
Abstract
Drawing on qualitative research in the main UK unions for nurses/midwives, this article explores union reps’ views of the functioning of workplace partnership in two feminized professions working in the English National Health Service (NHS). Through the investigation of two professional unions, which despite their vitality remain under-researched, the study offers an investigation of the interactions between formal and informal partnership arrangements at the workplace level, the ways in which they intersect with the professional nature of the union context, and the deterioration of working conditions. In doing so, this article contributes to reflections on the prospects of workplace partnership for professional trade unions.
Introduction
In the UK, union membership in the public sector remains strong (51.8%) compared to the private sector (13.5%) (Trade Union Membership, UK, 1995–2020). It is the presence and growth of numerous specialist unions representing specific (professional) occupations (teachers, nurses, midwives) that partly explain this vitality. These unions have a number of unique characteristics. They are strongly feminized and have diversified their membership. They have a high and growing union density, but they are rarely talked about or seen in the public space. Most of them can be described as ‘moderate’ (Kelly, 1996). They tend to display limited demands, infrequently threaten or use industrial action and believe in partnership arrangements (Bacon and Blyton, 2002; Kelly, 1996). Further, most of these unions fall under the category of ‘professional unions’ (Burchill, 1995), which have the characteristic of formally pursuing both economic and occupational aims, notably promoting the education and training of professionals as well as contributing to the improvement of the quality-of-service delivery. Claiming to be the voice of their profession, these unions build their power upon core occupational identities (Ackers, 2015; Kirton, 2018). Union framing and claims promulgate and endorse the values shared by professionals, which are transmitted by workplace reps drawn from the profession. Despite their contemporary importance in the UK, especially in the health sector, these professional unions remain under-researched, both in terms of their organization and the dynamics of workplace unionism (Guillaume and Kirton, 2017; Kirton, 2018). The literature on industrial relations in the NHS tends to look at the group of healthcare sector unions together (Bach, 2004; Givan, 2016; Tailby et al., 2004; Upchurch et al., 2008) or focus on Unison as arguably one of the more ‘unionate’ and militant unions in the sector.
Critical industrial relations scholars have traditionally criticized moderate trade unions (Hyman, 1975; Kelly, 1996, 1998), decrying the negative outcomes deriving from partnership practices (Danford et al., 2014; Martinez Lucio and Stuart, 2002), particularly in the context of liberal market economies (Upchurch, 2009). On the contrary, pluralist defence of participation through collective bargaining or workplace partnership is that it provides a means of regulating conflict and achieving mutual gains (Johnstone, 2015; Johnstone et al., 2010; Roche, 2009), giving workers an independent voice to express their distinct interests, and integrating them into stable democracies (Bacon and Blyton, 2002). Far from offering a conclusive assessment of partnership’s potential (Roche, 2009; Upchurch et al., 2008), empirical literature provides limited analysis of the dynamics, practices and processes that sustain such arrangements (Johnstone, 2015) at the workplace level (Butler et al., 2011), and over time (Johnstone and Wilkinson, 2018). Moreover, most studies were carried out during the first decade following the advent of workplace partnership initiatives in the UK (Ackers and Payne, 1998; Upchurch et al., 2008), before the 2008 financial crisis and the implementation of austerity measures in the public sector. There is also limited research investigating workplace reps acting both as professional workers and representatives of a professional union. And yet, the balance struck between resistance and accommodation has been described as more challenging for professional workers (Danford et al., 2014).
Drawing on qualitative and collaborative research with the main British unions for nursing/midwifery (Royal College of Nursing [RCN] and the Royal College of Midwives [RCM]) undertaken before the COVID-19 crisis, this article contributes to the literature by investigating workplace union reps’ and union officers’ views on partnership in two highly feminized professions working in the English National Health Service (NHS). Building on previous research (Bach, 2004; Bach and Givan, 2008; Bacon and Samuel, 2017; Carter and Pointer, 1999; Givan, 2016; Heaton et al., 2002; James and Kyprianou, 2000; Kessler and Heron, 2001; Lloyd, 1997; Munro, 2002; Tailby et al., 2004; Upchurch et al., 2008), the aim of the article is to examine three main propositions found in extant literature. The first contends that the resilience of workplace partnership arrangements over time has supported a cooperative relationship with employers and convinced trade unions, especially professional ones, to keep pursuing non-militant tactics (Gahan and Pekarek, 2013). The second proposition argues that workplace partnership intersects with/is affected by the professional nature of the union context, and the shared identities of managers and union reps (Danford et al., 2014; Dean and Greene, 2017). The last one claims that the deterioration of working conditions deriving from austerity policies has negatively impacted the functioning of (and belief in) partnership for professionals, as seen in other parts of public services (Kirton, 2018; Kirton and Guillaume, 2017).
The article is divided into four sections. First the relevant NHS workplace partnership literature is presented and reviewed followed by an overview of the mixed-methods approach of data collection. The main body of the article provides an analysis of RCN and RCM union reps’ and officers’ perspectives on formal and informal aspects of workplace partnership, the mediation role of the profession, and the impact of deteriorated working conditions on union participation. The concluding section offers an analysis of the dynamics and challenges of partnership for healthcare professional unions in the UK.
Workplace partnership and professional trade unions in the NHS
Since its creation in 1948, the NHS has developed a distinctive pattern of employment relations (Seifert, 1992), which has undergone significant changes from the early 1990s. Firstly, the NHS has always been characterized by high union density (Lloyd, 1997; Seifert, 1992), albeit declining, sustained by the growth of numerous specialist unions, representing specific occupations/professions (nurses, midwives, physiotherapy staff, radiographers, doctors) and the presence of large general unions such as Unison. The two unions investigated in this study – the Royal College of Nursing (RCN) and the Royal College of Midwives (RCM) – are examples of the numerous professional associations that are part of the NHS union landscape but with the former representing the largest occupational group in the NHS. Union rivalry and sectionalism are also part of the NHS industrial relations legacy (Bach, 2004; Heaton et al., 2002), with some unions competing to organize the same categories of employees (general unions such as Unison can also claim nurses and midwives).
In addition, the NHS is characterized by the coexistence of adversarial/distributive national collective bargaining and integrative/consensual joint consultation activities at the workplace level (Butler et al., 2011). While employment relations were initially very centralized, the 1990 NHS and Community Care Act, which created self-governing Trusts (comprising hospitals and other specialist services in geographical areas), has been followed by a process of decentralization (Lloyd, 1997) associated with the development of labour–management partnership initiatives at the local level (Bacon and Samuel, 2017; Tailby et al., 2014). Trust managers were given some authority to decide pay and conditions for their staff as well as the extent of union recognition. This process of decentralization was closely tied to the ‘NHS modernizing agenda’ of the late 1990s/early 2000s which obliged unions to cooperate with management in order to achieve reforms deemed as of universal benefit for all NHS stakeholders (Tailby et al., 2004; Upchurch et al., 2008). According to Bach (2004), within the new approach the traditional structures of union–management consultation became less central to the management of employment relations, with a shifting balance between more or less formal direct or indirect forms of participation (Heaton et al., 2002), depending on senior managers’ approaches.
Most NHS Trusts have generally established Joint Negotiating and Consultation Committees (JNCC), which consist of elected representatives organized by category of staff and cover consultation and negotiation on all pay and non-pay matters and conditions of service. While employee participation has been identified as effective at least for the nursing workforce (Bach, 2004), some JNCCs have been found to exert little influence on management policy due to narrow agendas focused on Trust policies, such as car park charges for staff, lack of senior manager involvement, under-resourced HR departments (Bach, 2004; Tailby et al., 2004), dearth of union activists (Bach, 2004; Carter and Poynter, 1999) and increased staff workloads.
Moreover, previous research has identified the possible discrepancies between formal partnership processes and informal labour–management relations at the workplace level, and the role of line managers as among the potential impediments to workplace partnership (Munro, 2002; Tailby et al., 2004; Upchurch et al., 2008). While studies identified NHS Trust managers’ continued commitment to pluralism and the industrial relations framework remained firmly collectivist (Bach, 2004; James and Kyprianou, 2000; Kessler and Heron, 2001), with some variation depending on senior managers’ approaches to the new structures and partnership ideals (Lloyd, 1997; Tailby et al., 2004; Upchurch et al., 2008), other studies claimed that middle management ‘obstructionism’ was one of the problematic aspects of workplace partnership (Munro, 2002). Tailby et al. (2004) also pointed to the lack of HR training among managers (including nurse managers), and some hostility to employee voice from managers representing manual workers. One of the reasons for this lack of enthusiasm for the principles and practices associated with partnership, which have been found critical in sustaining resilient forms of workplace partnership (Danford et al., 2014), is linked to the fact that managers were confronted by the most intense work pressure and stress (Tailby et al., 2004; Upchurch et al., 2008). At the same time, research has shown the increasing involvement of front-line managers in HRM, and the difficulty they had in performing multiple roles, in particular in the healthcare contexts (Hutchinson and Purcell, 2010), where they experienced competing loyalties among patients, team, organization and profession.
Finally, studies have pointed to the mediating effects of professional and occupational identities/ideologies on union strategies. While a traditional view among industrial relations academics is that an ideology of professionalism (such as that held by nursing and midwifery staff) tends to discourage collective organization and militancy (Carter and Poynter, 1999), some studies have shown that this is a simplification of the contemporary reality. Studies revealed how some trade unions have occasionally managed to challenge the gendered dichotomy of caring and professionalism/skilled work (Henttonen et al., 2013; Yates, 2010), and the connection to low pay and traditional (non-confrontational) collective action repertoires. Professionalism can indeed provide a basis for an occupational solidarity among nurses that can lead to union mobilization and organizing (Briskin, 2012; Krachler et al., 2021). However, few empirical studies have investigated how the dual role of professional trade unions manifests itself in everyday employee representation and consultation processes, such as workplace partnership.
Most of the studies led on the NHS are based on in-depth case studies and took place shortly after the introduction of partnership initiatives in the late 1990s, described at the time as a ‘bureaucratic and centrally driven process’ (Martinez Lucio and Stuart, 2002), and before the start of the 2010s austerity decade, leaving many questions unanswered. Has the resilience of formal arrangements over time supported the development of a nurturing model of partnership (Danford et al., 2014; Martinez Lucio and Stuart, 2005)? What has been the impact of austerity policies on the functioning of workplace partnership? How did professional trade unions that have progressively developed their union dimension (Bach, 2004; Kessler and Heron, 2001) manage to balance their dual role at the workplace level? These are the research questions that we intend to shed light on using a mixed-methods research approach.
Methodology
Founded in 1916 as a professional association and registered in 1976 as a union, the non-Trades Union Congress (TUC) affiliated RCN represents around 435,000 nurses, nursing students, midwives and healthcare assistants (around 90% female and union density approximately 60%). RCM was founded originally in 1881 and established under its present name in 1947; it represents around 48,000 midwives, student midwives and maternity support workers (around 99% female and a 98% union density). RCN England has approximately 1300 workplace reps (stewards, health and safety reps, learning reps) while RCM has approximately 745 nationally. Although the two union have some characteristics in common, notably their professional role and highly feminized membership, the value of their comparison resides in their difference in size and resources, their disparate exposure to competition from other unions and their contrasting organizing strategies. Besides, both have increased their memberships over the last 25 years or more.
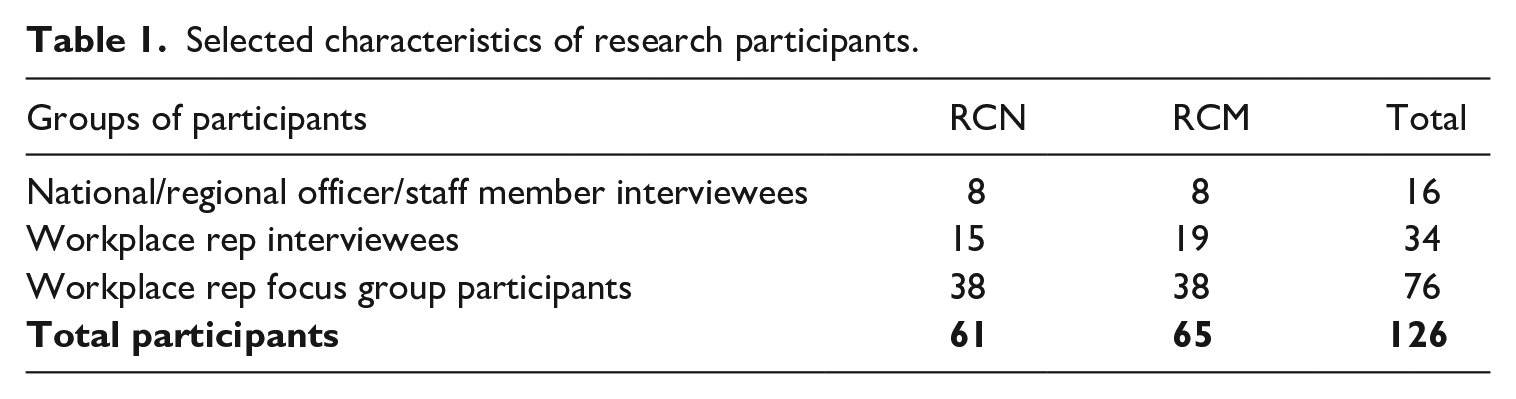
Fifty interviews were conducted with 16 union officers and 34 union reps (23 RCN and 27 RCM), working in 30 different workplaces, mostly in England. Four focus groups took place, two in each union, gathering 76 participants. Selected characteristics of research participants and their numbers are shown in Table 1. All worked in the National Health Service (NHS). Interviews and focus group discussions were carried out May 2018–December 2019 using guides containing themes, headline questions and prompts. This approach afforded some flexibility depending on participants’ roles and experiences, but also a large degree of thematic consistency across the interviews/group discussions. Interview/focus group guides were tailored to suit the different union roles but all covered work context and conditions of nursing and midwifery, union context, structures and strategies. Interviews were of 60–90 minutes’ duration and focus group discussions 60–120 minutes. Interviews and focus groups were conducted confidentially; therefore, we have made every effort to ensure participants’ anonymity. To this end, national/regional officers and staff members are rolled into one category – senior officer – when quoting from interviews with them and because of the small numbers involved, particularly in RCM. The main purpose is to distinguish officer/staff comments from those of workplace reps.
Selected characteristics of research participants.
All interviews were recorded and transcribed verbatim. Qualitative data were stored, organized, and thematically coded using research software NVivo. While the interviews initially aimed at exploring working conditions and workplace unionism, other themes relating to the functioning of social partnership emerged. These included: the attitude of managers and HR towards trade union reps and consultation bodies; the types of issues discussed in formal consultation bodies; the capacity of union reps to resolve their members’ problems through formal and informal channels of consultation; the difficulty of maintaining good relations with management, which are necessary to discuss professional problems, while continuing to defend the interests of members in a working environment under pressure.
In addition, an online survey of all RCN (England) and RCM workplace reps (stewards, health and safety reps, learning reps) was carried out May–August 2019. The survey asked a range of questions that comprehensively covered union activity around the challenges facing nursing and midwifery staff: reps’ union roles and participation, including member-facing, employer-facing and union-facing activities; broader workplace/branch organization and activities; union–management relations, relationships with other unions, union contribution to local NHS policymaking, improving branch effectiveness; and union strategies for tackling members’ concerns. The survey attracted 300 respondents: 77 RCN (6% response rate) and 223 RCM (30% response rate); the difference in responses between the two organizations can be explained by the different handling of the survey by the unions. In the case of RCN, we had a single contact who mainly dealt with diversity issues, whereas many RCM union officials, including regional secretaries, were involved in the survey (and therefore able to relay information to union reps). This is also probably a sign of a more active workplace unionism at RCM, resulting from a longstanding organizing strategy. Although RCN’s response rate is low, and therefore the results of the survey should be viewed with caution, answers of the reps of the two unions were convergent and echoed the findings of the interviews.
Ninety-five per cent of RCM and 74% of RCN respondents were female; 84% of RCM respondents were white and 10% black, Asian, minority ethnic (BAME); equivalent figures for RCN were 84% and 11% respectively. Ninety-three per cent of RCM respondents had trained as midwives in the UK; the figure for RCN respondents was 91%. Eighty-four per cent of the RCM rep respondents had been members for at least six years and almost 50% for at least 16 years. The figures for RCN were 83% and 57% respectively. Despite being longstanding members, 55% of RCM reps and 59% of RCN had been active (holding a workplace position) for only 0–3 years. The majority of respondents (59% of RCM and 70% of RCN) in the unions had no dependent children (under 16 years).
The complementarity of formal and informal aspects of social partnership
One of the most remarkable findings of the study is that the research participants predominantly described the management–union approach in their Trust as ‘partnership’, highlighting the often-smooth functioning of the existing joint consultation formal meetings. Interviewees gave many examples of the topics that are discussed during union–management joint meetings (JNCC) ranging from recruitment and staffing levels, health and safety issues, organizational changes to more ordinary, but sensitive, Trust policies (such as staff car park charges).
Recruitment, retention can be negotiated. We negotiate all our own policies. If you’d come in here yesterday, we had a table of policies like that. We were going through and saying they’re not getting away with putting that in there. And trying to keep the terms and conditions we’ve got that are better for our members than the national terms and conditions because if we can negotiate something better then we can use it. (Workplace rep, RCN)
However, as the composition and frequency of these consultative meetings are not imposed by any national policy, they depend on the robustness of local arrangements. Union regional officers who have a general overview of different Trusts reported significant differences in the implementation of social partnership policies depending on hospital managers’ preferences. For example, in some Trusts, health and safety reps were allowed to participate while in others they were not, which did not help their union influence.
So, there is no laid down mandate as to who should attend. Our broad recommendations are it should be the chief exec, director of HR, or equivalent, director of nursing, and the director of finance to either attend for the whole meeting or certainly to attend and give an update on the financial position of the Trust. They range from monthly to quarterly. It’s up to local bodies from both sides to decide how they operate and how frequently they meet. (Senior officer, RCN)
The other significant finding concerns the quality of the relationships between the different unions sitting on the various committees including staff-side. While in most cases, these relations were described as positive and constructive, which gave the unions some credibility vis-a-vis their employers, they were sometimes described as strained or competitive, especially between RCN and Unison that compete to recruit nurses (18% of RCN reps described the relationship with other unions as competitive, compared to 5% of RCM reps). Because of the small size of their union, some RCM reps also expressed some concerns about their lack of voice in large hospitals where general unions hold most of the seats on the JNCC.
We’re probably one of the smallest unions there. So that’s difficult. Also finding our voice and the way that they structure their JNCC or their joint negotiation committee, they almost have like an executive because they’ve got so many members and branch officers within Unison that they have an executive that then goes on to meet with the management side. (Workplace rep, RCM)
Moreover, some interviewees deplored the absence of some managers and HR during joint meetings – an issue that can be worsened if senior executives are absorbed by serious problems, be it financial difficulties directly linked to the austerity measures put in place since 2010 or other major organizational transformations. Such non-attendance was clearly associated with the constant restructuring of HR departments and their lack of resources, but also reflected union reps’ increasing lack of trust in HR, which is now seen as being disproportionately on the side of management.
I have a good working relationship with the head of HR and now he’s attending every single month, which is good, but we didn’t have that before. We’ve had a lot of change in HR management and directors and that’s not been easy because you’re constantly working with an interim and an interim only wants to do so much because they know they’re going so they’re not going to start any big projects. (Workplace rep, RCM)
Some interviewees also felt that the consultation exercise was rather a matter of box ticking, where all the important decisions had already been made.
Although the employers tend to make all the right noises about being pro-partnership working and promoting their JNCCs, there’s an awful lot of examples of when there isn’t partnership working and decisions are made and it is a bit of a tick box exercise, it’s on the agenda of the JNCC and it’s already been decided at executive level. (Focus group participant, RCN)
Despite these challenges, participation in staff-side and joint consultation committees was seen as an effective or quite effective strategy by at least 70% of survey respondents, both RCM and RCN. Union reps expressed their confidence in their ability to advance members’ demands in staff-side committees with 65% of RCM and 72% of RCN respondents describing themselves as confident or very confident. Numerous examples were also given of the critical support union structures provide to reps, in particular at RCN, which has a legacy of well-staffed regional offices (Kessler and Heron, 2001) that offer advice and frequently deputize for the union reps in staff-side meetings.
It’s a lot easier maybe for full-time officers to go in and really push a point and advocate very strongly on behalf of members whereas a rep or a steward understandably despite all the legal protection can feel very nervous of putting their head above a parapet and calling out the Trust for wrong or ill behaviour. (Senior officer, RCN)
Besides, these formal multi-union partnership arrangements are coupled with other more informal forms of regulation between senior managers (heads of nursing/midwifery) and RCN/RCM, usually at the level of regional directors or full-time officers. It is important to note that, in both unions, all the regional officers in charge of relations with employers and support for workplace reps are and must remain registered professionals, which means they must do a minimum amount of clinical practice per year.
I think we’ve got 27 directors of nursing, chief nurses for NHS Trusts in our region, I’ve met all of them. I go and see them all. They appreciate talking to nursing professionals about the issues that they’re dealing with. And not just table from big unions who don’t necessarily understand the nuances. And they have seen members of their staff getting really bad advice by UNISON or whoever because they’re not a nurse representing them. (Senior officer, RCN)
While these relationships are undoubtedly easier for regional officers who occasionally visit Trusts, they also exist at the level of workplace union reps who have regular meetings with their Head of department to exchange information, resolve any problems in a preventive manner or discuss the implications of national union campaigns or clinical changes.
Do you feel that your union role is valued by managers?
I think it’s a gradual thing. So, it’s not instant but after a while when they realize that you perhaps can resolve situations and help ease the situation which could become quite toxic then I find more people are coming my way now via advice from their manager to go and have a word with the union but it’s gradual, it is not instant. (Focus group participant, RCN)
Moreover, many Heads are also part of the same unions, especially in midwifery, which facilitates union–management relations, at least when it comes to professional/clinical issues.
And my Head of midwifery I meet with regularly, every six to eight weeks roughly. We just have a chat and if there’s any issues that are brewing I can kind of go to her and likewise she can come to me if I’ve heard anything. It’s a very good relationship. And she emails me things that might be coming up. (Focus group participant, RCM)
The mediating role of shared occupational identity
As expressed in the above excerpt, these informal relations are embedded within professional discussions, and most interviewees saw the dual role of their union as a major asset for maintaining unions’ credibility vis-a-vis management. Trade union demands in the workplace, including on staffing levels and low pay, are considered from the point of view of both the interests of professionals and the quality of service. Most union reps and officers interviewed were therefore of the opinion that the two aspects of their union role were complementary and helped them cultivate their legitimacy.
I think some people view trade unionists as people who are obstructive. We have to be cleverer than that. We have to work with the managers so that if you do that you get so much back. Once you get a good working relationship, it’s much smoother. And we can sort problems out very early. (Workplace rep, RCM)
This professional expertise also provides additional insights into the resolution of clinical incidents or capability issues, which can be discussed at Trust level in disciplinary panels.
The feedback that you might get from our heads of midwifery and HR directors that sit on disciplinary panels is that our approach to disciplinaries is maybe a little bit different to midwives who are represented by other trade unions. We come at it at a different angle because we are midwives, and we are on the NMC register. If a midwife has done something not quite right, we’ve got to say well, you didn’t really do a very good job that day but what was impacting on you that made you work completely out of character? (Senior officer, RCM)
However, the RCN/RCM dual role has also been described as a double-edged sword. While it allows a positive recognition of the contribution of the two unions by management, it encourages a more moderate stance, in comparison with other more vociferous unions, which may not always prove effective.
Management is more respectful. But is that from a paternalistic point of view as well because it’s a nice little . . . In our Trust, Unison have grown a huge voice on the staff side. When I go to the meeting to be honest, I feel very small. They have a forceful voice and there are quite a few of them who have been militant, and they’ve been in Unison for a very long time. They’re extremely experienced. They are very much listened to. (Focus group participant, RCM)
This double stance can on occasion give the impression that RCN and RCM are more on the side of management than on the side of their members.
I try and liken it to if you are a director of midwifery and today, I’m coming to talk to you about your service and your workforce and what’s happening around the region and they want to talk about what’s happening in midwifery at the moment and how you’re taking your service forward, that sort of conversation, that’s today. A very professional conversation. Tomorrow I am representing a member in a serious gross misconduct disciplinary, and I’ve got a completely different relationship with you. And it’s a very grown-up relationship to have and some of our reps find that difficult. (Senior officer, RCM)
It can also lead to some confusion of roles when union funds are used to improve service conditions that should be funded by Trusts. The fact that many stewards are part of middle management might tip the balance to the professional side at the expense of a more union approach.
Every year we do a cake sale, and we try and collect the money and the last couple of years we bought a cup chair so like birthing inflatable chairs. So, it’s something for our department. Last year from the money we raised and had in the pot, they bought special lights for each room. Right. So, this year I become the RCM rep, I said that’s enough, no more. And the suggestions from the RCM chairman [sic], she’s Band 7, was we spend it again on the department. I think that’s very unfair. (Workplace rep, RCM)
The function of stewards is inherently marked by role ambiguity which can make it stressful (Butler and Tregaskis, 2015; Harrisson et al., 2011). In fact, many interviewees described ‘walking a fine line’ in their attempt to build what was labelled by an RCM senior officer as a ‘grown-up relationship with management’. Nevertheless, being part of a professional union is seen as an asset by reps to assert their credibility vis-a-vis upper management and members. The performance of union duties is proving more difficult to get across to middle managers, who, like their colleagues, are experiencing the deleterious effects of austerity policies on staffing levels and work intensification; a context that is not conducive to the acceptance of time off for union activities and more generally the appreciation of union participation.
The impact of staffing issues on union operations and participation
A staffing crisis – with shortages throughout the NHS – is one of the most potent consequences of the austerity decade and one which has impacted hugely on union operations and participation. Union facility time – legally mandated paid time off to carry out union duties – has been squeezed in most Trusts. While most interviewees reported having access to time off to carry out their union activity, these are hours negotiated by mutual agreement with management, so they vary greatly from one Trust to another. What is ‘reasonable time’ to perform union duties may be subject to different interpretations, which in the context of high turnover in some hospitals is a problem as it requires union reps to provide evidence for obtaining these hours each time they have a new manager. Besides, as shown by the survey results, most RCN and RCM reps receive fewer than 10 hours of facility time per month, which is fewer than what they spend on their union work. These difficulties might explain the reluctance of some professionals to become a rep.
You do have facility time but there is no dedicated number of hours for the reps. You’re not told right, when you take up a representative position, you’ll have facility time and it will be 3 days a week or whatever it might be, there’s no set thing. So, I think people are reluctant to do it because they’re not sure what time they’re going to be given. (Workplace rep, RCM)
Even when they have an amenable manager who understands the value of their union role, a number of stewards or reps struggle to make use of their facility time because their schedules are so busy and the staffing level is insufficient, and they do not want to let down their already over-stretched colleagues.
I think there’s another problem that on the one hand, you could be active in the union and there’s good reasons to be, but then there’s the guilt, the guilt that you’re saying I need time off or you’re given time off but that will leave your colleagues short. So, there’s again this tussle between the theory and the practice. I don’t think we can ignore that because I think that is why people aren’t active, why people don’t do things. (Focus group participant, RCM)
Many stewards interviewed have therefore as their professional job a specialist or community role that allows them not to work shifts and to somewhat control their diaries, as well as to have access to phones and computers. Otherwise, several young reps working in wards with long and variable shifts expressed their wish to end their union role when they have a family.
It’s a very sad state of affairs but if anybody has been suggested as being a steward, one of my first questions is not what grade they are or what their name is, but where do they work. If I get told they work on delivery suite as a labour ward coordinator my heart drops because they’re not going to be able to be spared time off to go to meetings. Because they just are not going to be supernumerary, they’re not going to be surplus. Whereas if someone is a community midwife or they’re a specialist role midwife they’ve got slight control over their diaries. I think that’s where you can then jiggle things in the workplace to do things. Whereas if you’re working on the postnatal ward or the delivery suite, that is when you struggle. (Senior officer, RCM)
Work pressures and under-staffing also have repercussions for the propensity of reps to undertake union training and learn the necessary skills and confidence to engage in formal and informal partnership activities. Both unions have an extensive learning and development programme for reps and stewards which some find difficult to attend because of their professional constraints.
What I find in my area is it’s easy to recruit members, but we can’t retain them because they can’t get time off to go for their training or get involved. In the last few months, we have been heavily under-staffed, and we were overworked. So even when they got the package to read through, they said I haven’t even looked at it because I haven’t had time, I’ve worked five straight long days, I’ve worked four nights, I’m exhausted. So, with this case people are exhausted, they haven’t got time to put into RCN work and they won’t get time off from their employer to go for training. (Focus group participant, RCN)
While the resilience of workplace partnership within NHS Trusts can be explained by the existence of longstanding formal and informal arrangements between union reps and officers, HR managers and senior management, the tight staffing conditions that have worsened since the introduction of austerity measures in 2010 clearly jeopardize union reps’ ability to participate in workplace partnership actively and skilfully (also threatening the ability of trade unions to replace existing ageing unions reps).
Summary and conclusion
The purpose of this article was to investigate the prospects of workplace partnership for professional unions within the NHS context, while examining three propositions: first, the resilience of formal partnership arrangements has been conducive to the nurturing of high trust union–management relationships; second, shared occupational identity helps to facilitate these relationships; and thirdly, the deterioration of working conditions has a deleterious impact on the functioning of partnership arrangements. While the study displays some limitations as employers were not interviewed, we discussed those propositions using a mix of qualitative and quantitative data, investigating the views of RCN and RCM union reps and officers, in a large number of NHS workplaces. Beyond the NHS context and more generally, this study contributes to extant literature by providing original insights on the role of cultural and sociological aspects in the longevity of workplace partnership and by showing how the public sector, which is home to the rare examples of effective partnerships in the UK (Baccaro and Howell, 2017), is now facing the same economic challenges as the private sector (Martin, 2010), further risking to accentuate the trend towards decollectivized industrial relations.
First, the study underlines that the resilience of formal partnership structures over time has created a strong belief in the virtues of workplace partnership (Gahan and Pekarek, 2013), at least on the part of (professional) union representatives. While there are occasions where local managers (and HR departments) fail to engage in meaningful consultation, trivializing the consultation process by limiting discussion to relatively minor matters (Martin, 2010), the functioning of formal partnership seems to allow trade union involvement in decision-making and an overall feeling of openness in dealings between the parties. In this respect, the resilience of formal partnership practices has contributed to developing an organizational culture that promotes an ideologically cooperative relationship with employers and reduces the perception of conflicting interests between employer and employee (Kelly, 1996).
The robustness of workplace partnership in the context of the NHS can be explained by a combination of factors (Johnstone and Wilkinson, 2018), including high skill levels, strong unions with good reputation (Johnstone, 2015), (senior) management support, institutional provisions, and the separation of adversarial/distributive collective bargaining from integrative/consensual joint consultation activities (Butler et al., 2011). Moreover, studies within and beyond the specific context of the NHS have shown the role of workers’ preferences for cooperative rather than conflictual relations (Danford et al., 2014). Dean and Greene (2017) argue that ‘occupational ideology’ has an impact on members’ expectations, sometimes conflicting with union membership, but also on unions’ role as they have to work within the constraints of this occupational ideology, which may produce tolerance of disadvantage. Some professional occupations, including ones beyond healthcare, often female-dominated, have the characteristics of both recognition of poor conditions and satisfaction with aspects of their work, leading to ‘vocal tolerance’ (Dean and Greene, 2017).
That said, while an ideology of professionalism can discourage collective mobilization (Carter and Poynter, 1999; Danford et al., 2014), this study illustrates how professional work also facilitates the development of informal forms of regulation which complement formal and sometimes prescriptive forms of partnership (Upchurch et al., 2008). Previous research in healthcare has noted the role of senior managers/heads of nursing in developing extended involvement initiatives (Bach, 2004). Our study confirms the critical role of senior professionals, sometimes in their double capacity as manager and union rep, in the settlement of professional and trade union problems. This observation highlights the importance of the informal or ordinary dimensions of negotiation in professional environments, particularly in hospitals (Strauss et al., 1985), and the importance of shared occupational concerns in the shaping of smooth union–management relationships (Danford et al., 2014). Although sometimes amplifying stewards’ dual identification challenges (Butler and Tregaskis, 2015), this professional dimension is perceived as an asset by union reps and officers in their relations with management, while acting as a strong magnet to recruit members who are strongly attached to their professional value of putting ‘clients’ (here patients) first (Ackers, 2015; Danford et al., 2014; Kirton, 2018).
Despite these two positive points, the study emphasizes the profound impact of public sector austerity policies, particularly in terms of pressure on staffing and workloads, on the functioning of partnership arrangements, whether it is the resources dedicated to support services such as HR or the time available for union reps to participate and train. Previous studies identified middle- and line managers as among the potential obstacles to workers’ voice (Munro, 2002; Tailby et al., 2004; Upchurch et al., 2008), notably due to the intense work pressure and stress derived from the performance management regimes under which they are managed (Bach, 2004; Tailby et al., 2004). Our findings point to two other issues – intensified workforce shortage and high staff turnover in large hospitals, notably in London – that put line management under immense pressure. These challenges have the effect of making line managers not very accommodating when it comes to the management of absences, including union facility time. This lack of support for union work is problematic as the line management role is critical in bringing to life the values and principles of partnership (Geary and Trif, 2011). Moreover, this reluctance to accommodate union facility time adds to the guilt that reps have about putting in fewer hours of work when they know that their colleagues are overworked, thus contributing to making the performance of their union role morally difficult; a finding shared by previous studies carried out in feminized professions (Gavin et al., 2020; Kirton, 2018).
Lastly, previous research has shown the importance of employees’ perceptions of the distribution of partnership gains regarding their support for a continuation of a partnership approach (Geary and Trif, 2011). While the NHS can be seen as a sustainable case of union–management cooperation, this study also underlines the fragility of voluntary cooperation. As progress on pay rises, workload and staffing levels remains difficult and adversely affected by Brexit (not to mention the COVID-19 pandemic), front-line professionals may feel that the balance of benefits is too heavily weighted in favour of employers and therefore lose faith in the partnership approach (Danford et al., 2014; Upchurch et al., 2008). The preponderance of short-term financial concerns has been identified as a main issue for the maintenance of effective partnership (Simm, 2015) in the private sector. This study confirms that this has also become a challenge in the public sector (Guillaume and Kirton, 2017). In the NHS, as in other public services, the risks exist that workplace partnership is seen as a legitimization tool driven by government budgetary decisions, which is hardly compensated by union gains (Doherty and Erne, 2010). Moreover, as perceived benefits for employees are less evident, it may lead them to wonder whether institutional provisions only produce gains for the unions, without much impact on the improvement of employment and working conditions, ultimately undermining employees’ support for moderate unions. Professional unions, such as RCN and RCM, must therefore ‘walk a fine line’ in defining their future strategy, maintaining the gains from the long practice of ‘professional partnership’ (Ackers, 2015), particularly in their relations with government and NHS managers, and responding to the growing dissatisfaction of some of their members, some of whom might be tempted to ask for a change to a more militant strategy, as seen in other countries (Krachler et al., 2021).
Footnotes
Acknowledgements
We thank RCN and RCM for their collaboration with this research. We are also immensely grateful to all the officers, staff members and workplace reps who took part.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.