
Abstract
The late 1970s design for the Rosie Maternity Hospital on the Addenbrookes campus in Cambridge is a recurring type across the UK National Health Service, a framed three-storey courtyard configuration in brick masonry. It was selected as a case study project for the ‘Design and Delivery of Robust Hospitals in a Changing Climate’ project, pursuing the methodology developed for that research. Temperature data were collected in representative spaces within the hospital, over a two-year period. These revealed overheating in mild conditions relative to an observed 24℃ threshold for sleep but concealed within the customary 28℃ threshold marking the upper limit of acceptable conditions. The building was modelled using current climate data to predict 2010 conditions. The model was then calibrated against the observed 2010 data and used to predict the likely internal temperatures in current and 2030s. The results indicated an increase in peak temperatures. Four adaptive intervention schemes were subsequently developed: an ‘enlightened’ industry standard ‘Passivhaus’-type option providing superinsulation, sealed glazing and heat recovery; a lower technology-based scheme promoting natural cross-ventilation by providing greater opening glazing area, opening up the plan, sunshading and additional insulation; an enhanced natural ventilation scheme glazing over the courtyards to provide supply air winter gardens, and an advanced natural ventilation option pursuing passive downdraught cooling. All four schemes were modelled using the projected current and 2030s weather data and their performance was compared. The schemes were fully costed to yield relative ‘value for money’ guidance to National Health Service Trusts.
Introduction
From 2009 until 2013, the Design and Delivery of Robust Hospital Environments in a Changing Climate (DeDeRHECC) research project investigated the impact of summer overheating in the built estates of four National Health Service (NHS) Acute Trusts: Addenbrookes Hospital within the Cambridge University Hospitals NHS Foundation Trust; Bradford Royal Infirmary within the Bradford Teaching Hospitals NHS Foundation Trust; St. Albans City Hospital within the West Hertfordshire NHS Trust and Glenfield Hospital, a Nucleus scheme within the University Hospitals of Leicester NHS Trust. In each of these hospitals, 125 spaces within three to four wards in two or more buildings were monitored from June 2010. In Cambridge, the Addenbrookes Hospital ward tower and the Rosie Maternity Hospital were analysed. The performance of Addenbrookes tower has been presented elsewhere. 2 This paper focuses on the Rosie Maternity Hospital, representative of a recurrent 1970s NHS hospital-type building.
The Rosie hospital accommodates the maternity and neonatal services offered by the Cambridge University Hospitals NHS Foundation Trust in the East of England. 3 It was funded by a single private donation, designed by the architects Yorke Rosenberg and Mardell (YRM) in the late 1970s and opened in 1983. It comprises a steel and concrete-framed, brick-clad, three-storey, double-loaded corridor, double courtyard building. 4 Recently, as yet unpublished research, at Cambridge University for the Department of Health (DH) indicates the retention of some 117 postwar, three-storey, courtyard-type buildings across the NHS England Acute Estate, approximately 3 million m2 alone. YRM delivered the St. Thomas’s tower in Central London and the John Radcliffe Hospital in Oxford. The framed, repetitive bay, glazed treatment is consistent. Writing particularly of F. R. S. Yorke, YRM’S founder and an important publicist for modern architecture, Worsley wrote, ‘it was the rise of the Welfare State that made his firm’. 5 The ‘Rosie’ is a recognizably YRM design in the rigorous expression of its frame, ultimately a building system and aesthetic derived from Mies van der Rohe’s theoretical prewar schemes via Skidmore Owings and Merrill’s extensive output in North America, within which wide structural bays are entirely filled with glazing to a rectilinear grid. YRM’s tendency to clad their frames with ceramic tiles, as at St. Thomas’s in London, was overruled by the donor who insisted on brick and possibly also on the generous provision of opening glazing, which was suppressed in the late 1990s when urgent reactive NHS guidance suggested window opening be restrained to 100 mm. 6
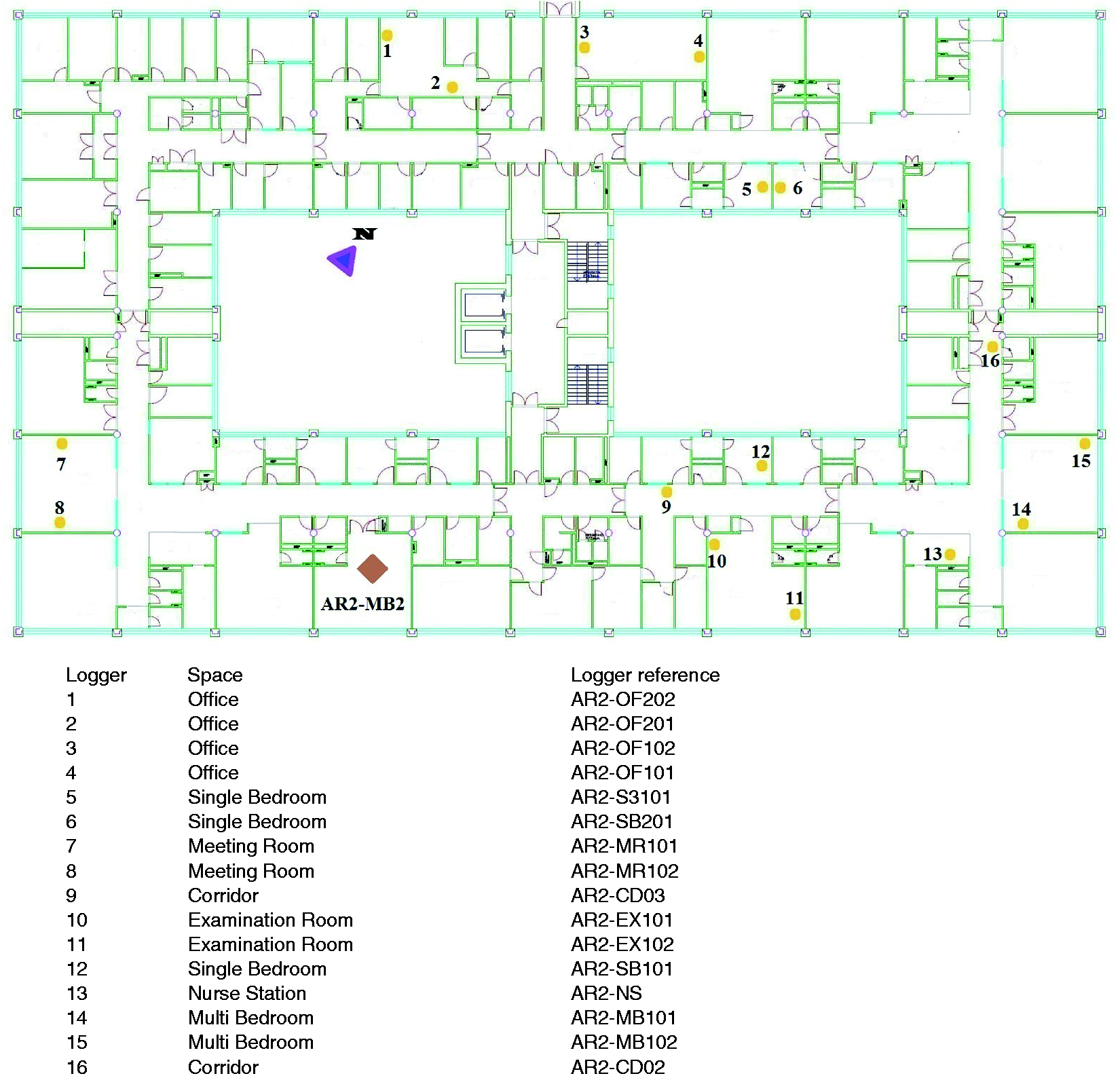
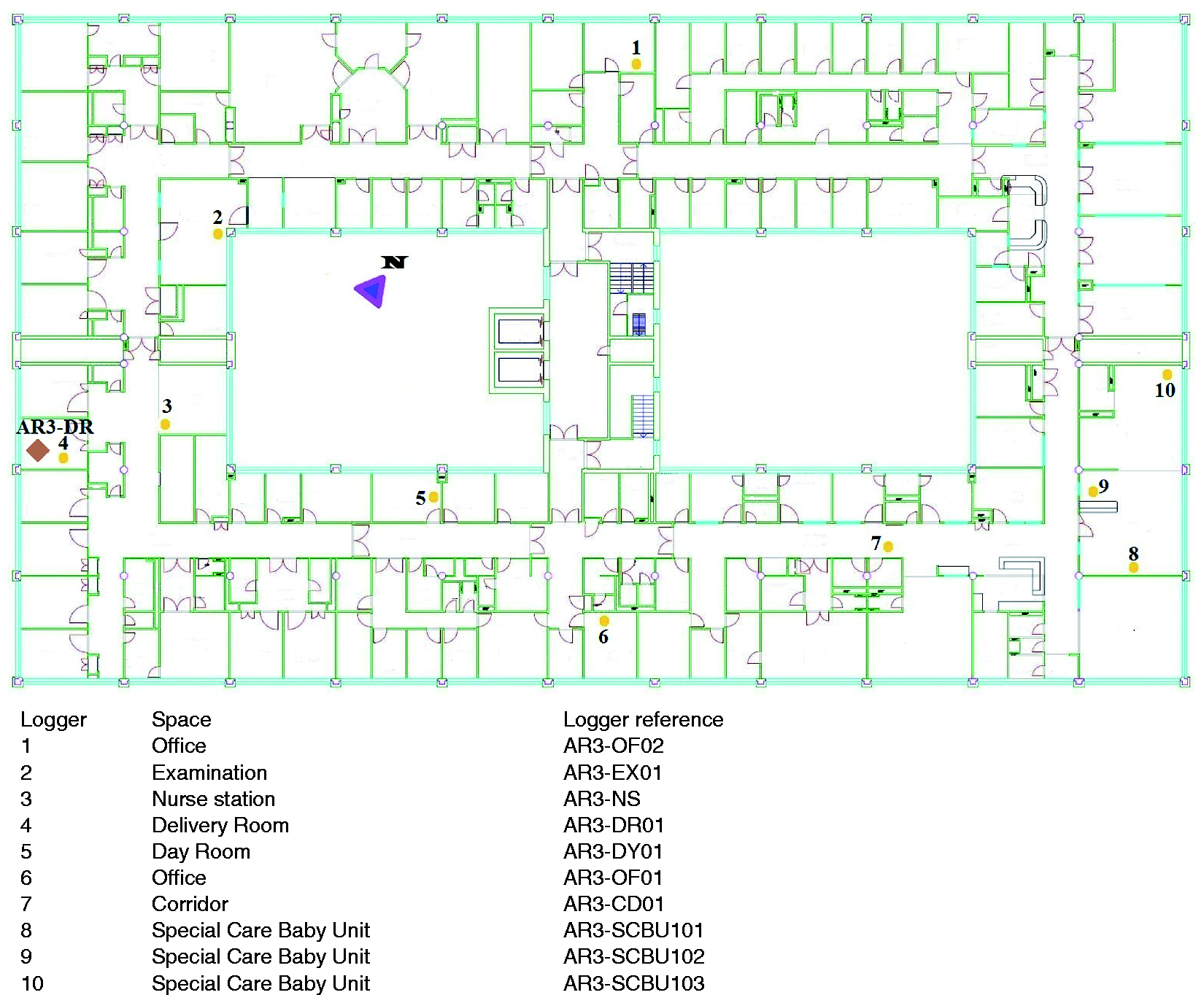
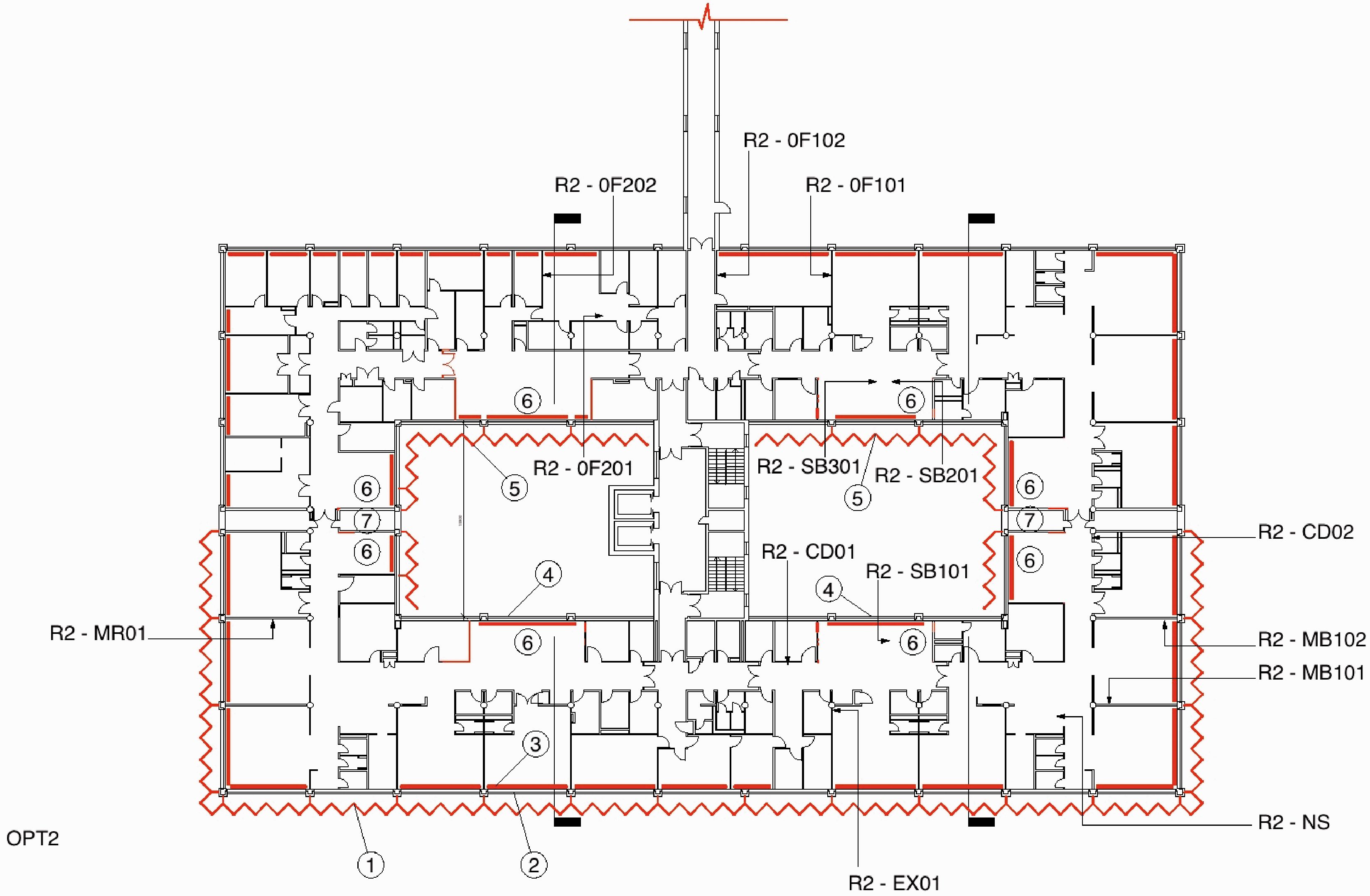
The building is oriented approximately east–west so that the main entrance and many of the multibed wards face south. Clinical services for outpatients examination, imaging and consulting rooms, are located on the level 1 (ground floor), whilst inpatient wards occupy second and the third levels. Figures 1–3 show general plan layouts with the location of data loggers installed by researchers. There are parallel academic and research functions, the Cambridge University Departments of Gynaecology and Obstetrics have accommodation in the northwest quadrant.
Monitored spaces and logger locations in Rosie level 1. AR1-EX was considered for predicted performance analysis (space with logger 5 and 6). Monitored spaces and logger locations in Rosie level 2. AR2-MB2 was considered for predicted performance analysis. Monitored spaces and logger locations in Rosie level 3. AR3-DR was considered for predicted performance analysis (space with logger 4).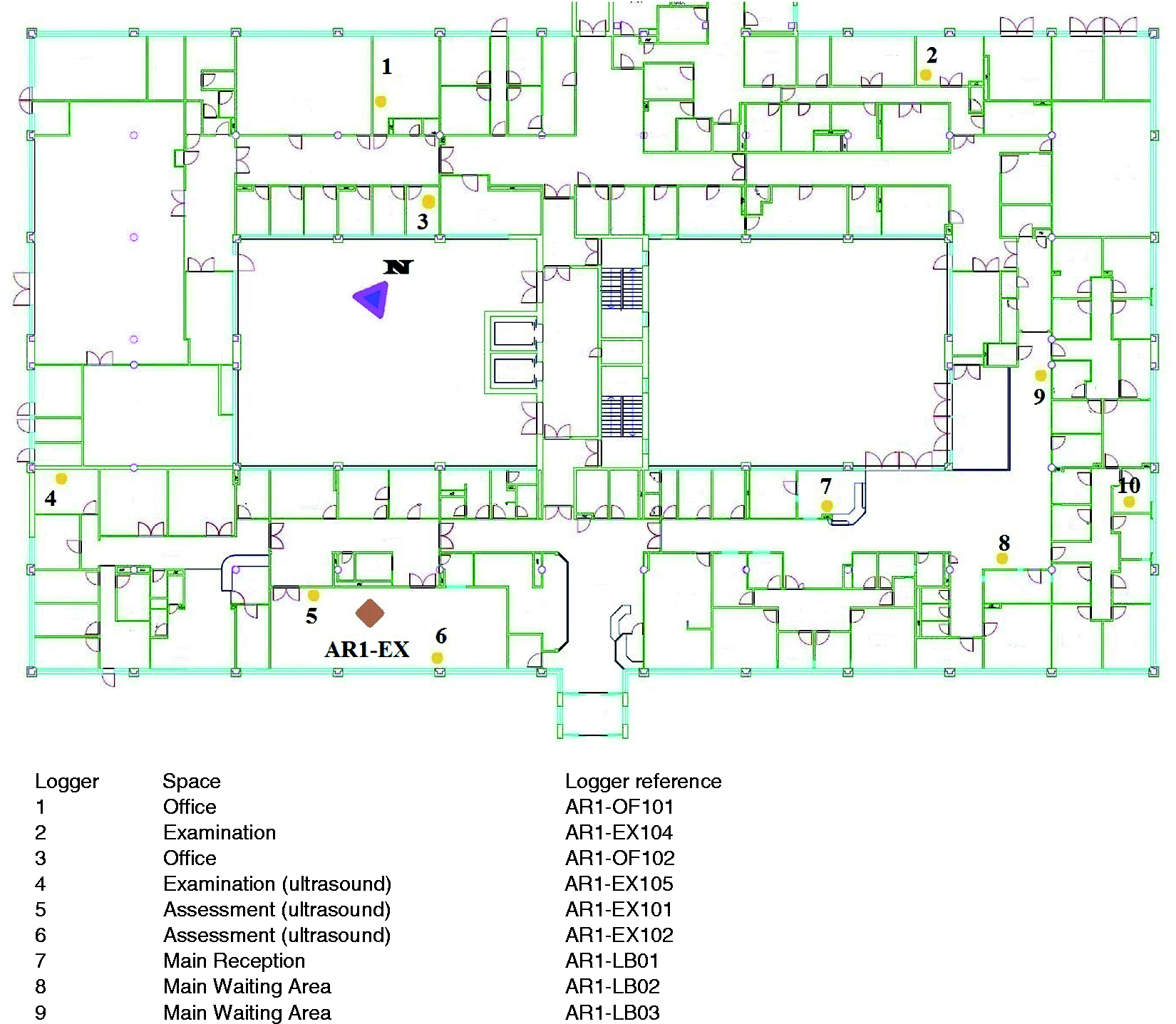
This paper investigates the performance of Rosie Maternity Hospital during summer 2010, and simulates the performance of adaptive interventions with a focus on summer time overheating. The study also costed all the schemes to yield relative ‘value for money’ guidance to NHS Trusts. The simulation weather files for the year 2010 (Bedford), current and future were created by the ‘Prometheus’ research team at Exeter University. The Bedford weather file was selected because the weather station at Cambridge does not measure all the necessary parameters to generate simulation weather files, especially the cloud cover and solar radiation intensity. The current Test Reference Year (TRY) and the Design Summer Year (DSY) were generated to the standard Chartered Institution of Building Services Engineers (CIBSE) methodology using weather data from the Bedford meteorological station. The TRY was created using 1980–2004 hourly weather data. The DSY was the year that had the third hottest summer between 1980 and 2004. In this case, it was 1997. For the year 2010 as well as for the current TRY and DSY, the diffused solar radiation, direct solar radiation and global solar radiation were derived from Bedford cloud cover as directed by CIBSE TM48. The future probabilistic weather files were derived using UKCP09 data for Cambridge under the A1B emission scenario. 7 The Prometheus team used a statistical technique to derive a single TRY and DSY for the future time slice. This work used 50 and 90 percentile weather files to generate the TRY and DSY, respectively. A detailed account of the weather file generation and selection process has been presented elsewhere. 8
Construction of the Rosie hospital
Figures 1–3 record the three floor plans of the hospital, Figures 4 and 5 show the frame structure. Table 1 summarises the use of materials.
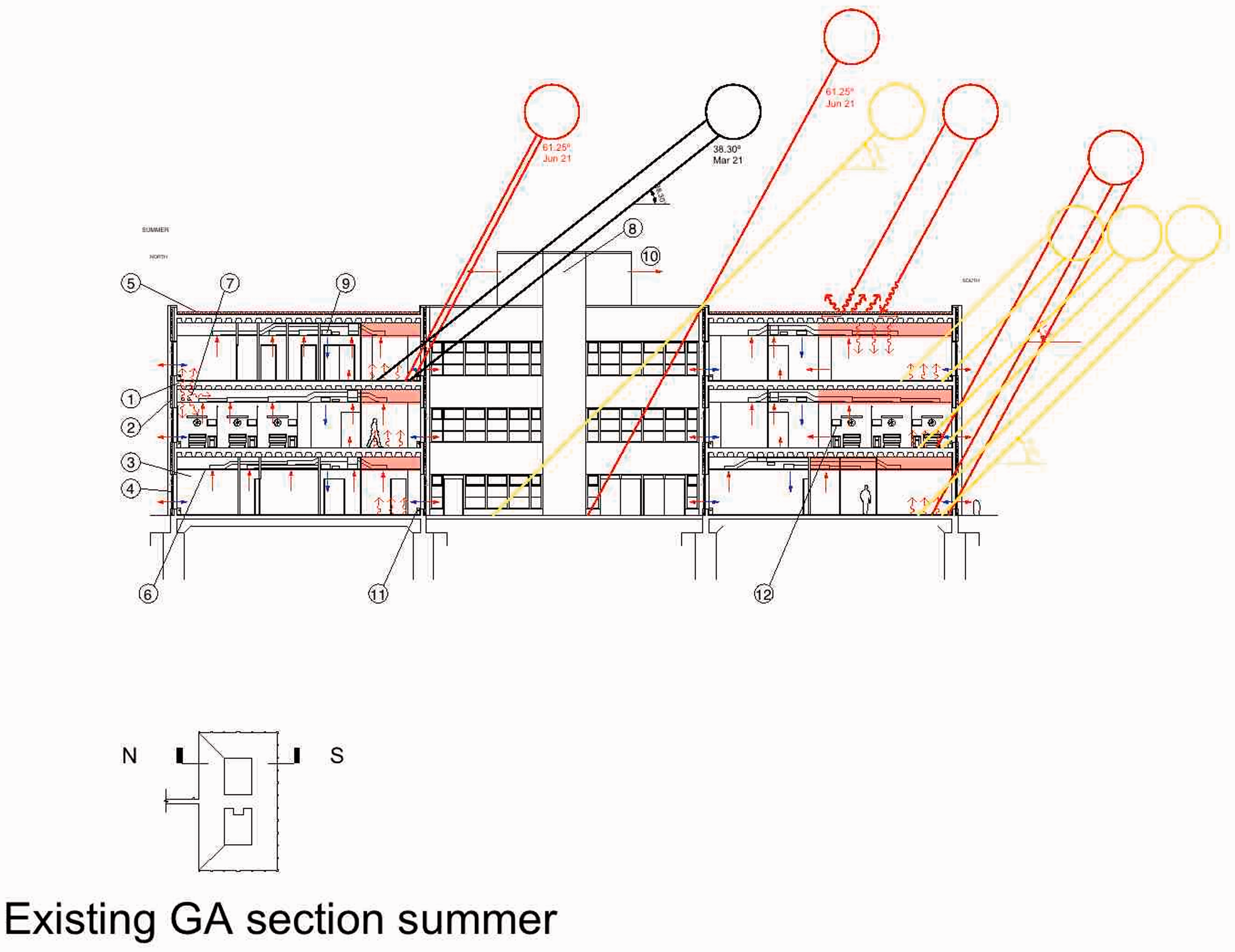
The Rosie Maternity Hospital, Addenbrookes, Cambridge. Existing Building, Summer Condition. The Rosie Maternity Hospital, Addenbrookes, Cambridge Existing Building, Winter Condition. General construction information for the Rosie maternity ward complex. Note: RC, reinforced concrete.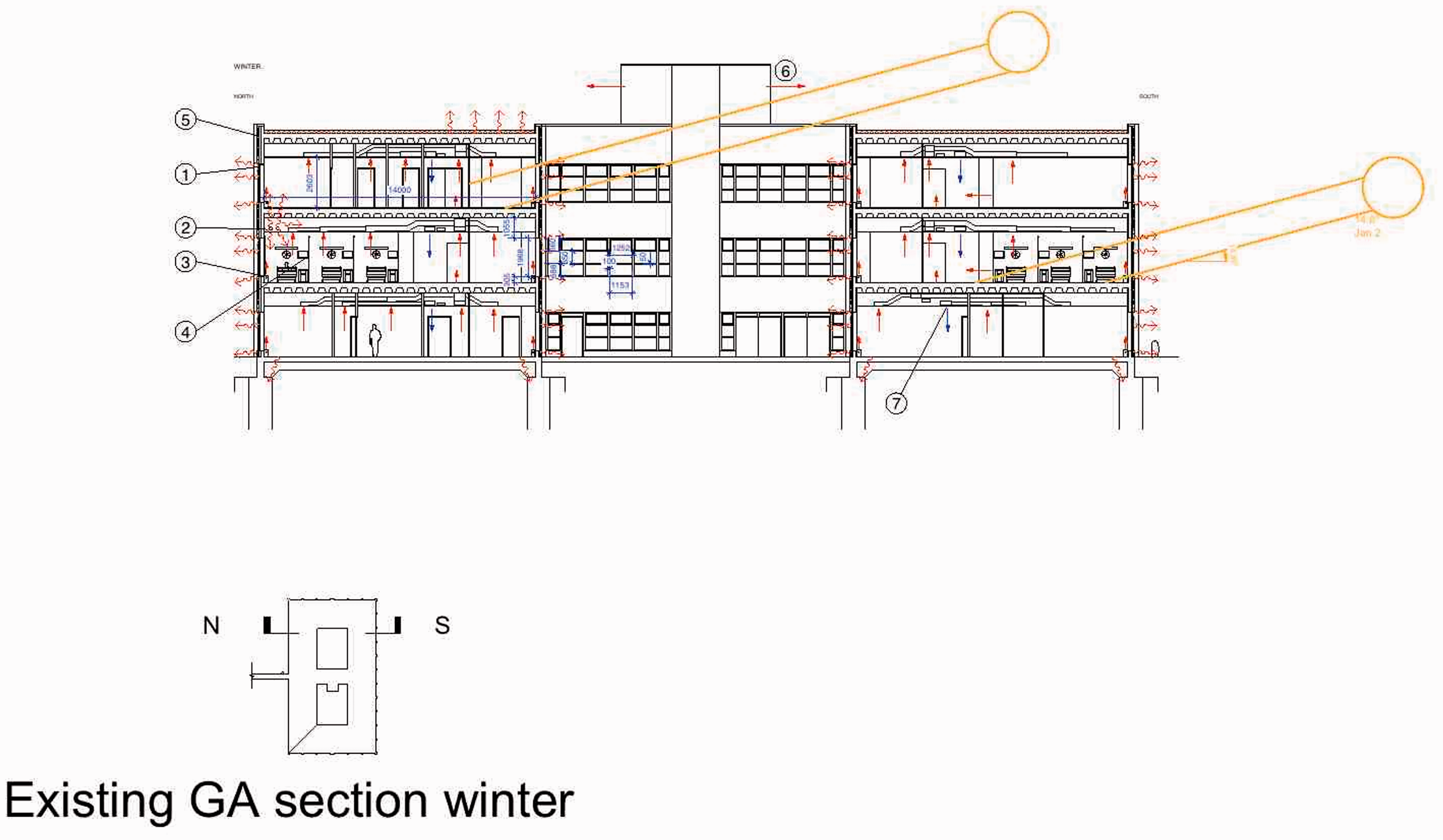
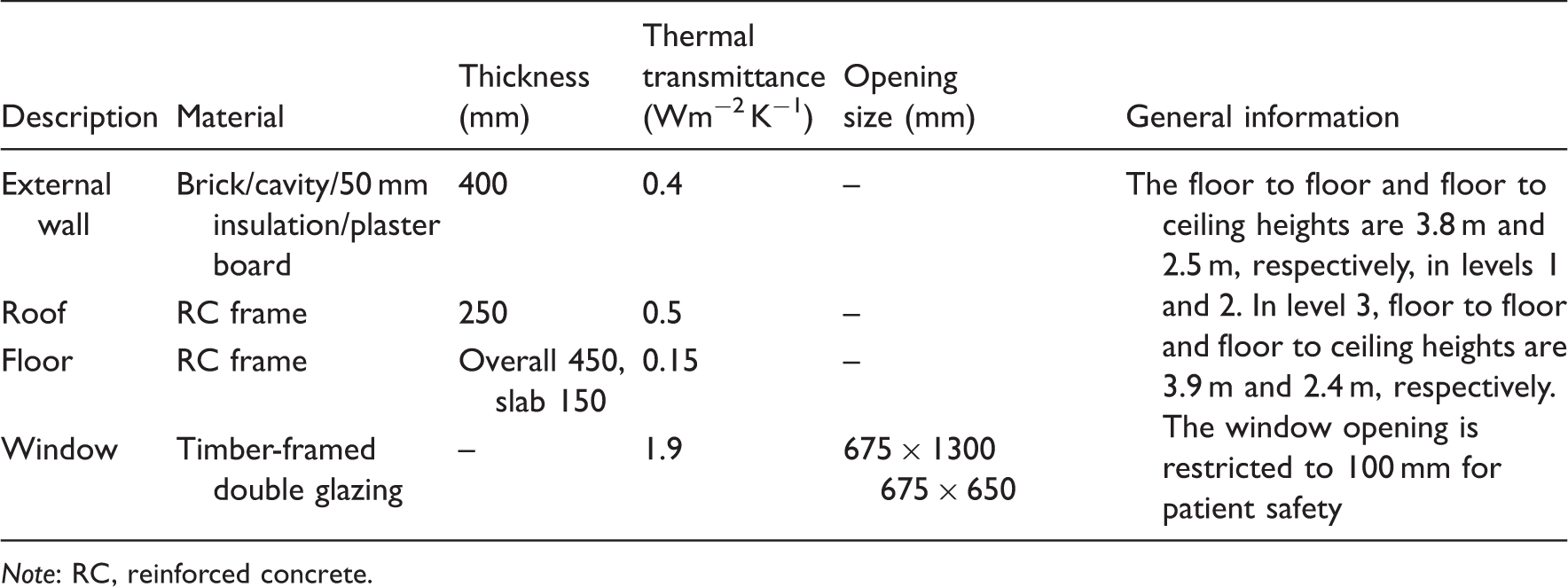
Floor and roof slabs are coffered ‘waffle’ type reinforced concrete slabs of 150 mm continuous slab depth with two way beams adding 300 mm depth, 450 mm overall incorporating substantial thermal mass, spanning across a steel frame. Deep perimeter downstands to the floor and roof slabs form lintols to the wide bays. The roof buildup comprises screed to falls, asphalt, 50 mm ‘Roofmate’ extruded polystyrene slabs, held below a 50 mm thick roof deck of prescreeded woodwool slabs with reinforced edges and 50 mm thick layer of washed gravel (20–50 mm diameter).
Suspended ceilings conceal all spanning concrete from the occupied spaces, suppressing radiant exchange with the occupants. The conventional cavity external wall construction comprises: 100 mm brick; 50 mm thick polystyrene partial cavity fill; the inner leaf either 140 mm block or plaster board on timber (100 mm × 100 mm) studwork; the floors screeded and finished with vinyl carpet. The rectilinear grid of windows in each structural bay is double glazed in hardwood frames (approximately 75 mm × 100 mm). Hot water and mains steam pipelines are suspended below the floor slabs retaining their original insulation at the time of this study, some of which is missing. The steam pipe, the main ring supplying the whole site, emitted heat continuously into the Level 2 ceiling void on the north side of the building. Recently the DH NHS Energy Efficiency Fund (EEF), administered by the lead author, has funded its reinsulation and the removal of asbestos lagging. 9
Arrangement of existing services
All spaces have perimeter heating elements without local thermostatic control, set within each bay below the extensive glazing, fed by supply and return pipes rising through the floor slab below, hot water reaching the perimeter radiators intended to be not less than 65℃, to maintain 24–25℃ in occupied rooms year round. The building is currently operated at a set point temperature of 24.0℃. Mechanical ventilation heats supply air at temperatures below 22℃ all year round. At the time of monitoring, there was no zone control. However, the Trust’s Estate Management was planning to introduce Thermostatic Radiator Valve (TRVs). The researchers’ expert panel observed that zone control employing wall-mounted thermostats would be more productive and efficient. 10 The Rosie hospital has its own plant room on level 1 of the west wing with four noncondensing duel fuel boilers, gas fired in normal mode. They supply hot water to the main header maintained at 60 and 70℃, respectively, in summer and winter temperature. The boilers come to operation in sequence during colder conditions to supplement heat provided by central steam plant supplying the whole site. The plant on site includes two shell–core heat exchangers to extract heat from the steam supplied from the central plant. The original exchangers are scheduled to be replaced by plate exchangers. Pumps work on constant volume and variable temperature.
The building has its own chiller providing chilled water to an air-handling unit (AHU) delivering comfort cooling to intensive care units and the operating theatres. The chiller set point temperature is 6℃. Standby mode set point is 9–10℃. When the chiller is not supplying chilled water to the cooling circuit, the temperature is set at 12℃.
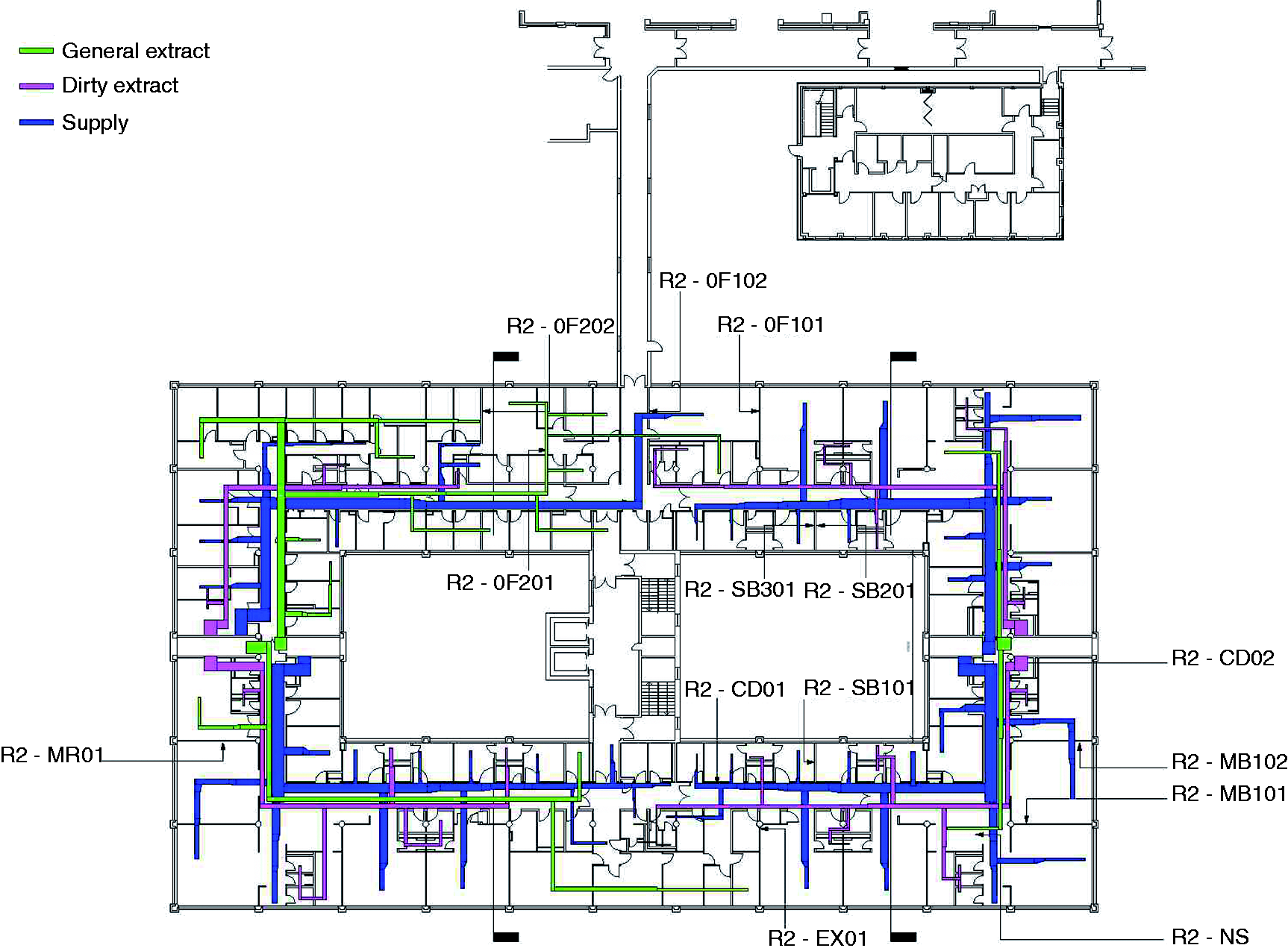
The building is mechanically ventilated throughout the year. Figures 4 and 5 show the supply and exhaust points, corridor pressurized by supply, exhaust above patient beds. For ventilation, the building is zoned into east and west wings with an AHU room located on each side. Each plant room contains three AHU units and in each room only one unit has the provision to cool the air (the other two are only for heating). Fresh air to these AHUs is drawn from above roof level through ducts. Generally, when the outside air temperature is 22℃ or above the fresh air is not conditioned (no heating) and it is directly supplied, but cooling is produced for special rooms such as the Special Care Baby Unit. The AHUs release the conditioned air at 21℃ through variable speed fans. Fresh air is heated to 18℃ and supplied to each zone via corridor ceiling supply grilles located. Anticipated maximum supplied air temperature is around 26℃ in summer. In the winter, it could fall as low as 18℃. At night, level 1 has reduced air supply due to low occupancy.
Extracts are located in service spaces, WCs, bathrooms and dirty utility rooms and in wards above beds. The centrally collected return air is released directly to the atmosphere above roof level with no heat recovery.
Performance of monitored spaces
Twenty-six spaces on three levels were monitored at hourly intervals with Hobo U2 temperature loggers. 11 The larger spaces receive more than one logger (Figures 1–3). The logger positions were constrained as NHS infection control protocols resist foreign objects appearing in clinical spaces. Specific ventilation rates were recorded using a Balometer on a typical working weekday during January 2012.
The second level emerges as the hottest floor and AR2-SB2 (logger AR2-SB201) records the hottest space (Figure 6).
12
Recorded Rosie level 2 internal and ambient dry-bulb temperature and solar radiation intensity.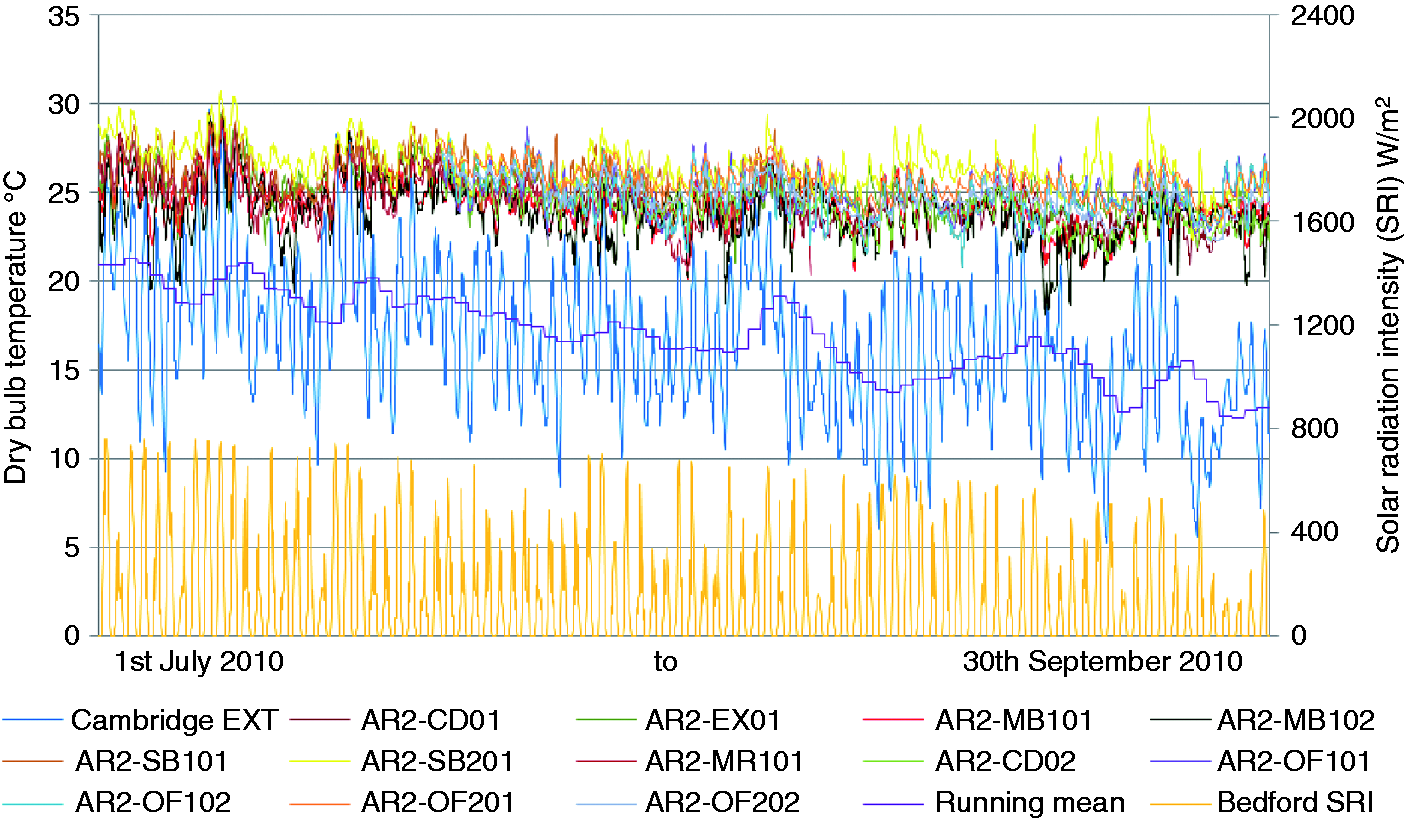
Multizone base model characteristics: selected spaces.
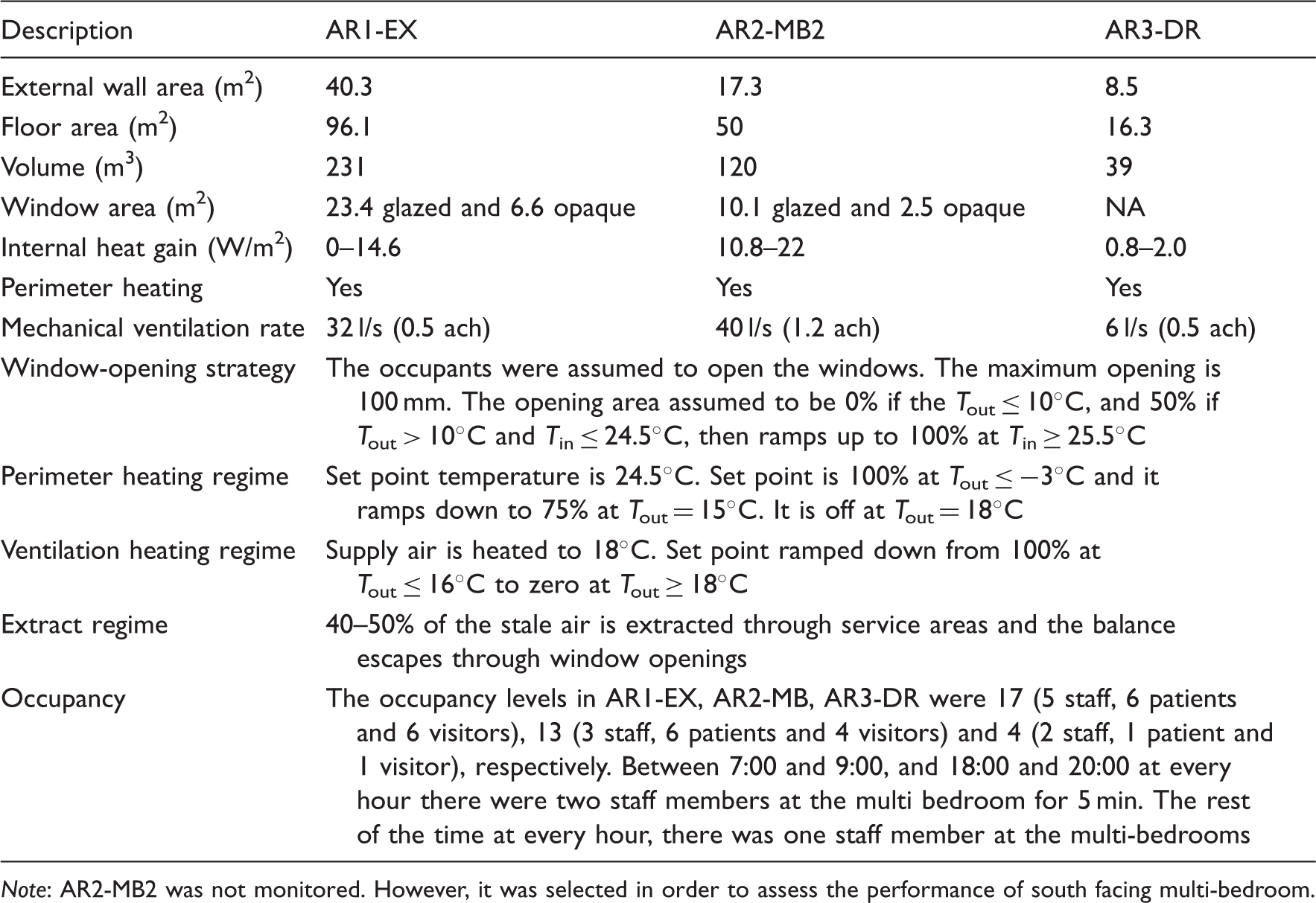
Note: AR2-MB2 was not monitored. However, it was selected in order to assess the performance of south facing multi-bedroom.
Comparison of internal temperatures measured between 1st July and 30th September, 2010, with BSEN15251, CIBSE and HTM03 overheating criteria: Representative spaces in Rosie maternity ward.
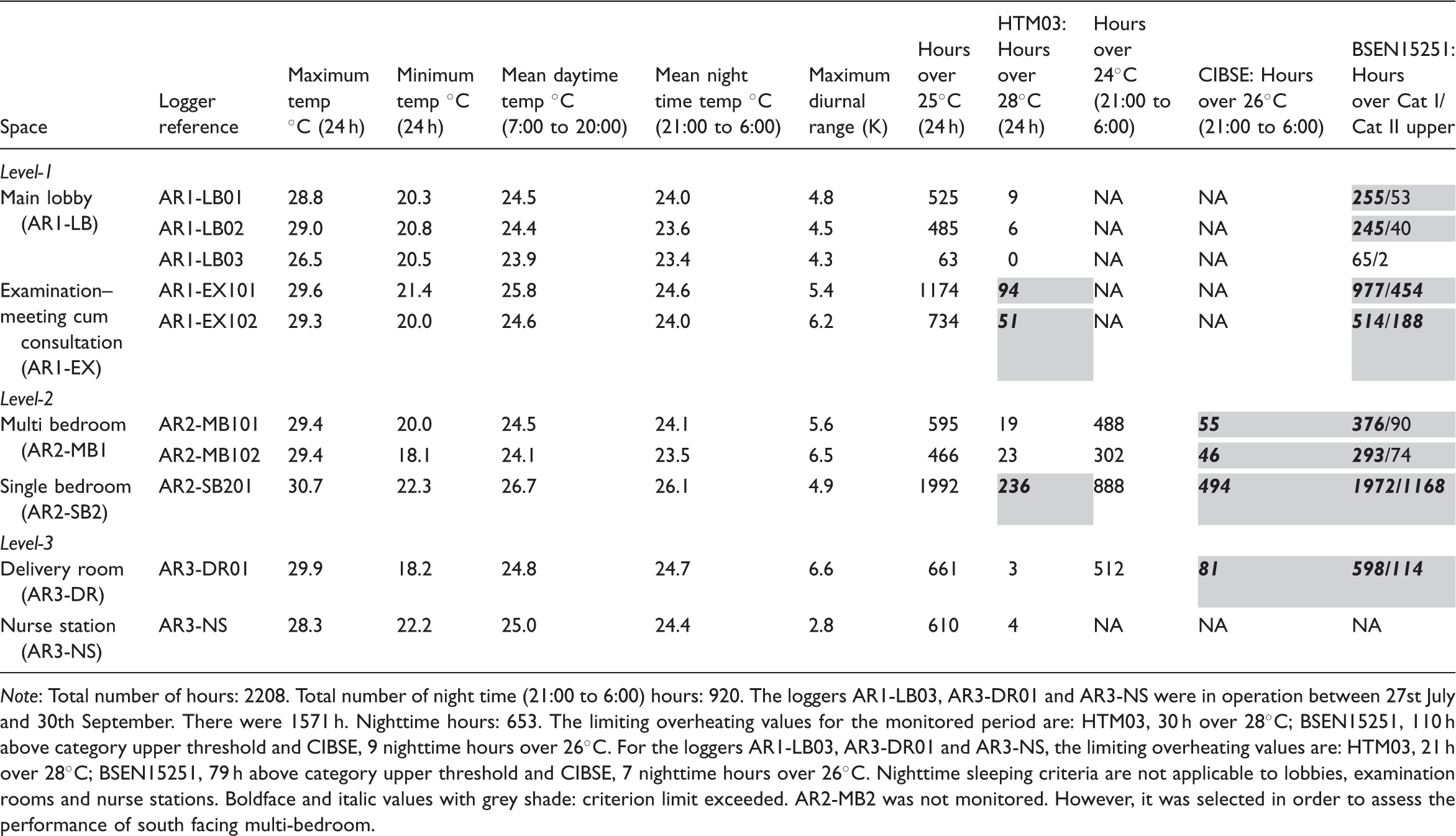
Note: Total number of hours: 2208. Total number of night time (21:00 to 6:00) hours: 920. The loggers AR1-LB03, AR3-DR01 and AR3-NS were in operation between 27st July and 30th September. There were 1571 h. Nighttime hours: 653. The limiting overheating values for the monitored period are: HTM03, 30 h over 28℃; BSEN15251, 110 h above category upper threshold and CIBSE, 9 nighttime hours over 26℃. For the loggers AR1-LB03, AR3-DR01 and AR3-NS, the limiting overheating values are: HTM03, 21 h over 28℃; BSEN15251, 79 h above category upper threshold and CIBSE, 7 nighttime hours over 26℃. Nighttime sleeping criteria are not applicable to lobbies, examination rooms and nurse stations. Boldface and italic values with grey shade: criterion limit exceeded. AR2-MB2 was not monitored. However, it was selected in order to assess the performance of south facing multi-bedroom.
Comparison of internal temperatures measured between 1st May and 30th September, 2011, with BSEN15251, CIBSE and HTM03 overheating criteria: Representative spaces in Rosie maternity ward.
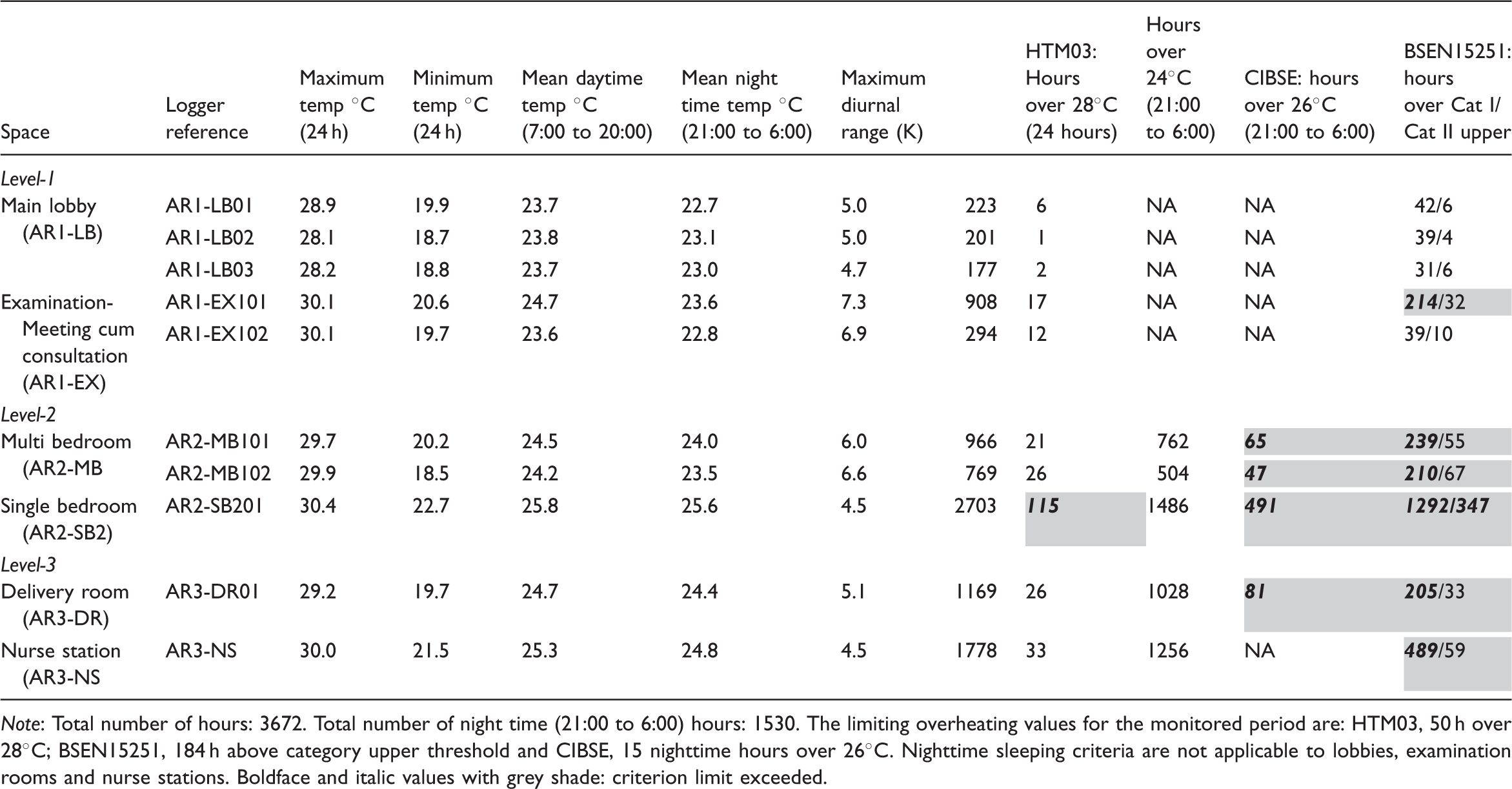
Note: Total number of hours: 3672. Total number of night time (21:00 to 6:00) hours: 1530. The limiting overheating values for the monitored period are: HTM03, 50 h over 28℃; BSEN15251, 184 h above category upper threshold and CIBSE, 15 nighttime hours over 26℃. Nighttime sleeping criteria are not applicable to lobbies, examination rooms and nurse stations. Boldface and italic values with grey shade: criterion limit exceeded.
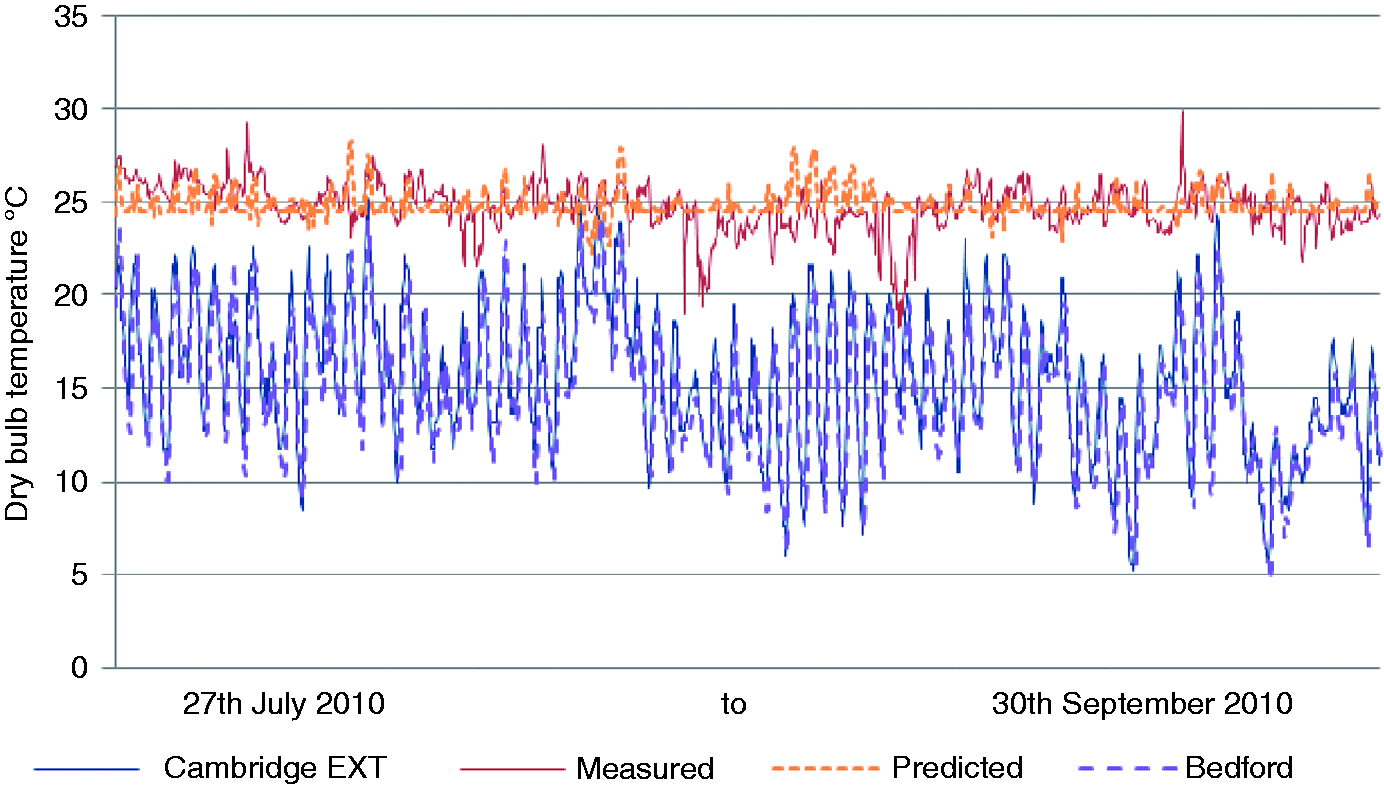
The spaces were monitored from July 2010 to October 2011. The focus of the DeDeRHECC research project is on resilience to summer overheating and so results for the consecutive summer periods 1st July to 30th September 2010 and 1st May to 30th September 2011 are presented (Tables 3 and 4). Analysis will focus on 2010 results insofar as calibration of the dynamic thermal model, the predictions it generated and the subsequent energy calculations are based on the 2010 Bedford weather file as described later in the paper.
To evaluate the monitored performance, the study used the ambient temperature from Cambridge University and solar radiation intensity from the Bedford meteorological station. The maximum ambient temperature during the summers of 2010 and 2011 were 29.6℃ and 31.2℃ respectively, 2010 was a relatively cool year, while the minimum temperatures for summer 2010 and 2011 were 5.2℃ and 3.5℃, respectively. The peak solar radiation intensity for 2010 and 2011 was of the order of 750 W/m2 and 950 W/m2, respectively, for the monitored periods.
During the period 1st July to 30th September 2010, the maximum temperature recorded in the building was 30.7℃ observed in the single patient bedroom (AR2-SB2). This trend was also observed during summer 2011. During the 2010 monitored period, a minimum temperature of 20.3℃ was found in the Lobby area and this trend repeated in 2011. For the 2010 monitored period, the mean daytime temperature varied between 23.9℃ and 26.7℃, while mean nighttime temperatures varied between 23.4℃ and 26.1℃. The single bedroom (AR-SB2) experienced the maximum temperature conditions recorded. The lowest diurnal temperature range, 2.8 K, was recorded in the nurse station (AR3-NS) and the highest, 6.6 K, in the delivery room AR3-DR.
Thermal comfort was determined by comparing the measured temperatures with the criteria adopted in previous papers by the authors. 13 These included both the simple static guidelines and criteria described by the CIBSE and the adaptive thermal comfort thresholds described in BSEN15251. The appropriateness of these approaches and their relative credibility are discussed by Lomas and Giridharan. 14 The static criteria suggest that thermal discomfort will arise if there are more than 5% of the annual occupied hours over 25℃ or more than 1% of annual occupied hours over 28℃ in occupied spaces. The research team assumed throughout the DeDeRHECC project that hospital wards are occupied for 24 h a day every day of the year, with the exception of the lobby, consulting and examination rooms.
The latter criterion is given in Healthcare Technical Memorandum HTM03. 15 The CIBSE Guide also indicates that sleep will be impaired if temperatures exceed 24℃ and that they should not exceed 26℃. However, the nighttime overheating risk criterion indicates that temperatures should not exceed 26℃ for 1% of the occupied hours. Nighttime was taken as 21:00 to 06:00 throughout the DeDeRHECC project. The BSEN15251 thresholds increase as the ambient air temperature increases; a narrow band of acceptability, Category one (Cat.I) which is 5 K wide, and a wider band, Cat.II of 7 K, are of interest here.
In 2010, the single bedroom (AR2-SB2) and examination room (AR1-EX1) exceeded both BSEN15251 and HTM03 thresholds. 16
The multi-bedroom ward and delivery room exceeded only the CIBSE criterion. None of the spaces met the adaptive comfort standard Cat.I. 17 However, the examination room (taking the average value of two loggers) and the lobby met the Cat.I threshold during 2011. On the other hand, during 2011, only the single bedroom (AR2-SB2) exceeded the HTM03 threshold. In 2010, most of the spaces were monitored for 2208 h, however the number of hours crossing the threshold is close to, or higher than 2011 values, especially in terms of the BSEN15251 thresholds. On the other hand, the number of hours of ambient temperature over 24℃ during 2010 (2028 h) and 2011 (3672 h) was 82 and 96, respectively. Therefore, better performance in 2011 can be attributed to milder summer conditions. However, in general, the 2010 summer has been considered as mild summer, not taxing conditions. 18 Therefore, these results indicate that summer overheating even in mild ‘normal’ conditions in the Rosie hospital is a major concern.
Overheating has been highlighted by hospital staff on many occasions during the researchers’ visits to Rosie Maternity Hospital. Excessive temperatures have been recorded by the DeDeRHECC team in the Bradford Royal Infirmary and the Edinburgh Evening News reported ‘Soaring heat at maternity ward “intolerable”’ in its 24th July 2014 issue.
Figure 4 depicts the winter mode in which unintended air infiltration through the envelope and fabric heat losses do not appear to dispel the significant internal heat gains. Mechanical ventilation delivers warmed air to achieve the set point temperature and perimeter skirting heating attempts to counter the prodigious cold down-draughting off the glazing.
The fundamental factors contributing to the poor summer time resilience are indicated in Figure 5. Hot water and steam pipes with intermittent insulation contribute to significant internal heat gains from lighting and equipment. The diagram reveals the extent of the exposure of direct solar gains through the liberal glazing area, which is largely fixed but with an intermediate band of lights opening to only 100 mm. This explains the marginal thermal comfort generated on even mild days in south and south westerly facing wards as shown in Figure 5.
Predicted performance of the existing building: Modelling and calibration
To predict the annual frequency of overheating of the wards and the energy demands and CO2 emissions in the current climate, the dynamic thermal model Integrated Environmental Solutions (IES) was used. 19 This software was chosen because it is widely used by UK building engineering consultancy firms including partners in the ‘DeDeRHECC’ project. Its application to the refurbishment of hospitals would thus meet with general understanding and interest in the industry. Since measured temperatures were available, it was possible to calibrate the IES model prior to embarking on the assessment of the proposed refurbishment options.
A multizone thermal dynamic model of the Western wing of the Rosie hospital was constructed to predict current and future performance. The measured hours over 28℃ was taken as the primary criterion to be matched by the predictions. Table 2 records the construction information on which the model was run. The calibration was carried out by focusing on two spaces; AR1-EX and AR3-DR (Figures 7–9).
Comparison of predicted and measured temperatures for AR1-EX, and ambient temperature, during the monitored period. Comparison of predicted and measured temperatures for AR3-DR, and ambient temperature, during the monitored period. Option 1 SMVHC.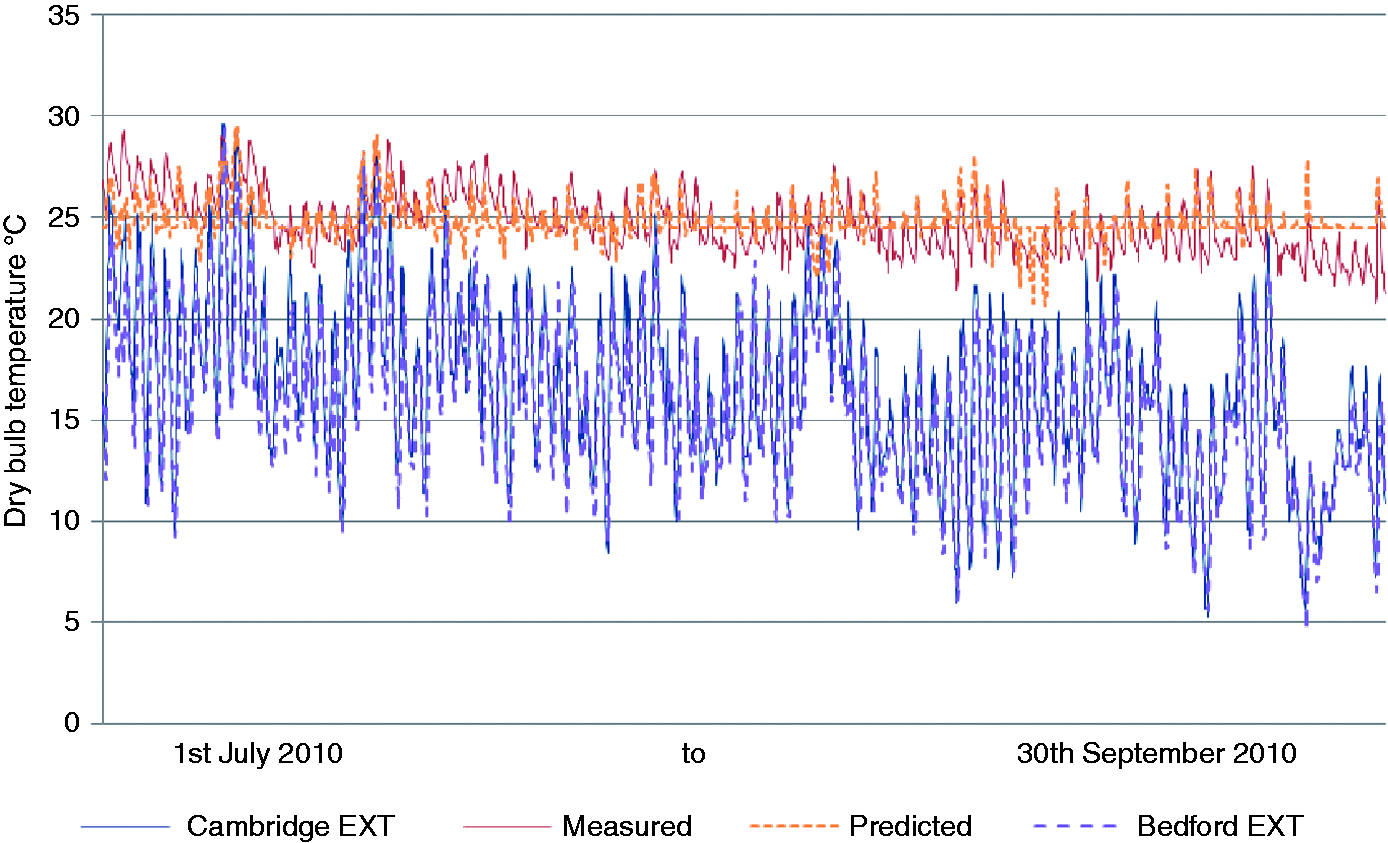
The weather file for Bedford in 2010 was used for the calibration, as described elsewhere. 20
Sensitivity analysis was carried out to identify the critical variables necessary to tune the model. The model is sensitive to internal gains, especially heat gains from the equipment, the degree and duration of both window and door opening in all the rooms.
At night, the model assumes that in any 1 h, 50% of the doors were opened for 5 min in discussion with nursing staff. The window-opening regime (see Table 2) is one of the most uncertain assumptions but is very critical, especially in making nighttime predictions.
Entry onto wards for researchers was limited to brief forays to install or collect data loggers and on some days forbidden outright. The model cannot accurately reflect an individual’s preferences, i.e. the window-opening regime will not change in line with each and every occupant decision, but it is not clear how autonomous inpatients and their visitors may be in practice. Therefore, the model used a generalised window-opening profile that researchers believe to reasonably reflect the overall trend in the ward from limited accounts by nurses and spot observations of the exterior elevations (see Table 2).
Experiments have shown that the largest difference between measured data and predictions occur during periods of high solar radiation intensity (solar gain) and high airflow rate. The deviations during high solar radiation intensity could be attributed to the weather file used for the simulation i.e. in real situation; solar radiation intensity could have been less than that in the constructed Bedford simulation weather file. The model takes into account shading by the building to the west but not winter morning shading from the east. Overall, the deviations of the predicted temperatures during high solar radiation intensity are not significant. The model-predicted temperatures were not very sensitive to the prevailing mechanical ventilation rate, but were sensitive to high natural ventilation rates via windows.
Comparison of measured and predicted results of three monitored spaces for the calibration period.
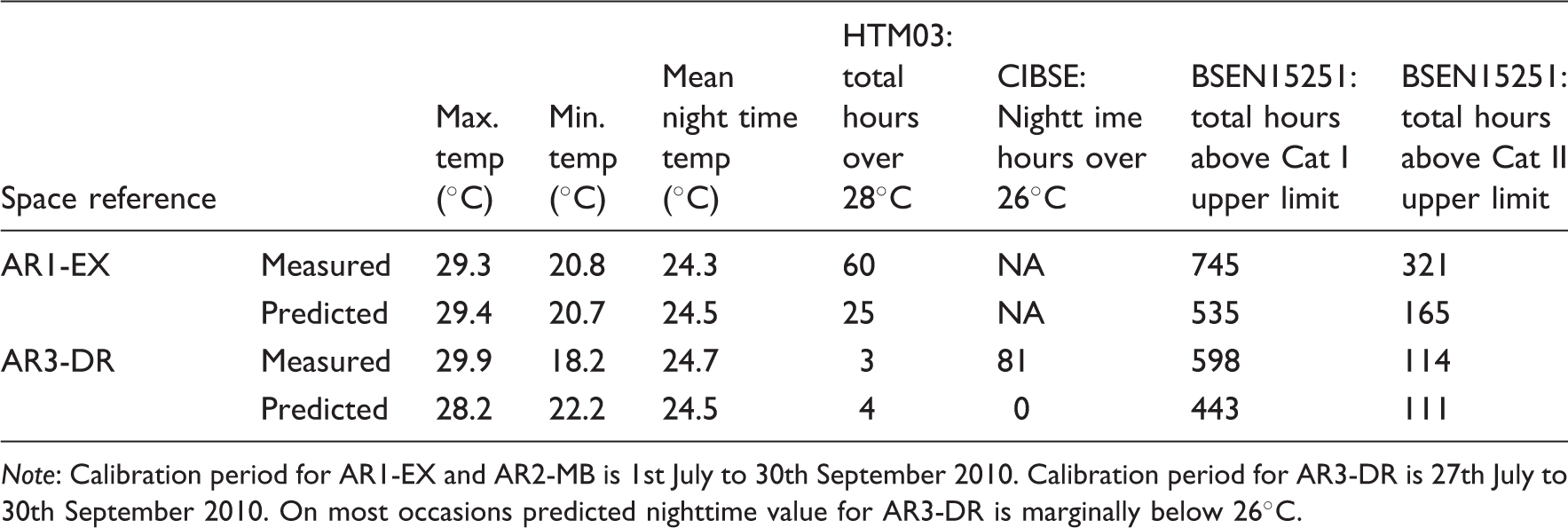
Note: Calibration period for AR1-EX and AR2-MB is 1st July to 30th September 2010. Calibration period for AR3-DR is 27th July to 30th September 2010. On most occasions predicted nighttime value for AR3-DR is marginally below 26℃.
The mean nighttime temperature shows a good agreement with the measured values for both the spaces (Table 5). The deviation in HTM03 value is slightly high in AR1-EX. This is largely due to limitations in the schedules.
The NHS annual Heatwave Plan, released when DH determines external temperatures have reached a predetermined limit. The criterion for implementation varies across the country, being higher in the southeast to acknowledge adaptation to the prevailing heat island. The effectiveness of what are emergency short-term measures has been found to be affected by behaviours and understanding. 22 The building clearly requires longer term intervention to deliver greater resilience to current and future summertime overheating.
Four adaptation refurbishment options
Schemes to deliver greater resilience to hot summers were devised, commencing with what appears to have become the ‘enlightened’ industry standard ‘Passivhaus’ model adapted to the scale of the nondomestic building, a superinsulated envelope coupled with a rigorously controlled mechanical ventilation regime with efficient heat recovery, through lower technology, perhaps more conventional, cross-ventilated schemes to atrium-type solutions providing an air supply winter garden and in the final option, a relatively very low energy form of gravity-driven cooling.
Option 1, SMVHC: sealed mechanical ventilation heating and cooling (see Figures 9 and 10), proposes all glazing is sealed, airtightness improved as far as practicable, 100 mm insulation added to the roof and, through an overcladding insulation and render system, to the external walls. Mechanical ventilation is operated to achieve the unqualified DH recommendation of 6 ach with 60% heat recovery. Figure 10 shows the basic duct layout. Air cannot be recirculated within UK hospital wards.
Option 1 basic mechanical ventilation arrangement.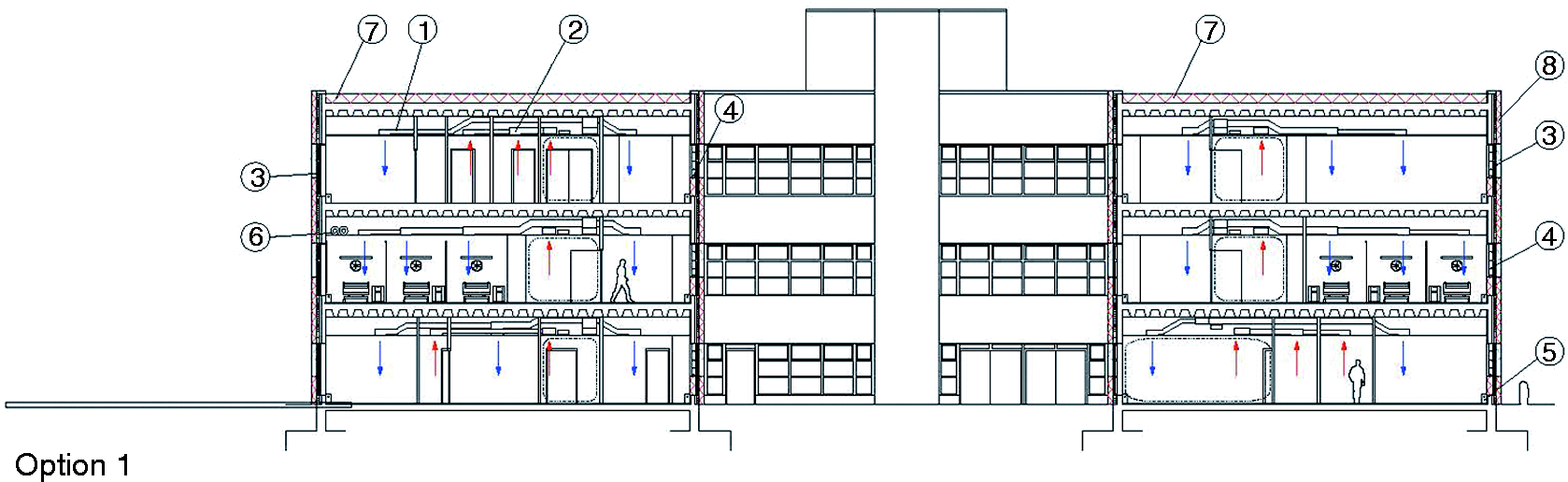
Option 2, NCVPH: natural cross-ventilation retaining perimeter heating (Figures 11 and 12), reintroduces natural ventilation as the primary ventilation strategy. This follows DH best practice guidance: HTM 09-02 para 10.15 ‘Natural ventilation of rooms should be employed wherever possible and appropriate. Design should incorporate measures for minimizing solar heat gains, which, if controlled, will avoid the need for mechanical ventilation. Measures to minimize the need for cooling should include locating temperature-sensitive accommodation away from south-facing fascias, shading windows, and using reflecting glass where appropriate and cost-effective’.
23
Para 10.16 suggests, tentatively, the potential benefit of passive nighttime cooling.
Natural cross-ventilation perimeter heating option 2 NCVH. Opening up of plan areas adjacent to courtyards to enhance cross-ventilation.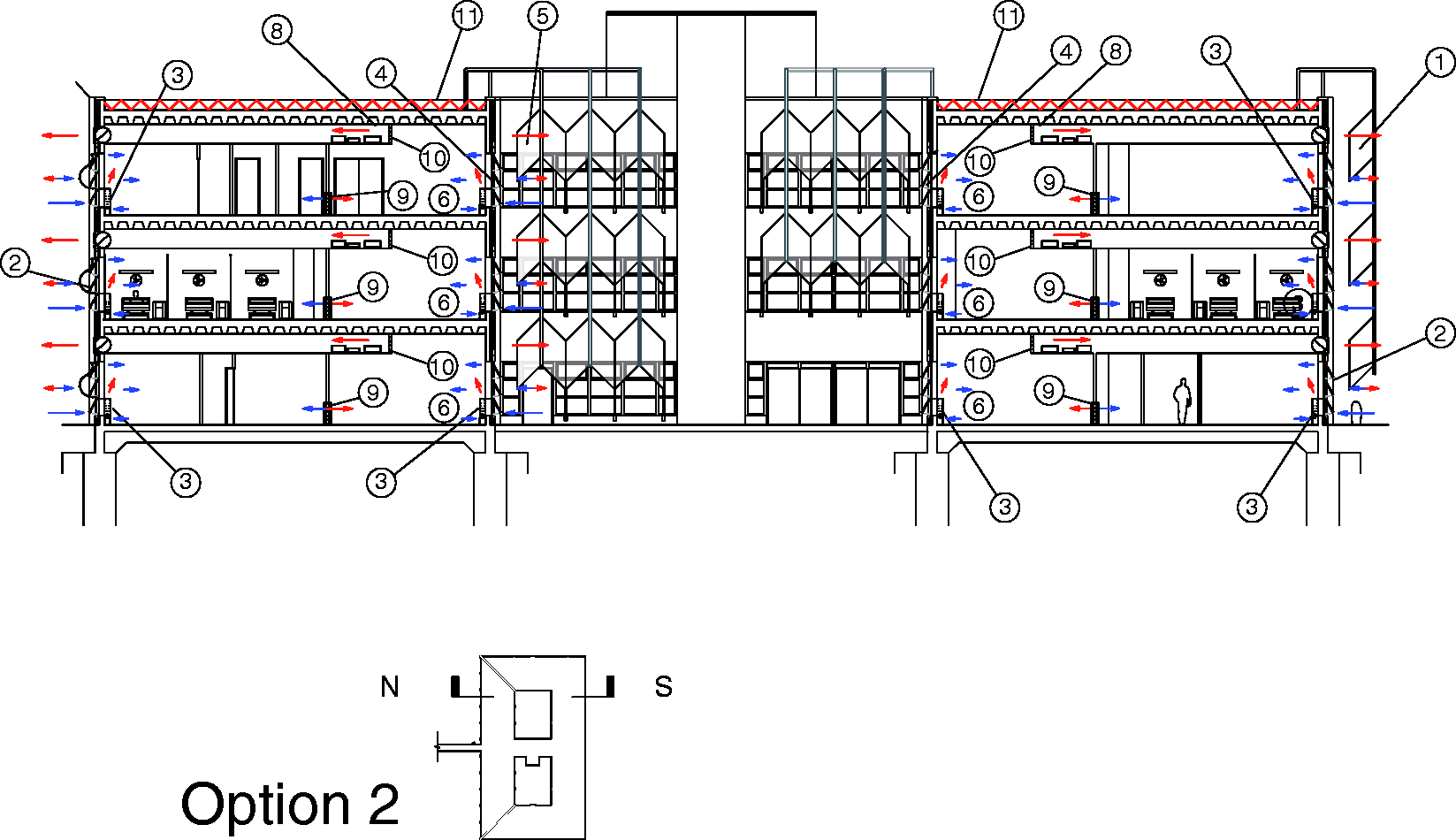
This option proposes that the roof is insulated further, all glazing to South, Southwesterly and Southeasterly elevations are shaded externally to eliminate direct summer solar gains to reduce the scale of the cooling problem, but preserving bedhead level views out from the wards, all glazed panels to open to 45° with the addition of panels below existing cill lines, all applying to glazing to the courtyard elevations within. Again this is in line with current DH guidance. HTM 07-02 para 4.61 (p. 46) promotes ‘passive solar design’, to ‘use the available daylight to its full extent’ with provisos to avoid overheating and glare. 24 It cautions that in the modern hospital setting, internal heat gains from activity and ever-increasing medical equipment may preclude passive solar design.
Spaces adjacent to the courtyards are opened out by the removal of cellular offices to become patient day-spaces and encourage distributed cross-ventilation (Figure 12). Suspended ceilings are removed in these areas to reveal concrete soffits to capture ‘coolth’ from cross-ventilation from the shaded courtyards, transfer grilles and ducts, as judged by cross-infection risk, connect these inboard spaces to the perimeter.
Option 3, ANCSVPH: Advanced Natural Cooling Summer Ventilation (see Figure 13) through glazed atria and retaining perimeter heating pursues a natural ventilation strategy and proposes the enclosure of both courtyards with glazed roofs. These become unheated atria with liberal opening areas above to dissipate summer solar gains and below slab air supply via concrete ducts offering a measure of ground cooling. All glazing to the atria becomes operable to 45°. In winter mode, air is admitted through damper-controlled perimeter heating units. Transfer ducts exhaust air from zones adjacent to the atria and again hung ceilings are cut back to expose thermal mass. External window guards deliver DH safety policy and all vulnerable glazing is shielded from direct summer solar gains. The option is capable of further refinement by incorporating winter heat recovery at the atrium head.
Option 3.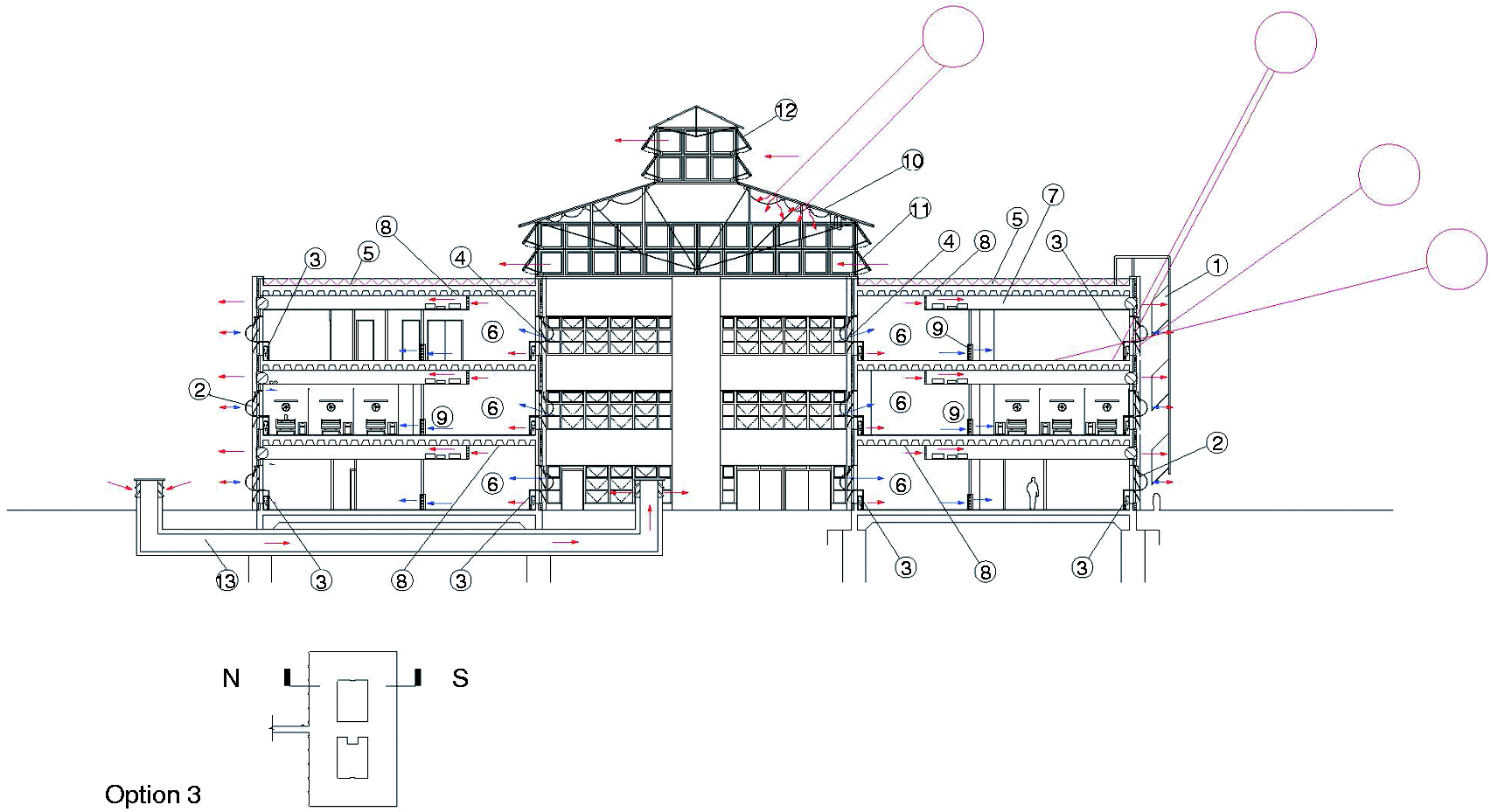
Option 4, NVPDCPH: natural ventilation incorporating passive downdraught cooling and perimeter heating (PDC) (see Figure 14) also proposes the enclosure of the courtyards but in a more active way, developing the low-energy cooling strategy of the UCL School of Slavonic and East European Studies SSEES building in Central London.
25
Cooled water batteries at high-level openings induce a downward flow of precooled air which is contained by a lightweight, acoustically absorbent, fabric shroud. The cooled air is then drawn across surrounding occupied spaces. The diagram suggests ground-sourced cooling supplements the action of the PDC by utilising thermal storage, shown as readily available water tanks, crossing the seasons so that heat gained from summer hot spells is dissipated in winter and winter coolth utilised in summer. Banks of passive solar water heaters on the roof of each PDC rooflight supplement warming of winter supply tanks. Recovered heat from all sources is gathered in winter to supplement the supply to the perimeter heating system. Air is permitted to circulate within the twin summer and winter storage chambers to a predetermined regime.
Option 4 passive downdraught cooling PDC.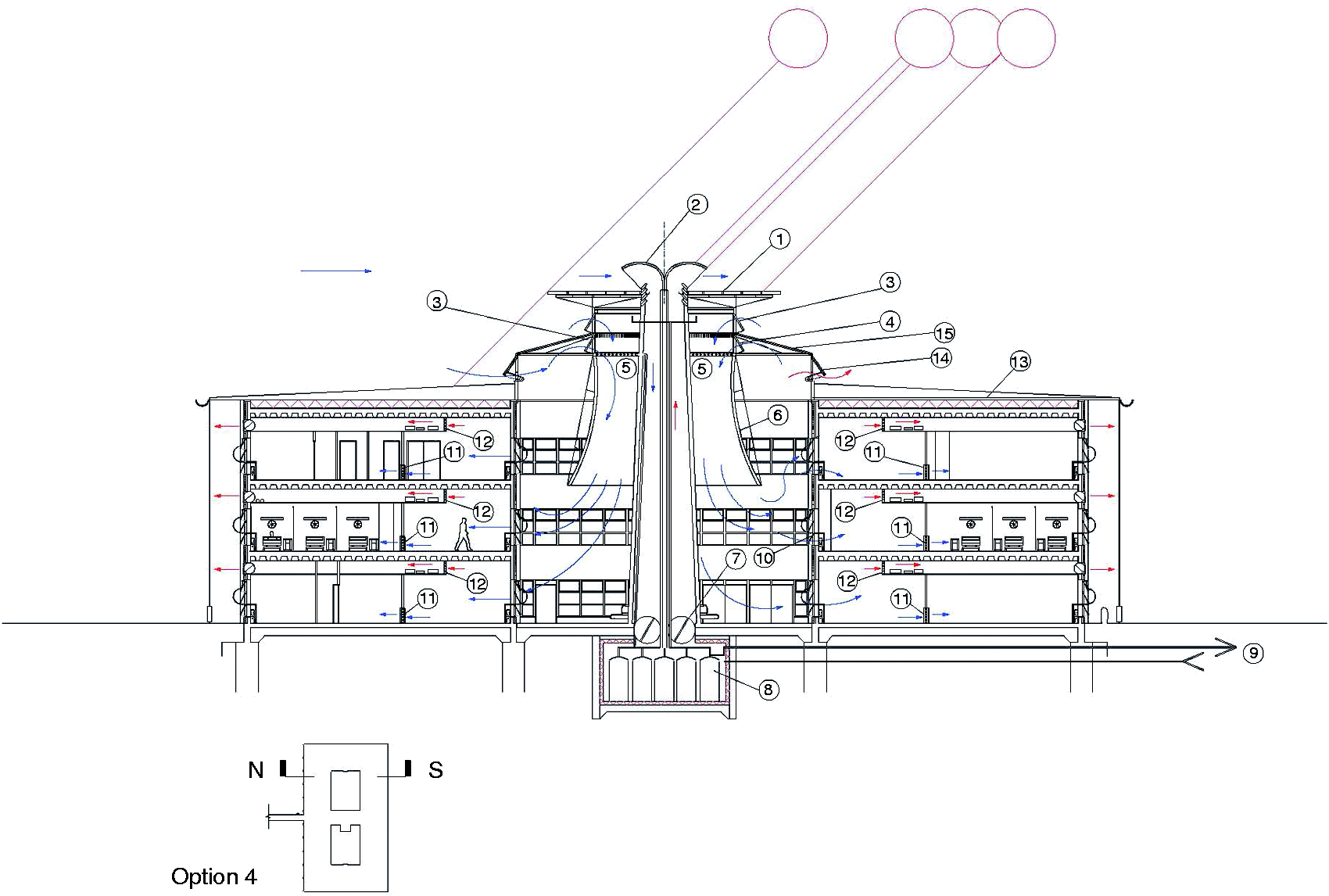
Predictions: Performance, energy consumptions and CO2 emissions
Summary of predicted performance during the summer of 2010: Three selected spaces.
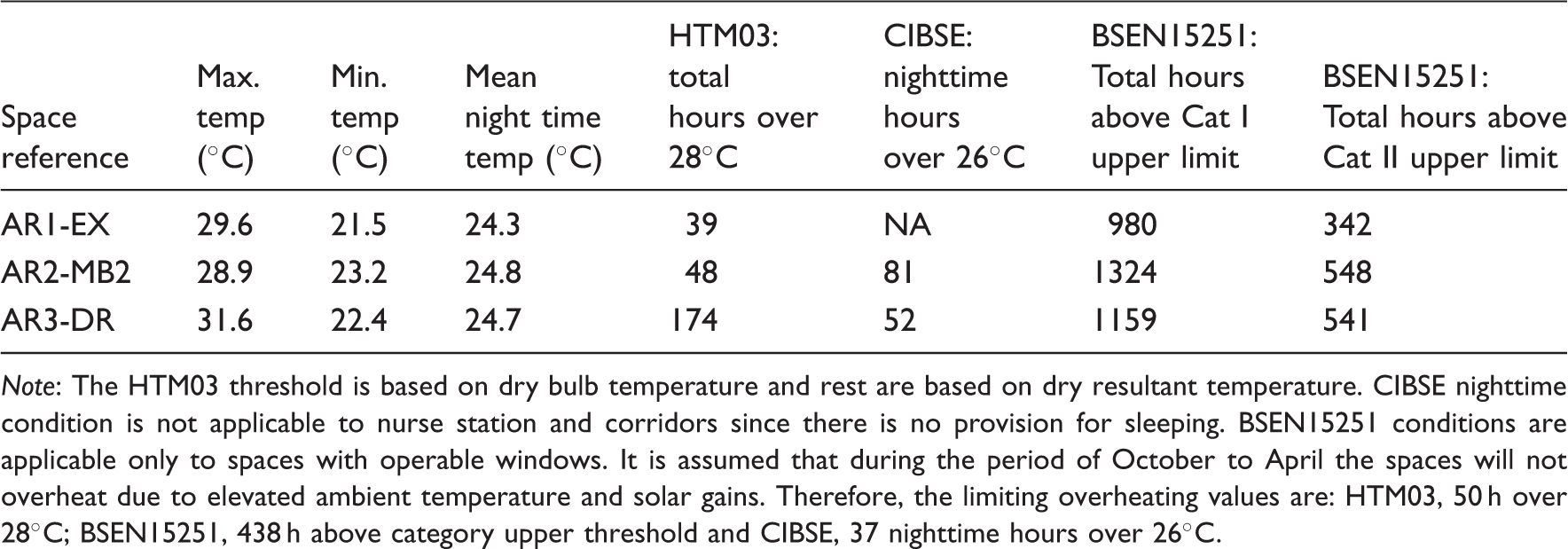
Note: The HTM03 threshold is based on dry bulb temperature and rest are based on dry resultant temperature. CIBSE nighttime condition is not applicable to nurse station and corridors since there is no provision for sleeping. BSEN15251 conditions are applicable only to spaces with operable windows. It is assumed that during the period of October to April the spaces will not overheat due to elevated ambient temperature and solar gains. Therefore, the limiting overheating values are: HTM03, 50 h over 28℃; BSEN15251, 438 h above category upper threshold and CIBSE, 37 nighttime hours over 26℃.
Summary of predicted performance for current and future, test reference (TRY) and design summer (DSY) years: Three selected spaces.

Note: SMVHC: heating and cooling through ventilation (6ach) with 60% heat recovery. NCVPH, natural cross-ventilation with perimeter heating; ANCSVPH, advanced natural ventilation through atrium with perimeter heating; NVPDCPH, natural ventilation with passive down drought cooling and perimeter heating. 05 and 30s represent 2005 (current) and 2030s, respectively. The HTM03 threshold is based on dry bulb temperature and rest are based on dry resultant temperature. CIBSE nighttime condition is not applicable to nurse station and examination room since there is no provision for sleeping in these spaces. BSEN15251 conditions are applicable only to spaces with operable windows. HTM03 standard not applicable for fans. Nighttime hours are 21:00 to 6:00. Simulated hours (3672) are for May to September. It is assumed that during the period of October to April, the spaces will not overheat due to elevated ambient temperature and solar gains. Therefore, the limiting overheating values are: HTM03, 50 h over 28℃; BSEN15251, 438 h above category upper threshold and CIBSE, 37 nighttime hours over 26℃. Unshaded values indicate that they are within the threshold limit, dark grey shade indicate that the exceedance is substantial and light grey shade indicates exceedance is minor.
In general, all three spaces under all four options met the HTM03 threshold for current as well as for future years except for AR3-DR under option-2. However, the deviation is only marginal. Further, three of the four spaces met BSEN15251 Cat I and II under all four options. Similarly, AR2-MB2 and AR3-DR met the CIBSE nighttime criterion as well.
During extreme years, DSY’s Option 1 projected the best performance in all three spaces, while the existing building exhibits the worst performance (Table 7). For the current DSY extreme conditions, all four options broadly met the HTM03 1%/28℃ while for the 2030’s Options 2–4 exceeded the HTM03 criterion. Further, during the nighttime options 2–4 room, AR2-MB2 only marginally exceeded the CIBSE criterion.
However, improved performance is achieved at a cost. Although the existing building, unaltered, has the worst thermal performance, it has the lowest energy consumption, see Figure 15, and the lowest CO2 emissions, see Figure 16.
Predicted energy demand for existing and refurbishment options for the year 2010, Cambridge (Bedford weather file). The energy values are average of AR1-EX, AR2-MB2 and AR3-DR. Predicted CO2 emissions for existing and refurbishment options for year 2010, Cambridge (Bedford weather file). The CO2 values are average of AR1-EX, AR2-MB2 and AR3-DR.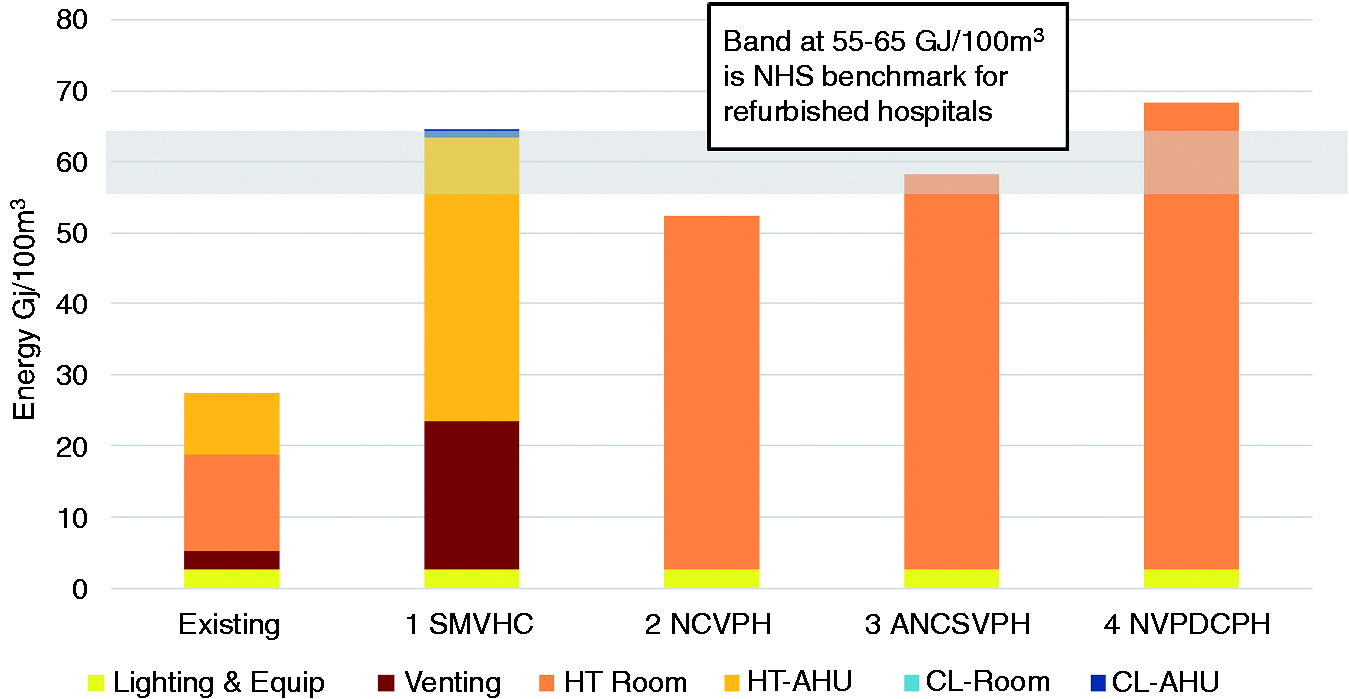
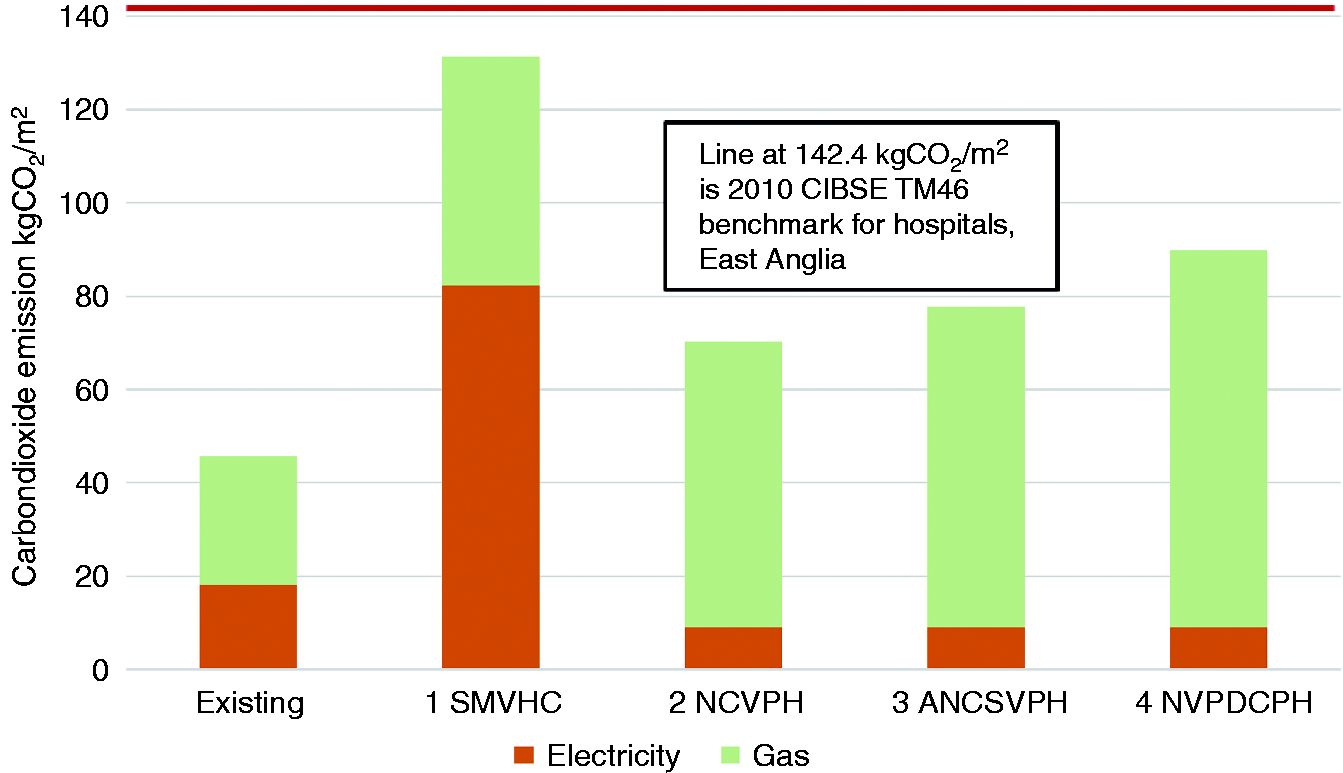
The highest energy consumption and CO2 emissions are found in options 1 and 4, respectively. Options 1–3 were within the NHS refurbishment energy bench mark, while option 4 marginally exceeded. However, all four options were within the CIBSE threshold of 28℃.
Costs of implementing the four options
Comparative cost estimates overview as of July 2012, Davis Langdon AECOM Cost Report Rev. A.
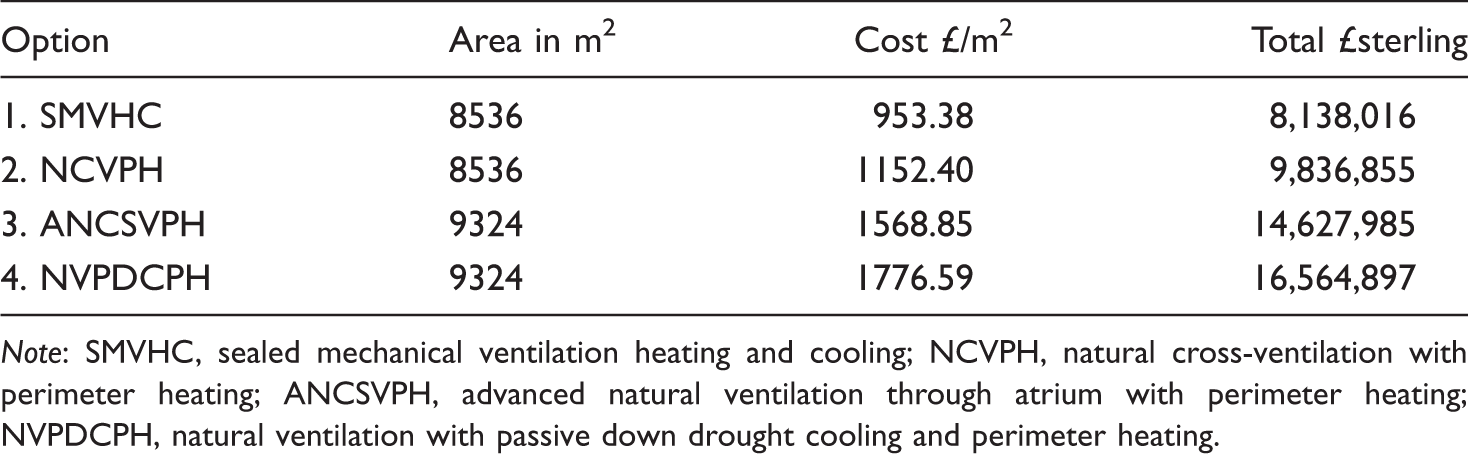
Note: SMVHC, sealed mechanical ventilation heating and cooling; NCVPH, natural cross-ventilation with perimeter heating; ANCSVPH, advanced natural ventilation through atrium with perimeter heating; NVPDCPH, natural ventilation with passive down drought cooling and perimeter heating.
Comparative elemental cost breakdown by selected elements derived from Davis Langdon AECOM Cost Report Rev. A July 2012.
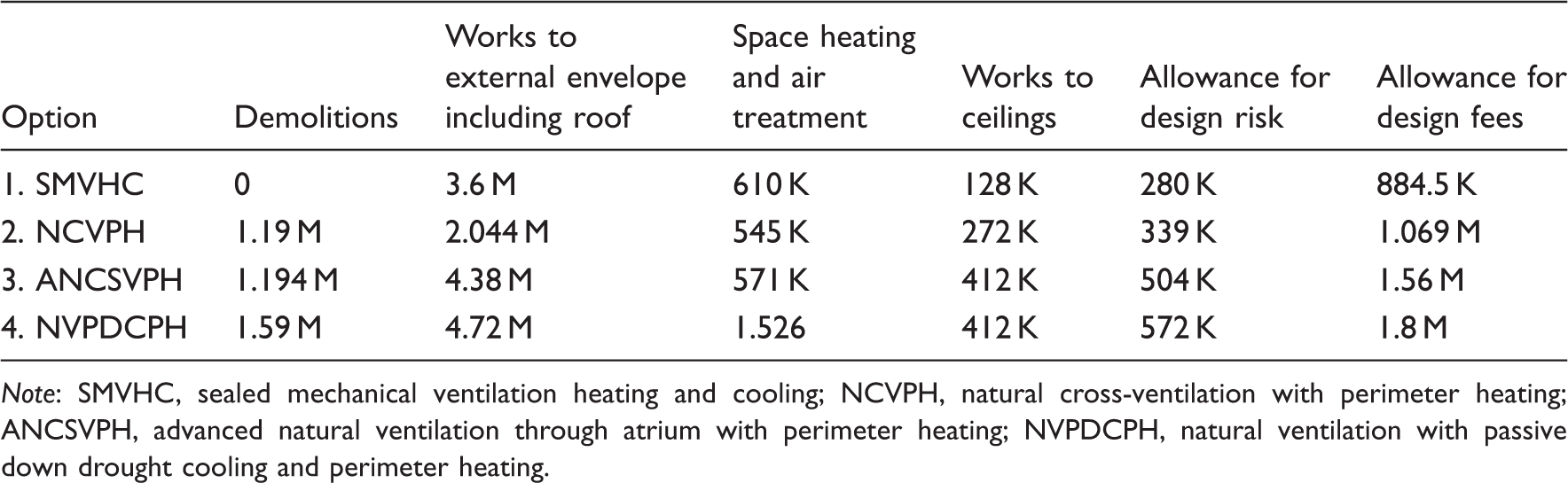
Note: SMVHC, sealed mechanical ventilation heating and cooling; NCVPH, natural cross-ventilation with perimeter heating; ANCSVPH, advanced natural ventilation through atrium with perimeter heating; NVPDCPH, natural ventilation with passive down drought cooling and perimeter heating.
Discussion and conclusions
The existing building enjoys a relatively low energy and low carbon performance against the DH guidance benchmarks but at the cost of comfort, it is unable to shed heat so that internal temperatures reach 28℃ in relatively mild external conditions. Night temperatures are consistently uncomfortable, 23.5–26℃, suggesting that simple measures against the recommended threshold may give an inadequate account, for example, one bedroom records 1992 h above 25℃, 888 of which occur at night. In the 2030 DSY, the existing building has a nighttime mean temperature in excess of 25℃. The mechanical ventilation rate is too low. In most of the bedrooms it does not even reach a minimum value of 10 litres per second per person (l/s/p).
Option 1 predicted that DSY peak temperatures oscillate around 28℃, additional cooling capacity will be required, and will be increasingly necessary. Does the building have the capacity to accommodate it? Predicted energy demand is high and associated CO2 emissions very high, 130 kgCO2/m2 almost two-third resulting from its electrical demand which will, of course, rise as cooling capacity is increased, the ‘worm in the bud’ of this approach, it has no other means of defence. Option 2 peak DSY temperatures hover between 33.5 and 34.9℃, additional cooling will be required but night ventilation cooling, an obvious response, is wholly excluded by current practice. A peak of 31℃ is predicted in TRY summer conditions. More research is required into the clinically safe night conditions in maternity wards. Could cooler temperatures be contemplated? Incubators in ICUs provide close environmental control for vulnerable infants. However, option 2 has the lowest energy penalty and markedly lower CO2 emissions than option 1. Option 3 offers similar DSY peak conditions, but TRY peaks in line with current guidance. Predicted energy demand and CO2 emissions are only marginally higher than option 2. Option 4 offers lower TRY and DSY peaks than options 2 and 3. In the natural and hybrid schemes, the unblocking of key plan areas to reduce resistance and enhance cross ventilation, especially adjacent to the courtyards, has the potential to reduce overheating substantially, but at an appreciable construction cost.
Avoiding the sealing of the building, the key characteristic of options 2–4, emerges as an important element in evolving a ‘least regret’ adaptation strategy for this building type. Option 1 emerges as requiring the lowest immediate capital investment but the additional increment for option 2 may be delivered in cash releasing and other quantifiable savings. The carbon reduction commitment payment alone will contribute significantly as will a more rapid throughput of patients. However, even the almost wholly passive adaptation option is predicted to double existing energy consumption. The current DH EEF Scheme would not fund any of the options, the Treasury requires a return on investment of 2.4 within five years of implementation. This is potentially a huge barrier to achieving adaptation of the public nondomestic building stock, which is unfortunate given that the NHS Retained Estate would seem to be a particularly promising place to implement a public sector adaptation scheme.
Footnotes
Acknowledgements
The authors would like to acknowledge the contributions of Phil Nedin and Shahila Sheikh, mechanical engineers at Arup; Paul Banks and David Nichol, quantity surveyors of Davis Langdon AECOM building cost consultants; Short and Associates Architects for producing adaptive design drawings; the ‘Expert Panel’ comprising Dr. Simos Yannas of the Architectural Association and Dr. Nick Baker of the University of Cambridge; colleagues engaged in the EPSRC DeDeRHECC project; officers of the Addenbrookes Hospital Estates and Facilities Department and the administrative and nursing staff of the Rosie hospital for their forebearance through the long process of collecting data within the building.
Funding
This work was undertaken at part of the UK Engineering and Physical Sciences Research Council project, ‘Design and Delivery of Robust Hospital Environments in a Changing Climate’ [grant number EP/G061327/1] through the ‘Adaptation and Resilience to a Changing Climate’ (ARCC) programme under the auspices of the ‘Living with Environmental Change’ (LWEC) initiative. The Project also received funding directly from the Department of Health.
Conflict of interests
None declared.