
Abstract
This article examines the identity (re)work undertaken by junior doctors during the junior doctors’ contract dispute of 2015–16 in the National Health Service (NHS). A qualitative, longitudinal approach was used, consisting of 31 interviews with 18 junior doctors across two time periods. Findings show that the junior doctors’ strike represented a major threat to their professional identities, and that the strike action instigated significant identity (re)work for the doctors. Furthermore, findings reveal three overlapping ‘identity threat alleviation’ strategies that were constructed by striking doctors: reluctant acceptance of their weak bargaining power due to their professional identities; a subsequent reattachment to their normative professional values; and a focus on their future careers. This study examines the effects of a ‘white collar’ industrial dispute through the lens of professional identity, showing how medics employ identity (re)work as a resource to help them cope with perceived assaults on their professional identity.
Introduction
The junior doctors’ dispute of 2015–16 was a unique moment in public sector and professional employment relations in the UK, bringing the first withdrawal of emergency care by doctors in the history of the NHS. Public and practitioner opinion was polarised by the action of the junior doctors, and the British Medical Association (BMA) representing them. For example, Park and Murray (2014) are critical of the ethics of strike action for financial gain, which they say conflicts with the primary role of the doctor, while others offer a moral defence of junior doctors striking, arguing that limited action is not harmful to patients because senior colleagues can be reallocated appropriately (Chima, 2020; Toynbee et al., 2016).
Retrospective analysis of the strike has thus far focused on patient outcomes, primarily due to the far-reaching effects of the industrial action on the general public of England (Furnivall et al., 2018). The occupational identity of junior doctors, which is heavily rooted in patient care, in this study served to dilute and ultimately thwart the effectiveness of the strike action, both through doctors’ own commitments to patients and as used as a tool by government to sway public opinion against their action. This article explores how this failed action threatened doctors’ professional identities. In turn, the article explores how a reworking of junior doctors’ professional identities helped them accept defeat in the strike and refocus on their careers. We show this though a longitudinal qualitative study, providing nuanced insights into the tensions that challenge junior doctors’ working lives, by addressing the following questions:
How did junior doctors’ failed strike action threaten their professional identity?
What mitigation strategies were employed by junior doctors in response to professional identity threats?
Our findings are threefold and are located around the identity threats and identity reworking experienced during the industrial action, whilst also adhering to the Hippocratic Oath of upholding patient care. Firstly, the failure of the industrial action was alleviated by a reluctant acceptance of weak bargaining power unique to their profession, which effectively prevents meaningful withdrawal of labour. Secondly, a lack of recognition for excessive and intensive work was alleviated with a reconnection to normative professional values of patient care. Finally, frustration with nonclinical management was alleviated with a focus on their future career potential.
The contribution of this article is to show how professional identities and identity work can moderate the outcomes that follow from workers’ defeat in industrial disputes. This is important more generally because evidence suggests that in some contexts, such as long strikes utilising replacement workers (Krueger and Mas, 2004) or contract disputes (Mas, 2008), workers’ defeat leads to long-term deterioration in product or service quality while in others quality returns to pre-dispute levels (Gruber and Kleiner, 2012). Identity work and identity provide a theoretical mechanism to explain this divergence. It is also important in the specific context of the English NHS, where there are record treatment backlogs as a consequence of the COVID-19 pandemic combined with ongoing unrest among junior doctors, as well as nurses and paramedics, over pay levels that are being rapidly eroded by inflation, which in turn threaten future strikes.
The article proceeds as follows: the next section discusses the context of the junior doctors’ industrial dispute, then reviews literature on professionalism before considering identity regulation and ‘identity work’ as concepts crucial in understanding the self and where one fits into an organisation/profession. The article then details the qualitative, longitudinal methodology, from the dispute and following their return to work, and post-imposition of the new contract. Findings are presented in terms of the identity threats experienced by junior doctors, followed by the alleviation strategies used by them to construct reworked identities in light of the new landscape of their work. Finally, theoretical and practical implications of the research are discussed.
Context of the junior doctors’ dispute
Junior doctors are qualified doctors who have graduated from medical school and are in clinical training. They have anywhere up to 10 years’ experience working as a hospital doctor under the supervision of a senior doctor, excluding any additional time spent undertaking self-directed training or education. They progress from two years of formal foundation training, where they rotate around several different medical and/or surgical specialties, through to speciality training and then spend several years as a speciality registrar in their chosen field. Then they are able to progress to consultant as an established senior hospital doctor, or as a fully qualified general practitioner (BMA, 2022). Labour disputes in healthcare are typically significant political events (Szabó, 2022) and this was no exception. The Secretary of State for Health intervened in an ongoing negotiation over a new contract, threatening to impose new terms, which resulted in a general strike of junior doctors across the NHS, including withdrawal from routine and emergency care. This was the first time such action had happened and resulted in significant public and media attention (Bessa et al., 2016).
One of the principal reasons for the junior doctors’ strike was the proposed imposition of a detrimental contract, removing additional pay for anti-social hours, adjusting their working time patterns, and the alleged subsequent risk to patient safety. Junior doctors’ working lives have been subject to much enquiry in the medical literature, and are characterised by long hours at work, low levels of morale (Bessa et al., 2016; Hart and Warren, 2015), high levels of occupational stress (Swanson et al., 1998; Zhou et al., 2019), ever-increasing workloads (Hobbs et al., 2016), sexism (Nicholson, 2002) and persistent agitation from nonclinical managers (Bessa et al., 2016; Doolin, 2002). Nonetheless, careers in medicine remain popular: a record number of students (68,680) applied for undergraduate medical degree courses in the academic year 2018–19 (Universities and Colleges Admissions Service [UCAS], 2019).
The dynamics of this ‘white collar’ strike were qualitatively different to our typical understanding of industrial disputes over pay and conditions, and thus the experiences of those who took part in it offer potential new insights into the dynamics of professional industrial disputes. The focus of this dispute, although related to pay and conditions of work, was also rooted in threats to the professional identities of the doctors: identities which, at the same time, may prevent them from effectively withdrawing their labour. On the other hand, public sector or medical professionals might be able to use their societal position and social standing to garner public support for trade union demands (Schmalz et al., 2018). There may be cases where professionals such as doctors have a bargaining advantage when their objectives chime with the public interest, such as demands which focus on safe staffing of medical wards; however public support is likely to be lost where action is seen as defending privilege (Schmidt et al., 2019). Campbell and Haiven (2012) explored labour disputes in professional workers, classed as dominant rather than subordinate employees, in terms of their striving to maintain professional control. Building on their findings, this article aims to explore the unique effects of an industrial dispute through the lens of professional identity threats and subsequent reworking. Identities at work are both constrained and enabled by organisational and occupational context (Ashforth and Schinoff, 2016; Brown, 2017). Individuals in all lines of work can be faced with threats to their identities (Petriglieri, 2011), however less attention has been paid to professionals and their identity rework in response to apparent assaults on their professional identities (Brown and Coupland, 2015; Gill, 2015).
Professionalism and identity at work
The extensive body of literature surrounding professionalism, and what it means to be a professional, is broadly split into two categories: structural and normative/rhetorical. Both are vital in understanding the contemporary lived experiences of junior NHS doctors. Structural professionalism (Freidson, 1970, 2001; Macdonald, 1995) outlines the concept of becoming or being a ‘professional’ as needing to adhere to certain criteria. An occupation must successfully navigate a ‘professional project’ (Larson, 1977) in order to become a profession. Freedom, impartiality and public service are seen as cornerstones of structural professionalism. Importantly, given that Freidson (2001) calls for professionalism to be maintained in the face of an ‘assault’, the professions are acknowledged as having been, and as will be discussed, continuing to be, faced with forces attempting to instigate unwelcome change. The ‘assault’ on professionalism is considered to be due principally to the encroachment of managerialist actors who were originally considered an unnecessary element of a self-policing, self-regulated profession (Raelin, 1991). Whilst the stark ‘deprofessionalisation’ theses of the 1970s (Haug, 1972, 1975, 1977) have not completely materialised, the management styles of large businesses, and the creation of multiple levels of management hierarchy, have encroached far into the medical profession (Doolin, 2002; Exworthy, 1998; Learmonth, 1997).
Other interpretations of professionalism have reconsidered the concept as one principally based in normative rhetoric and behaviour, rather than rigid structure. Being a professional is understood more to be a matter of conduct (Grey, 1994, 1998), and ‘appropriate’ work identity (Fournier, 1999), as well as an instrument to discipline and control people at work (Muzio and Kirkpatrick, 2011). The discourse of professionalism operates as a powerful instrument of occupational change and social control (Evetts, 2013), playing a crucial role in understanding the identity and motivations of professionals at work (Barbour and Lammers, 2015; Muzio et al., 2013).
The concept of identity loosely refers to subjective meanings and individuals’ experiences in answering questions such as ‘who am I?’, ‘how should I act?’ and ‘where do I want to be in the future?’ (Alvesson et al., 2008; Brown and Coupland, 2015). Personal identity weaves together feelings, values and behaviour and can be grouped together by individuals to form group, organisational or professional identities. The management of identity is understood to be an ongoing, instinctive project requiring constant identity work (Giddens, 1991), which is ‘the ongoing mental activity that an individual undertakes in constructing an understanding of the self that is coherent, distinct and positively valued’ (Alvesson et al., 2008: 15). It involves construction, upkeep, renovation and sometimes complete overhaul (Brown and Coupland, 2015), through which people seek to realise the ideal version of themselves (Caza et al., 2018). The aforementioned rise in managerialism in healthcare is important to consider here, given that mechanisms of bureaucratic-style control in knowledge-intensive organisations are inextricably linked with the identity work of employees (Alvesson and Willmott, 2002). Thus identity work is very much a medium and an outcome of organisational control. The context-sensitive nature of identity, the high levels of workload, stress, anxiety and burnout (Lundin et al., 2018; Monrouxe et al., 2017), combined with the relative subordinate status of junior NHS doctors, create the necessary conditions for their identities to be questioned, threatened and consistently reworked.
Identity threats: Their occurrence and responses
As has been established, individual identities may be insecure and as such are subject to regular, sustained threats from multiple contextual, organisational and hierarchical forces. The demands of normal life, and particularly of high-stress medical work for early-career doctors, may lead to self-doubt and emotional instability (O’Donnell et al., 2012). Insecurities are acknowledged to have the potential to exist in multiple forms: according to Collinson (2003), they can be at the same time existential, social, economic and psychological. The extant literature portrays individuals at work as in a consistently precarious position, particularly those with high levels of organisational or strategic responsibility (Gill, 2015).
Identity threats may take multiple forms. According to Brown and Coupland (2015: 1318), ‘identity threats are regarded as being construed through identity work: they are any discursively constituted thought or feeling that challenges one of an individual or group’s preferred identity narratives’. Threats are not only discursively formed through everyday experience however: temporally specific, one-off events such as job loss can constitute a significant threat to an individual’s identity too (Shepherd and Williams, 2018). Similarly, organisationally-developed actions that threaten a group’s identity can be met with active resistance in order to protect that group identity (Ashforth et al., 2008). Individuals respond to threats to their identity in a manner of ways. The majority of the literature acknowledges that people pursue strategies of conforming, resisting and impression management (Collinson, 2003). More recent research (Brown and Coupland, 2015) has identified how professional sportspeople construct and manage the various threats to their identity by deploying appropriation strategies designed to mitigate against inauspicious features of their profession, such the pervasive risk of injury. Knights and Clarke (2014) explored the insecurities of academics in business schools, and illustrated how academics cope with their insecurities through a threefold typology of impostors, aspirants and existentialists.
Professional roles and identities in healthcare
Professional identities are acknowledged by Pratt et al. (2006) as being formed, and reformed, by junior doctors from the outset of their medical training, particularly during times when they experienced a mismatch between what they thought of themselves, and what they were expected to do. Doctors who behave in ‘professionally appropriate ways’ elicit positive emotions from medical students, and as such, act as powerful triggers for identity work in aspiring physicians (Dornan et al., 2015). The same is highly likely of junior doctor interactions with their seniors. The continuous nature of identity (re)formation in individuals means that fluctuations in the status and professional identity of doctors are experienced constantly, from the outset of medical training to the end of their career (Foster, 2011). Monrouxe et al. (2017) found low levels of self-reported professional identity were associated with high levels of work-related burnout, though causal direction here cannot be determined. Importantly though, low levels of professional identity and the resulting effects on job satisfaction may result in high levels of intent to leave a profession, both in geographical and absolute terms (Humphries et al., 2015; Sharma et al., 2012).
As discussed, professional autonomy is prized by physicians: they have been known to fiercely resist attempts by nonclinical managers to intrude into their professional space and risk the wellbeing of patients (Doolin, 2002; Waring and Currie, 2009). More recently, Kyratsis et al. (2017) investigated the identity threats experienced by physicians facing pressure for change in their professional identity due to an organisationally-led shift in management logic. They identified three forms of professional identity threats: professional value conflict, status loss and social identity conflict; and three corresponding forms of identity work: authenticating, reframing and cultural repositioning, which acted to ameliorate the aforementioned threats. Bolton et al. (2019) explored the professional identity threats experienced by Greek doctors, who saw managerial encroachment into their national healthcare system as the involvement of a negligent and corrupt state. However the unique and ever-changing nature of identity means that not all doctors see managers as having competing goals from practising physicians: some senior doctors identify with and adopt a ‘hybrid’ role where they take on managerial roles as part of their workload (Iedema et al., 2004; Kirkpatrick et al., 2008, 2009; Noordegraaf, 2007), signifying a departure from the derision usually associated with the clash of cultures between professionals and bureaucrats (Raelin, 1991). Nonetheless, the ‘traditionalist’ understandings of managerialism being at odds with medical practice remain a somewhat pervasive identity amongst senior clinicians (Martin et al., 2020) and nurses (Bolton, 2004; Cooke, 2006) alike.
As seen, there is clear diversity of scholarship related to the professional identity of doctors. Whilst a broad, discursive approach to the concept of how individuals conceive threats to their identity enables research subjects to talk more in-depth and to draw from a wide range of experience (Brown and Coupland, 2015), acute and temporally specific events offer fertile ground on which to locate an investigation into how those events might initiate identity work in the people experiencing them (López-Andreu, 2019; Park and Murray, 2014). Thus, the aim is to develop theory from discursively constituted understanding of identity threats constructed by junior NHS doctors through the lens of an unprecedented, temporally specific event: the strike of 2016. We now discuss the methods we used to do this.
Methodology
This article discusses qualitative data from a mixed-method longitudinal study of the work experiences of junior NHS doctors during a single period of industrial conflict, concerning a new detrimental contract, and in a follow-up data panel two years later. The strike comprised three days of labour withdrawal in January, February and April in 2016. An abductive research strategy was implemented, where the researchers developed theory, generated data and analysed data simultaneously in a dialectical process (Mason, 2002). Critical to the abductive approach is the entry of the researchers into the world of the research subjects, in order to understand the motives and reasons that accompany social activities (Blaikie, 2009). We now discuss data collection as part of this strategy.
Data collection and sampling
Twenty semi-structured interviews were initially conducted with junior doctors during the period of industrial unrest (November 2015–February 2016). Interviews were purposively sampled, with the researchers initially utilising personal contacts to identify potential candidates. Snowball sampling was subsequently utilised to expand the sample from the initial interviews (Bobek and Devitt, 2017). Limitations of this strategy are recognised in terms of limiting the sample to a group who were professionally in contact with each other to some extent, however they were from a range of clinical locations and levels, and none of them worked on the same wards. Alongside the interviews, the researchers gained permission to join junior doctors on their picket lines, advancing a participant observation methodology (Masood, 2019) which yielded contextually rich insights from striking doctors. Additionally, 13 follow-up interviews were conducted from the same initial sample after the failed action, to gain a deeper understanding of how attitudes towards work and trade union membership had changed since the imposition of the new contract in September 2016. The number of these was reduced because some of the initial participants were no longer junior doctors, because they had qualified as consultants or other senior roles, and were excluded for that reason. Other reasons for attrition from the first sample were relocation or not responding to follow-up contact. These interviews took place between September 2017 and March 2018. This enabled effective and meaningful triangulation of data from the same interviewees, in order to understand how subjects’ identities had transformed over the time elapsed between interviews. Interviews lasted between 25 minutes and one hour, and written consent was received from participants to record interviews. To unpack and explore contextually rich and personal insights into identities surrounding a profound career event, richness and depth of data were prioritised over a larger sample size (Baker and Edwards, 2012; Saunders and Townsend, 2016).
The first section of each interview was structured on socio-autobiographical grounds (Chamberlayne et al., 2000). Interviewees were asked to recount their early aspirations, education and career histories from the point of entering medical school, through the use of generalised, open-ended questions such as ‘tell me how you’ve got to this point in your career, and what it’s been like for you?’ The rich, long, detailed answers given enabled the researchers to pick up on cues regarding professionalism, which enabled further probing questions to be asked, such as ‘what does it mean to you to be a doctor?’, which offered a more nuanced understanding of interviewees’ professional identities. Following this, interview questions focused more on the specific context of the industrial action and the perceived effects of it on the interviewees’ identities: an example question in this section was ‘how do you feel about the strike?’ (and in the second round of interviews: ‘looking back on the strike: how do you feel about them now?’). Asking such questions enabled the specific socio-political context of the junior doctors’ strike to be explored in terms of how the events were perceived as an ‘assault’ (or otherwise) on the professional identities of the junior doctors that made up the sample (Rubin and Rubin, 2011). These questions also enabled the researchers to understand how interviewees coped with, and justified, the imposition of the new junior doctor contract, as well as how it affected their career plans and professional values.
Data analysis
Having been fully transcribed, all interviews were uploaded to NVivo. Interviews were analysed using a thematic (Braun and Clarke, 2006) method. For the first cycle of coding, the authors made note of the broad themes in each interview in a manner Miles et al. (2013) term ‘descriptive’ coding. The second cycle coding method utilised was ‘pattern coding’ (Saldaña, 2009). Pattern codes are ‘explanatory or inferential codes, ones that identify an emergent theme or explanation. They pull together a lot of material into a more meaningful and parsimonious unit of analysis’ (Miles and Huberman, 1994: 169). Pattern coding was appropriate to utilise in understanding the perceived identity threats that junior doctors understood themselves to be facing, as well as the alleviation strategies that they employed to substantiate them. Given the longitudinal nature of the research, thorough triangulation of interview data was key in understanding the contours of interviewees’ perceptions over the time elapsed between interviews.
A note on reflexivity
The context of this research is particular to the lead author. Whilst a great deal of qualitative data analysis is presented as a neutral, value-free and decontextualised process (Mauthner and Doucet, 2003), in this research, the subjectivity of the lead author was closely entangled in the lives of the interviewees because the initial interviewee and the inspiration for the research itself was their partner. The other two authors have no such relationship and were equally involved in data collection, analysis and interpretation. As such regarding the lead author, issues of reflexivity (Cunliffe, 2003, 2011; Denzin and Lincoln, 2011) in data collection, data analysis and the presentation of data, which follows this section, were apparent. The close relationship between the researchers and interviewees, we argue, adds authenticity and strength to our findings for multiple reasons (Berger, 2015). Firstly, exceptional access was gained to a hard-to-access (principally due to their working hours, as will be discussed in the next section) group, because respondents were willing to share their experiences with a researcher they perceived to be familiar with, and sympathetic to, their situation. Indeed, the author’s own familiarity with tedious bureaucratic processes gave rise to some very honest exchanges because interviewees were very comfortable discussing their thoughts, feelings and opinions with an interviewer with whom they had spent time on the picket line.
Issues of reflexivity were considered throughout the research process, in order to maintain the credibility and quality of the research. This was particularly apparent during interpretation of the data, but also in critical self-reflection on how the data are presented (Alvesson and Sköldberg, 2009). The input of the other two authors was crucial in achieving ethical, valid data and findings. Interview analysis and presentation of findings were carefully undertaken by the wider group of authors, in order to avoid ‘unconscious editing’ because of the lead author’s relationship and consequent sensitivities (Valentine, 2007). As such, the projection of potential political biases and the risks of blurring analytical boundaries were reduced as much as feasibly possible, whilst maintaining the openness and honesty that added so much to the interviews. The research team remained constantly alert to avoiding projecting their own experience on interviewees or the data they generated (Sword, 1999). Whilst no qualitative researcher can completely separate the self from the data collection and analysis activities in which they are intimately involved, we argue that our attendance to and self-scrutiny of those effects has secured and heightened the credibility, trustworthiness and non-exploitation of the phenomenon that we explore in this article.
Having outlined the methodological and analytical approaches taken in this research, we now turn to a discussion of the identity threats and alleviation strategies uncovered.
Findings
In this section we analyse three specific threats to junior doctors’ identities (the negative outcome of the industrial action, tensions between work requirements and professional values and nonclinical managers’ encroachment into their work practices) and the three strategies used to alleviate these threats (a reluctant acceptance of weak bargaining power, a reattachment to normative occupational values and a focus on the future, respectively). These threats and alleviation strategies are presented in matching pairs, which illustrate a nuanced picture of the working lives of junior doctors during and after an industrial dispute.
Identity threat one: Failure of the industrial action
The industrial action carried out by junior doctors and their representative trade union, the BMA, did not ultimately end in success: the contract that they were bitterly opposed to was imposed upon them by the Health Secretary and NHS employers. A key contributor to this failure was doctors’ sense of professionalism, underpinned by their Hippocratic Oath, which prevented them from exercising a meaningful withdrawal of labour. One of the prerequisites in organising the action was to ensure that care continued for patients, so that the worst effects of the strike were disruption to shift rotas. Publicity and momentum were gained rapidly at the start of the dispute, but as they progressed, those taking part in the action found their credibility called into question as public goodwill tailed off in the face of a questioning media. Their Hippocratic Oath was used to delegitimise any withdrawal of labour:
I think that there has been a lot of miscommunication, to the general population and from the government. . . a lot of media coverage was aimed at giving negative associations to doctors. So the strikes became less about the true problem and were redirected towards other things and were lost. So the momentum fizzled out, and soured opinions and any impact was dampened down. And before you know it, it’s several months down the line and there’s a new contract and nothing you can do. (Heather, 28, GPST2)
1
The industrial dispute itself, in a more extensive manner than the negative outcome of the strike, was what we found to threaten junior doctors’ professional identities. This was principally because they never expected to be partaking in extended strike action, and as the strike went on they developed anxieties surrounding their Hippocratic Oath as a complicating factor in their decisions to withdraw labour. Junior doctors’ interpretations of the industrial action, when asked about what they felt the strike achieved, revolved around themes of resignation in the face of weak bargaining power, and moral fortitude that they had done their best to raise awareness of their intense working conditions and a commitment to upholding the Hippocratic Oath. The following quote demonstrates a theme that emerged strongly amongst our interviewees, which suggested that the professional values of a doctor were incompatible with a withdrawal of labour:
I think actually the expectation of what we were going to achieve, the hope was that they could, the government would bow to its knees and say we know we can’t function without junior doctors, because I think that’s really what everyone knows, but you have got to be able to bear out and be the brick wall that does cause harm to show that. And actually that’s what most, a lot of people weren’t prepared to do. (John, 28, anaesthetics registrar)
So the professional identities of junior doctors were rooted in their Hippocratic Oath, which effectively rendered their action weak and meaningless. Their reluctant acknowledgement of the weakness in their bargaining power as a result of this oath was central to a refocusing of their professional identities, which served to alleviate the initial identity threat.
Principal alleviation strategy: Reluctant acceptance of weak bargaining power
The strong concern of potentially harming patients prevented meaningful disruptive strike action from taking place. We constitute the concept of ‘unwilling acceptance’ as an alleviation strategy because it was deployed by interviewees as a means to distance them from the highly publicised inferior working conditions that are a feature of their day-to-day work. Additionally, it served to reconnect them with their profession, in the sense that participants noted how they lost the support of the mainstream media and the general public as the strike went on. Thus, threats to interviewees’ professional identities brought about by going on strike were alleviated by carrying out identity work that reconnected them to their sheltered, exclusive position in the labour market. It is clear that they could not control the ‘terms, conditions, goals and content’ of their work (Freidson, 2001: 60): a feature of the junior doctor labour process is a lack of autonomy and discretion at the early-career stage. Nonetheless, interviewees displayed a resolute commitment to each other – and thus to the profession – whilst experiencing a multifaceted loss of goodwill from the government, the public and NHS employers, as illustrated by the following quote:
I think it was nice that there was unity among doctors for the first time in a long time, and that we made the issue public because it affects the public. But to be honest I feel like most of it was wasted time because the majority are on new contracts. And that’s what we were fighting for, to not be on them. (Tamara, 28, GPST3, second interview)
This professional commitment was echoed by senior members of the profession: during the dispute, in solidarity with junior doctors, consultants acted as rota cover whilst junior doctors withdrew their labour, which acted to further solidify juniors’ identity work and thus their professional identity:
. . . even though the junior doctors were striking, the senior doctors all pulled together to actually all cover the rota. And so obviously they all supported us as well. Unfortunately though I don’t really feel like they [the strikes] made much of a difference, because the new contract went ahead anyway. (Naomi, 26, foundation trainee, interview 2)
The unique commitment of the medical profession, both to colleagues and to the patients they care for, was illustrated here and again reinforced why the strike was unsuccessful. Senior doctors covered the junior doctors’ shifts, and this was seen as supportive. In many other professions, this would be seen as ‘scab labour’ to break a strike. A culture of care and collegial support remained key to professional identities, but this culture ultimately served the financial logic of the NHS, in permitting the imposition of less costly contracts on junior doctors; a theme we examine in more detail later in the analysis.
Identity threat two: Lack of recognition
Closely related to the contractual reasons which led to the industrial action mandate was a lack of recognition and appreciation for the intense work which junior doctors endure, from long shifts without breaks to frequently working unsociable hours. Participants frequently mentioned a lack of recognition or appreciation for their work, both in relation to the government’s Department of Health as well as individual NHS Trusts which oversee junior doctor training:
I probably sort of coped with the job quite well, I manage to enjoy it on a day to day basis, I’m paid relatively well. And it’s a noble job. But actually you get no reward for it, there’s no gratitude, the government thinks you’re well. . . they just don’t value you at all. (Nathan, 28, GP trainee, interview 2)
Participants viewed the strike action as having the potential to bring to light wider issues of junior doctors’ unsafe working patterns and workload, but given the negative outcome of the strike, they ultimately interpreted the result as overwhelmingly negative for both contractual and status-based outcomes. While professions are considered to have public gravitas (Freidson, 2001), our interviewees displayed unease with how quickly levels of public support for them appeared to dwindle during their strike, in the face of the considerable pressure applied to them by the government and the NHS Trusts employing them, which was in turn amplified by the media.
. . . we feel very unsupported as a profession. I think the public, first of all kind of supported us, but then slowly the support petered out because we’d had three strike days and a lot of the public opinion was come on get back to work get on with it. So we feel like really there is not much support there or understanding really about what the new contract actually involves, and what is actually going on in the NHS on a day to day basis that we see, we are frontline staff. (Naomi, 25, foundation trainee)
Our interpretation of this identity threat is that the ‘public recognition of collective worth’ (Larson, 1977: 155) afforded to healthcare professionals was seen to have significantly decreased. Threats to the social standing of a career in medicine were also apparent because participants conveyed that their views on the issue were not being taken into account, and how they as juniors were treated principally as service providers rather than as respected professionals. This served to separate junior doctors from the aspects of their work which gave them their professional identity in the first place: that is, providing healthcare to people in need of it. An example of this strength of feeling came from one participant who had actively dissuaded a family member from going to medical school.
Principal alleviation strategy: Reconnection with normative professional values
Recognition-based threats to junior doctors’ identities were tempered by an understanding that whilst being a ‘prisoner of their Hippocratic Oath’, they work in a captive labour market, which also negatively impacts on their bargaining power as they cannot realistically move to alternative employers. Thus this threat was principally alleviated through identity work that served to reconnect the junior doctors to their normative occupational values: those of caring, selflessness and a deep commitment to public service. As summarised by one interviewee:
I think it’s really nice to go to work and I think. . . this sounds really clichéd, but really feel like you have made a difference, and you have put in extra effort and made the help that you needed, and someone else could have done that and maybe they wouldn’t have taken the time to explain it, or understood that they wanted to bring the family and stuff like this – you could make it really personal, but I think it’s a great thing to do. (Sonia, 28, CMT)
2
Despite the varied and extensive threats to junior doctors’ professional identities that became apparent over the course of the interviews, there was very little discussion surrounding leaving the profession. Those who had given it consideration, principally ruminated about private practice – however the idea of working in a for-profit healthcare organisation was not a strong theme in the data, as illustrated below by a participant expressing negative sentiment towards it:
I don’t know whether I want to do that. Not because I have anything against it. But I love working in the NHS and what it stands for, and I wouldn’t want to go purely private and be part of a company that maybe necessarily isn’t just out of health reasons. (Jennifer, 28, obstetrics and gynaecology registrar, interview 2)
A resoluteness to continue practising medicine was a particularly dominant theme within the data, as we would expect due to the captive labour market, but strength of expression to advance careers within the NHS was also strong. We found that junior doctors reworked their identities surrounding a desire to work in a free-at-the-point-of-access healthcare system, and for the opportunity to exercise the classic facets of Freidson’s (2001) archetype: to practise specialised work, to perform their work in the shelter and security of a controlled labour market, to complete their occupationally-controlled training and thus (over time) to gain control over their labour market and organisational positions. This was done with acceptance that they receive little recognition for their intense and challenging work, and have little discretion over it; however the wider role they play in providing care for those in need remained the underlying positive force constructing their professional identities.
Identity threat three: Frustration with nonclinical managers
The maintenance of a selfless culture of patient care, underpinned by doctors’ Hippocratic Oath was a major factor in the failure of their strike. In turn this served the financial aspirations of the NHS and the Department of Health well, specifically allowing a detrimental contract to be imposed and lowering the overall cost of employing junior doctors. We now turn to our final identity threat, which was rooted in the financial and bureaucratic concerns of nonclinical managers. In their day-to-day work, junior doctors generally experience ‘management’ from two separate sources: clinical managers, who are senior medical practitioners responsible for the day-to-day running of clinical directorates and departments; and nonclinical hospital managers, who are responsible for activities like overseeing waiting-time targets and financial planning. Across the two rounds of interviews, junior doctors were generally positive about their experiences of clinical management, principally due to the fact that they were fellow ‘professionals’ and their managerial roles extended to valued clinical supervision and professional mentoring or career development. Dissatisfaction with nonclinical management, however, was widespread and acute. One particular recurring concern was that performance targets and bureaucratic tasks set by nonclinical managers forced doctors to act in a way that was not in the best interest of their patients:
Management give you shitloads of paperwork, I don’t really know for what reason, it’s meant to improve patient care, but it removes people from patients, so therefore you have less patient interaction and more patient harm. (Ellen, 26, foundation trainee)
Such frustrations formed a strong theme among our participants. Naturally, they saw the concerns of nonclinical management (things like waiting times, patient turnover, bureaucratic administrative tasks) as being of a lower priority than clinical concerns. It was generally acknowledged that nonclinical managers were only responding to centrally-imposed guidelines, but this did not act to assuage the frustrations of junior doctors. The conflict between junior doctors’ desires to provide the best, most clinically appropriate care for their patients, and their inability to do so because of managerial demands/constraints, stemmed from a perception that performance targets and bureaucratic demands were detached from the reality of clinical situations. This conflict posed a real threat to their professional identity. In one interview, a core medical trainee discussed the imposition of a four-hour time limit for accident and emergency patients to be triaged. Breaching this four-hour limit would result in a £10,000 fine to the NHS Trust which manages the hospital, but the interviewee expressed frustration at the unrealistic nature of the time limit due to understaffing and clinical priorities:
. . . the idea was that you know people will get seen you know swiftly and promptly and decisions will be made quickly, which is like you know a good idea. It’s probably come from somebody from like management or HR or like something, or like finance or some department who doesn’t actually have much clinical contact with patients, and who hasn’t worked on the shop floor in A & E and doesn’t know what it’s like because it’s completely unrealistic. (Anna, 25, CMT)
Whilst the frustrations of being answerable to many nonclinical managers were apparent, the main source of identity threat was that junior doctors saw themselves as generally unable to eschew these managerial instructions, despite their concerns that certain targets were unreachable, potentially dangerous, or that certain administrative tasks were a waste of expert time. As such, our interpretation is that the junior doctors constructed the intrusion of nonclinical managerial practice as a threat to their identity principally due to their lack of discretion or authoritative power to overcome or bypass it. A key hallmark of a professional in structural terms is that they are able to exercise skill and discretion in implementing specialised knowledge (Freidson, 2001). However, the labour process of junior doctors is such that early-years clinical practitioners are still subject to a myriad of direction, particularly from nonclinical backgrounds, and there is little they can do about it. The cause of this subjugation of clinical discretion to performance targets was driven by the increasing financial logic of the NHS. The outcomes are adherence to performance targets and improved financial performance of clinical departments and NHS Trusts. However the side-effect of this is a perception amongst the clinicians in our sample that clinical expertise is at times overridden, with the potential to put patients at risk, whilst damaging the identity of those providing the clinical care.
Principal alleviation strategy: Focus on future careers
Our participants circumvented the perceived threat of nonclinical managerial encroachment by focusing on their completion of training and a belief that they would achieve professional autonomy and discretion. After a mandatory two-year ‘foundation’ programme after completing medical school, clinical specialties require varying amounts of time to complete their training programmes. General practice is shortest (three years) and anaesthetics/surgery are generally considered to be the longest, with a minimum run-through of seven years to reach completion of training and achievement of a consultant position. Within these training programmes, junior doctors complete a number of ‘rotations’, which last between four and six months in length. A focus on the future provided strong motivation for trainees to get on with their day-to-day work, as each four to six month rotation acted as a ‘stepping stone’ to their ultimate goal of becoming fully qualified. This served to alleviate the day-to-day stresses of enduring nonclinical managerial encroachment, whilst working in typically highly stressful and understaffed conditions:
I think there’s definitely a promotions prospect when I could be a consultant, and I think being a consultant would be a nice job. But I think the route to being a consultant is horrible. Like being a CMT [core medical trainee] like I am now is horrible, and being a registrar is horrible. So it’s like the pathway to get there is horrible but I think the actual prospect maybe is fine. (Sonia, 29, CMT, interview 2)
Our interpretation of this identity work is that junior doctors predominantly constructed their time as a ‘junior’ doctor as a period of their professional career in which a lack of discretion and autonomy was, and would remain, a major feature. Their enthusiasm for discussing their longer-term careers and becoming fully qualified through the achievement of a ‘certificate of completion of training’ acted as an effective strategy to reposition their professional identities as young professionals who still generally have a significant amount of the junior doctor training period to navigate. Upon reaching the upper levels of clinical hierarchy, doctors are acknowledged as being more willing to engage in subterfuge and resistance to bureaucratically-driven change agendas (Waring and Currie, 2009).
Discussion and conclusions
As has been noted in previous research on identity threats (Brown and Coupland, 2015), the appropriative strategies of individuals engaged in extensive identity work can frequently overlap, and a ‘matching-pair’ delineation of identity threats and appropriative strategies is a convenient simplification of a rather complex issue. Whilst the principal relationships between identity threats and alleviation strategies have been discussed in the previous section, the relationships between threats and strategies experienced by junior doctors were similarly far from linear. For example, whilst ‘reluctant acceptance’ appeared to be the foremost alleviation strategy in the face of the negative outcome of the industrial action, it was apparent that our participants could deploy identity work to reconnect with their normative professional values to alleviate the threat of strike defeat. Furthermore, others had employed the other alleviation strategy, a focus on the future, to rework identity away from that of a defeated employee, or to refocus on future contract renegotiations around consultant-grade pay and conditions.
Figure 1 illustrates the principal and secondary relationships between identity threats and alleviation strategies: as with other work in this area, we present this model with the caveat that processes of identity reconstruction are extremely personal, changeable and complex. This develops understanding of identity threats and insecurities by highlighting how, construed from temporally specific, professionally-demanding events, they can give rise to extensive identity rework in young professionals.
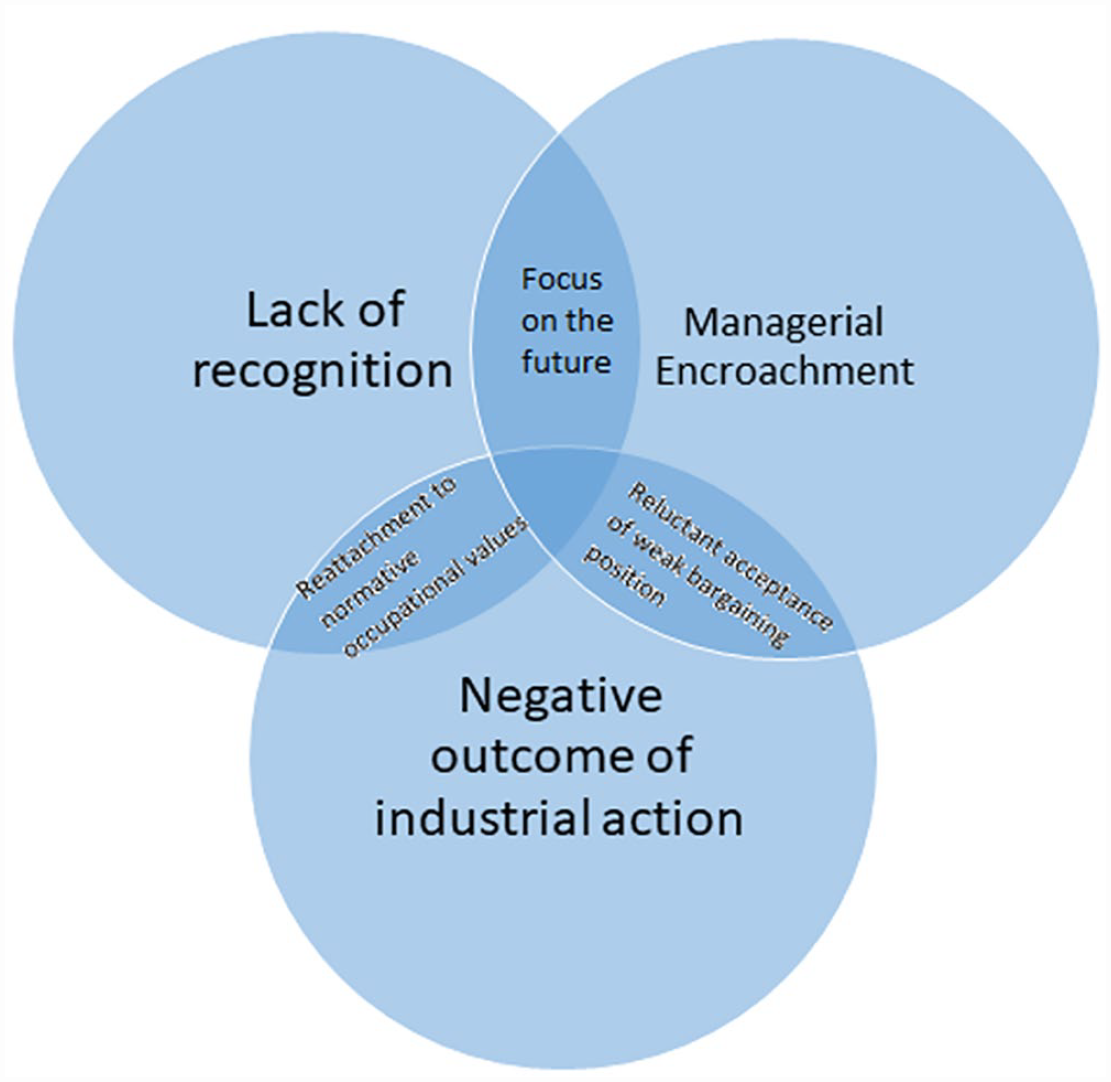
Identity threats and alleviation strategies.
This article set out to identify the key threats to junior doctors’ professional identities during, and how they mitigated these threats in the aftermath of, the 2015–16 conflict. Junior doctors are exposed to myriad stress-inducing phenomena in their day-to-day work (Hobbs et al., 2016; Nicholson, 2002). While previous research found that junior doctors’ morale in the lead-up to the strike was notably low (Bessa et al., 2016), this study found that the industrial dispute led doctors to ascribe feelings of low morale to the failure of the dispute, though the limitations of our methodology do not enable claims of causality. As such, their professional identities underwent significant (re)work during this time, because their attention was focused on identity in a more intense manner. Thus, our principal empirical contribution is that we have identified the fundamental professional identity threats experienced by junior doctors, and we have linked them to identity-work strategies they deploy to alleviate the perceived assault on their professionalism. In doing this, we address demands for additional research into established professionals’ identity development (Brown and Coupland, 2015), and highlight how early-career healthcare professionals do indeed construe anxiety-provoking threats and corresponding alleviation strategies as an ongoing part of their ‘projects of the self’ (Grey, 1994). In illustrating these complex, overlapping alleviation strategies, these findings also contribute to the literature on the sociology of the professions (Haug, 1977; Freidson, 2001; Kyratsis et al., 2017; Macdonald, 1995; Szabó, 2022). They do so by undertaking a contemporary analysis of junior doctors’ labour process, highlighting the increasing encroachment of managerial actors into doctors’ professional domains and illustrating the serious morale issues and professional insecurities experienced by them at a time of significant personal and occupational upheaval.
Implications of the research
We uncover the complex identity struggle experienced by junior doctors in being a ‘prisoner of oath’: the basic tool of industrial action, a complete withdrawal of labour, was deemed to have too many risks for patient care, putting lives at risk. This displays parallels with the ‘prisoner of love’ framework (England, 2005; Folbre, 2001), where care work is argued to be low-paid due to the altruistic motivations of carers and the intrinsic rewards of the work itself. By being bound to the Hippocratic Oath, junior doctors were unable to withdraw their labour in full and this was exploited by managerial and political actors. This illustrates a fundamental weakness in the abilities of junior doctors to meaningfully resist the imposition of new terms of employment through strike action. The findings herein suggest a potential route to more effective action, which is a suspension of non-essential administrative work whilst continuing patient care, thus creating disruptive impact without breaking the Hippocratic Oath, which builds on ideas that professional identity can in some contexts strengthen resistance against detrimental organisational change (Szabó, 2022; Wright, 1997). However in our study and to date in the UK NHS, resistance has been limited to small-scale disruption and sabotage by senior, fully-qualified clinicians (Waring and Currie, 2009). The practical implications of this are significant, and whilst our research found that few doctors were considering leaving the profession, low levels of morale, principally due to a perceived misfit between personal values (what it means to be a healthcare professional) and the requirements of a job, can lead individuals to seek alternative employment, where in the UK there are many such opportunities in the private healthcare sector (Humphries et al., 2015; Sharma et al., 2012). We did not seek or find evidence of deterioration in service quality affected by the contract dispute among our participants, as other research on contract disputes has found (Mas, 2008), however the persisting low morale that we did find helps to explain such findings. Finally, whilst recruitment problems were not found following the dispute (UCAS, 2019), retention issues amongst junior doctors in the NHS may well become apparent as wages or working conditions are not addressed, especially as inflation takes hold against a backdrop of likely further public sector austerity.
Limitations and further research
This study has a number of limitations which give rise to potentially fruitful avenues for future research. The in-depth, qualitative, longitudinal nature of our study has yielded deep insight into a very personal, contextually specific situation. As such, depth was prioritised over generalisability. Nonetheless, additional interviews would have further strengthened our work. Our sample was gender-diverse, and was limited to relatively young participants (none over 32 years of age): this is generally to be expected given the ‘junior’ nature of the interviewees in professional terms. The nature of the case is somewhat extreme: as a ‘key case’ (Thomas, 2015) it lacks representative generalisability but that is not what the research seeks to achieve, and in turn the analytic generalisability is rich: themes emerging from our sample are likely to be found in other healthcare workers exposed to similar threats. This study also represents a move away from cross-sectional explorations of identity (Brown and Coupland, 2015); however, further longitudinal research would shed more valuable light on the ‘becoming’ of junior doctors. Future research might explore in more detail the more mundane aspects of junior doctors’ work, principally the administrative and clerical tasks that contribute to their frustrations, to see if they can be more effectively carried out by nonclinical support staff in a manner similar to a ‘paraprofessional’ (Maister, 1993). The increasing popularity of the ‘physician’s associate’ position within NHS Trusts (Drennan et al., 2019; Patel et al., 2018) represents another intriguing opportunity to explore the interaction of junior doctors with ‘paraprofessionals’ to understand if their identities align.
Through exploring the working lives of the UK’s next generation of doctors around an industrial dispute, this study develops understanding of the threats to professional identities brought about by increasing searches for efficiency. New insights into the dynamics of ‘white collar’ strikes and their effect on professional identity are put forward. Given that the UK in particular, and developed economies more broadly, are struggling to address medical backlogs resulting from the COVID-19 pandemic and relying heavily on the labour of junior doctors, these findings are especially relevant. Indeed, the UK faces a significant struggle against inflation and rising living costs combined with strong political and market forces against public sector borrowing, leading to further industrial disputes in healthcare, so lessons learned from this research are likely to be of value.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.