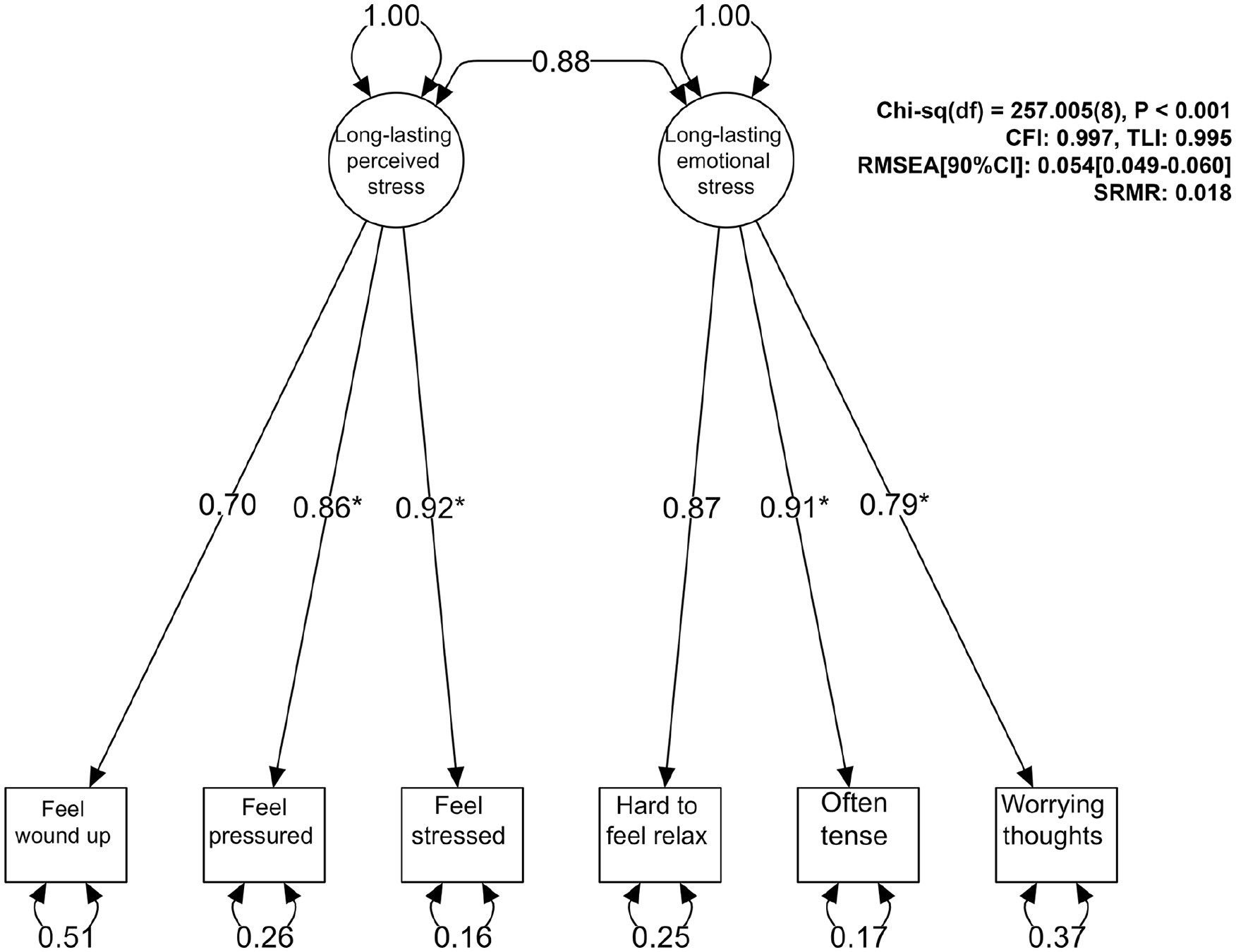
Two-factor confirmatory factor model.
Convergent and discriminant validity
The ‘long-lasting perceived stress’ and ‘long-lasting emotional stress’ show AVE of 0.68 (95% CI: 0.67–0.70), 0.74 (95% CI: 0.72–0.75) and CR of 0.86 (95% CI: 0.85–0.87), 0.89 (95% CI: 0.87–0.90), respectively, which are well above the thresholds, indicating strong convergent validity for the two factors. The Cronbach’s alpha coefficients for the ‘long-lasting perceived stress’ and ‘long-lasting emotional stress’ are 0.80 and 0.84, respectively. This indicates that both factors have good internal consistency in the population. The discriminant validity of the two factors is evaluated by two well-known criteria, Fornell–Larcker (Fornell and Larcker, 1981) and heterotrait-monotrait (HTMT) (Henseler et al., 2015). However, the criteria should be evaluated on a continuum rather than a binary decision, i.e. discriminated or not (Henseler et al., 2015). The Fornell–Larcker criterion is evaluated by comparing the AVE to the square of the correlation between the two factors. The square of the factors’ correlation is 0.770, which is above the respective AVEs of the factors (0.683, 0.742). The HTMT value is calculated as 0.872 (95% CI: 0.857–0.883), which is above 0.85, but less than 0.90. According to the Fornell–Larcker criterion this indicates a lack of complete discrimination. However, according to the HTMT criterion, there is moderate discrimination between the two factors (Henseler et al., 2015). Therefore, we may conclude that a moderate discriminant validity is established between the two latent factors.
Table S4 (online Appendix) presents the estimated correlation coefficients between the mean scores of each stress-related variable and factor scores. We can see that there is a strong positive relationship between the two factors of LLSS and emotional exhaustion (correlation coefficients: 0.65, 0.65) and sleep problems (correlation coefficients: 0.46, 0.50), respectively. The relationship between the factor scores and job demands is lower (correlation coefficients: 0.31, 0.27), while correlations with overcommitment are moderate (correlation coefficients: 0.40, 0.39). Finally, we tested the suggested single-item measure (item 8) in relation to the stressor and health impairment indicators. The results demonstrated significant correlations with the stressors. We found a high significant correlation between the single item and emotional exhaustion (0.57), with sleep problems (0.40), with overcommitment (0.35) and with job demands (0.27) (Table S4, online Appendix). The correlation between the single-item measure and the factors was 0.91 for factor 1 and 0.80 for factor 2.
Discussion
The present study aimed to investigate the psychometric properties of the Long-Lasting Stress Scale (LLSS) in a large and representative sample of the Swedish working population. Additionally, it aimed to examine the association of this scale with established measures of psychological work demands, emotional exhaustion (a core symptom of clinical stress disorders) and disturbed sleep.
Our study shows that the LLSS is a valid and reliable measure to measure stress symptoms in a relatively comprehensive way. This means that the findings support the utility of this scale in epidemiological and psychological research and highlight its potential for both research and practical applications in assessing stress levels in the working population. It thus provides researchers and practitioners with a valuable tool for monitoring stress trends and evaluating interventions aimed at reducing stress and promoting well-being. Furthermore, a single-item measure (‘I have days when I feel stressed all the time’, item 8) also showed robust associations with the well-established measures of work stress, emotional stress and disturbed sleep, although the strength of the associations was slightly weaker.
Our findings reveal a two-factor structure of the LLSS, comprising long-lasting perceived stress and long-lasting emotional stress. Both factors demonstrated good model fit and satisfactory psychometric properties. The first factor, long-lasting perceived stress, focuses on the physical ramifications of a stress experience (strain and symptoms of intense pressure), while the second factor, sustained emotional stress, focuses on symptoms of distress, especially anxiety and apprehension. These factors can be used as two different measures of stress or as a single factor representing the multidimensional concept ‘stress’.
There is no clear theoretical ground for two independent measures of long-lasting stress symptoms and both factors are highly correlated. One explanation for the two-factor solution might relate to the way items were phrased. The items of the first factor (long-lasting perceived stress) start with the wording ‘I have days’, whereas the wording of the items in the second factor is ‘I am’, ‘I often’ and ‘I find it’. However, the strong correlation between the factors suggests that the way the items were phrased only had a marginal effect on the factor structure. We found a moderate level of discriminant validity of the two factors, which means that it might be possible to use the two factors as one single factor in case the research question targets perceived overall long-lasting stress. The LLSS thus demonstrates some flexibility and its use may depend on the specific research question. For example, the factor ‘long-lasting perceived stress’ would be preferable if the research question examines the relationship between long-lasting stress symptoms and mental health disorders, given the overlap between sustained emotional stress (the second factor) and mental health issues.
The significant associations between the single-item measure, the work stressors, emotional exhaustion and sleep disturbances are consistent with previous research, showing that a simple question about perceived stress can provide reliable information about stress levels in studies where it is not possible to use multiple-item scales (Arapovic-Johansson et al., 2017; Elo et al., 2003; Littman et al., 2006). At the same time, the strength of the associations is weaker compared to when all items are included in the long-term stress measure, suggesting that the measurement of long-lasting stress is more accurate when the full scale is used.
It seems that both subscales are effective in identifying people with high stress level. The correlation coefficients with emotional exhaustion, overcommitment, sleep problems and job demands were very similar for both factors, supporting the construct validity of the subscales. The correlations with emotional exhaustion are substantially higher than those with the other factors, which is consistent with a scale designed to measure potentially harmful long-term stress activation rather than exposure to particular stressors. Similarly, studies using the PSS have also found relatively weak associations with work stressors (Larsen et al., 2023). This is consistent with the notion that the direct association between stressors and the stress response is mediated by the cognitive appraisal of the stressor, as well as resources available to cope with it (Lazarus and Folkman, 1984). Consequently, exposure to a specific stressor will in many situations generate individual differences in the stress reactions (Cohen et al., 2016).
As outlined in the introduction, several questionnaires that measure stress are available. The obtained factors of the LLSS have similarities with the factor structure of the Trier Inventory of Chronic Stress (TICS) scale (Petrowski et al., 2018), even though the TICS is a more extensive scale with 57 items and nine subscales. However, the most commonly used scale is the Perceived Stress Scale (PSS) (Cohen et al., 1983). Compared to the PSS, the LLSS is slightly shorter, has a longer time frame (three months) and focuses on more long-lasting symptoms of persistent stress. Also, while the PSS focuses on feelings of being able to cope with certain events (e.g. ‘How often have you found that you could not cope with all the things that you had to do?’), the LLSS has a clear focus on the core symptoms of perception of stress that can be harmful, such as ‘I have days when I feel wound up all the time’ and ‘I have days when I feel very pressured and at the limit of what I can cope with’. The latter two items, and the statement ‘I have days when I feel stressed every day’, should according to stress theory reflect elevated long-term physiological activation or arousal. If these feelings occur almost every day, they would indicate chronic stress. While the first factor represents long-lasting stress activation, the second factor portrays the inability to shut out worrying thoughts, tension and difficulties relaxing. These items are typical symptoms of anxiety disorders but may also indicate persistent emotional responses caused by exposure to a long-lasting stressor (Chida and Hamer, 2008).
The inclusion of symptoms of anxiety items further enhances the comprehensiveness of the scale, aligning it with contemporary stress theories emphasizing the importance of understanding stress mechanisms apart from the symptoms of stress as such. The items of worrying thoughts, tension and difficulties relaxing have similarities with the concept of insufficient recovery developed by Sonnentag and colleagues (Geurts and Sonnentag, 2006). The factor may indicate problems with two components of insufficient recovery, more precisely poor detachment and inadequate relaxation after stressor exposure. The stress-recovery model proposes that the negative consequences of work stress occur when it is combined with insufficient recovery (Sonnentag, 2018). However, even though the LLSS can provide insight into the importance of relaxation and the ability to decrease activity within the stress system (Sonnentag, 2018), the items of the second factor measuring stress-related anxiety symptoms are too unspecific to assess recovery in detail. For example, the LLSS does not measure relaxation from stress per se but rather the consequences of insufficient stress recovery.
One item, ‘After taking it easy for a couple of days, I do not feel rested’, loaded on both factors and we decided to exclude this item. This item shows elements of impaired recovery (not feeling rested) and inability to relax (not feeling rested after taking it easy), which suggests that the question probably refers to insufficient recovery rather than long-lasting stress.
Building upon a comprehensive theoretical framework of stress, we acknowledge the multi-component characteristics of stress. However, the results also show that the single-item measure can be used as a proxy measure of long-lasting stress, which makes the item useful in large-scale survey studies. While we were able to demonstrate cross-sectional correlations of the LLSS with important outcomes, future research should explore longitudinal associations between stress levels measured by this scale and various health outcomes, further elucidating the impact of stress on overall health and human functioning. Also, further validation of the LLSS through comparison with other stress scales, such as the PSS (Cohen et al., 1983), as well as physiological measures of stress activation (e.g. hair cortisol levels) would be useful. Finally, while this scale makes repeated measures of perceived stress in large samples feasible, further investigations into the accuracy and precision of using the single item to measure long-term changes in long-lasting stress are needed.
Our study also has some limitations. First, the analysis combines all working individuals irrespective of different characteristics. We have not yet tested whether the factor structure can be replicated in different groups (e.g. sex, age groups, working status). In the future, we plan to investigate the measurement invariance of the established factor structure across different groups and time points. Establishing measurement invariance will allow researchers to compare factor scores across groups and over time. Also, while the scale was developed to measures stress regardless of a person’s work status (i.e. being in paid work or not), we limited our validation to working individuals. Further validation including those not in paid work, such as retirees and persons on long-term sick leave, is warranted. Furthermore, it is also likely that the obtained stress dimensions are related to personality traits, as suggested by the moderate correlation with overcommitment, warranting further investigation (Angelini, 2023). Finally, the high correlation between the two factors may suggest some form of common method bias, potentially arising from similar wording in some of the items.
In conclusion, the present study advances the understanding of stress measurement by providing a validated instrument that captures long-lasting perceived stress processes. By incorporating psychometrically sound measures of stress, researchers and practitioners can more effectively assess and address the complex dynamics of stress, complementing the measurement of stress exposure with that of measures of long-term overwhelming stress and associated symptoms.
Supplemental Material
sj-docx-1-eid-10.1177_0143831X251350449 – Supplemental material for The Long-Lasting Stress Scale (LLSS): Psychometric evaluation of a brief stress scale in the SLOSH cohort study
Supplemental material, sj-docx-1-eid-10.1177_0143831X251350449 for The Long-Lasting Stress Scale (LLSS): Psychometric evaluation of a brief stress scale in the SLOSH cohort study by Holendro Singh Chungkham, Constanze Leineweber, Linda Magnusson Hanson, Hugo Westerlund and Göran Kecklund in Economic and Industrial Democracy
Footnotes
Author contribution
HSC: analysed the data, and wrote the first draft of the paper together with GK
CL, LMH, HW and GK: contributed to the planning of the data analysis, interpretation of the data and critical review of the paper
All authors contributed to the design of the study
HW acquired funding for the study
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.