
Abstract
Previous research on the acquisition of a sign language by deaf and hard of hearing (DHH) children has indicated the importance of factors such as chronological age and age of first exposure to the language, the latter being highly variable in populations of DHH children. The results of an empirical study on the acquisition of South African Sign Language (SASL) using a sentence repetition task are presented, examining the effect of these individual factors. Participants were 40 DHH children (aged 7–9 years) attending two schools for DHH children with an official policy of using SASL, in the Western Cape, South Africa. The results clearly indicate an effect of chronological age, as well as age of acquisition of SASL, on sentence repetition accuracy. In addition, there was a significant difference in the results from the two schools. The results of the study are discussed in the light of the considerable variability in the language learning environment of DHH children in South Africa.
Keywords
Introduction
Learning a sign language as a first language is highly dependent on the quantity and quality of input offered to the child. This has been frequently shown to be the case for spoken languages as well, whether being acquired in a monolingual or bilingual situation (Hoff & Core, 2013; Thordardottir, 2011). Deaf children who learn a sign language from their deaf parents have a similar acquisition trajectory to hearing children learning a spoken language, since the quantity and quality of input is generally equivalent (Lillo-Martin & Henner, 2021; Van den Bogaerde, 2000). However, more than 90% of deaf children across the world are born to hearing families (Lederberg et al., 2013), a situation that poses barriers for full access to a sign language. Hearing parents are usually non-signers and if, once they know that their child is deaf, they decide to learn their local sign language, they are learning it as a second language and proficiency can vary hugely. Recent evidence does however suggest that, if parents have the opportunity to learn a sign language, they can attain proficiency levels that support deaf children’s language development (Lieberman et al., 2022). It is important to note that deaf children from hearing families can become highly proficient in sign languages if they also have early access to a sign language in a school environment (Finton et al., 2024).
Research on the acquisition of sign languages is pivotal for both understanding the effects of linguistic diversity on language acquisition and for developing inclusive language acquisition theories. Sign languages are underrepresented in child language studies, which overwhelmingly focus on spoken languages, particularly Indo-European spoken languages (Kidd & Garcia, 2022; Lillo-Martin & Hochgesang, 2022). This bias limits our understanding of universal and language-specific features of language acquisition. As Edward (2022) points out, indigenous African sign languages often exist within multilingual environments, adding complexity to acquisition patterns. Research on the acquisition of South African Sign Language (SASL) is, therefore, critically important for both theoretical and practical reasons. At this point in time, there are, for example, no standardised tests for SASL. The sociolinguistic context of SASL, characterised by late diagnoses of deafness, inconsistent language input, and limited exposure to proficient language models, exemplifies challenges faced by many underrepresented sign languages globally. Moreover, the current research focus on dominant sign languages like American Sign Language (ASL) and British Sign Language (BSL) leaves significant gaps in understanding the acquisition processes of sign languages with distinct linguistic and sociocultural dynamics (Edward, 2022). The recent recognition of SASL as South Africa’s 12th official language (July 2023) underscores its critical role in education and cultural preservation. Expanding research on SASL acquisition is essential not only for refining universal language acquisition theories but also for addressing the needs of South Africa’s deaf community, ensuring equitable access to education, and fostering linguistic inclusion.
This article presents the results of an empirical study of 40 deaf and hard of hearing (DHH) school children (aged 7–9 years) who are learning SASL. This study aims to evaluate specifically the impact of chronological age and age of acquisition (AoA) as individual factors in their sign language acquisition. The results will be discussed in relation to the complexity of the language learning context of deaf children in South Africa.
SASL: Background Information
The number of people who use SASL is contested. Heap and Morgans (2006) have suggested that between 500,000 and 1.5 million deaf South Africans use SASL. Census statistics have suggested lower numbers (around 235,000 in 2011, and even lower in 2022; Statistics South Africa, 2012, 2023). However, rather simplistic measurement instruments were used that may have underestimated prevalence (London et al., 2020). SASL is also used by a relatively small number of hearing people, usually children of deaf adults or professionals who work closely with members of the Deaf community.
There is little historical documentation of SASL. As is the case in many countries, the history of the sign language is closely linked to the development of deaf education. The first school for deaf children in South Africa was founded by the Irish Dominican Order in 1863. This was a signing school up to 1880 (Aarons & Akach, 1998) when an international conference held in Milan, Italy proposed that only spoken languages be used in deaf education; sign languages were then forbidden. South Africa was one of the countries that adopted these resolutions. During the period of apartheid (1947–1994), the policy of no sign language was enforced in schools with white deaf children, but not applied very strictly in schools with other races. Despite SASL being forbidden in schools, it was still used by deaf people outside the educational context (Aarons & Akach, 1998).
Since 1996, the official policy has been that “[a] recognised Sign Language has the status of an official language for purposes of learning at a public school” (The South African Schools Act, 1996). The Constitution of the Republic of South Africa (1996) also proclaimed “Sign Language” to be one of the languages of South Africa that must be promoted and that adequate conditions for its ongoing development and use must be created. In 2009, SASL was included as a Home Language subject in the national curriculum. A committee created by the Minister of Basic Education was tasked with the creation of a full curriculum (Holness, 2016; Morgan et al., 2016, p. 17). This full curriculum was first introduced in 2014 (Morgan et al., 2016, pp. 17, 20) making it possible for SASL to be taught up to matric (grade 12) in schools for DHH children. Since then, materials for use in the curriculum have been developed by diverse bodies, meaning that there is no set of uniform materials used by all schools. In July 2023, SASL was recognised as the 12th official language through a constitutional amendment. As a consequence, the Pan South African Language Board now has a specific section for SASL that is charged with developing resources for this language.
Despite these official changes in policy, SASL is still not always used as a language of teaching and learning in schools for the deaf. Of the 43 schools for DHH children across the country, only 35 use SASL in some form. Teachers in these schools are predominantly hearing and only a very low percentage have adequate SASL proficiency (Du Plessis, 2025; Ngobeni et al., 2020). Furthermore, some schools still have, in practice, policies of total communication (i.e. using a sign supported version of a spoken language) or oralism (where all focus is on using a spoken language).
Learning a Sign Language as a First Language
Research on children’s acquisition of sign languages has been conducted in several countries (see reviews by Chen Pichler, 2012; Lillo-Martin & Henner, 2021). The research on DHH children born into signing deaf families indicates that very similar milestones are achieved at similar times to hearing children learning a spoken language. For example, first words and first signs occur generally between 1;0 and 1;5, while multi-word combinations appear for both groups between 3;0 and 3;5 (Baker et al., 2016). Where this is not the case, that is to say a DHH child is born into a hearing family that does not offer a sign language to the child, the path of acquisition will be delayed.
There are no published studies focussing on the acquisition of SASL. One recent study examined general early development in deaf children (Young et al., 2025), reporting on the adaptation and pilot testing of the Early Learning Outcome Measure (ELOM 4&5) administered using SASL. The ELOM (4&5) is specifically designed to measure the progress of 4- and 5-year-old children across five domains of early childhood development, one domain being Emergent Literacy and Language (ELL). No details of the instrument for measuring ELL are given. The pilot results indicated that over all 5 domains only 2 out of the 29 (6.9%) children were at or above the 60th percentile ELOM (4&5) standard distribution. In one case, both parents were Deaf and SASL was a home language. For the ELL specifically, 26 children (89.6%) were assessed as “falling far behind.” The authors query whether the very poor performance of the sample of deaf children is a true reflection of the children’s ability or whether the ELOM (4&5) was scoring the children below their true ability. They also question whether the quality of the children’s sign language is sufficient to be able to understand and navigate the assessment process in general. This article emphasises the difficulty of assessing young deaf children’s linguistic ability in the South African context.
In many of the studies of deaf children acquiring a sign language, the children have been older than those in Young et al.’s (2025) study. In these studies, various factors have been shown to influence acquisition of a sign language. Below, we will consider some of these factors in general and, where possible, in the context of South Africa.
Age of Diagnosis of Deafness
For the small number of DHH children born into deaf families, deafness is often spotted earlier and a diagnosis obtained. DHH children born into hearing families are dependent on an indication of deafness being picked up by neonatal screening, health checks, etc. The prevalence of hearing loss in children world-wide is large. It affects approximately 15.5 million children under the age of 5 years, but there is considerable variation in prevalence between areas of the world. In sub-Saharan Africa, for children aged between 5 and 14 years, prevalence is estimated in a WHO 2013 report at 1.9% as opposed to 0.4% in high-income countries (cited in Kuschke et al., 2020).
Neonatal screening is the most efficient way of detecting deafness. In a 2019 survey of 46 European Union countries, only four had no neo-natal screening in place, but the organisation of the neonatal screening in the other countries varied considerably (Mackey & Uhlén, 2019). Furthermore, most of these EU countries have some form of pre-school hearing screening (3–6 years) and screening at school entry. In contrast, there is no universal neonatal screening protocol at the current time in South Africa; this is only sometimes provided in private medical care (Kanji & Khoza-Shangase, 2021). Pre-school hearing screening is also not systematic (Eksteen et al., 2022).
A 2019 study of 240 children under the age of 6 years with confirmed hearing loss was conducted in the Western Cape province of South Africa, a province with good medical and educational facilities in comparison to some of the other provinces in South Africa (Kuschke et al., 2020). The results of the study indicated that the mean age of diagnosis of permanent congenital or early-onset hearing loss was 31.4 months (22.8 Standard deviation [SD]; range 2–72), with a mean delay of 9 months (13.2 SD; range 0–60) between age of suspicion and diagnosis of hearing loss (n = 93). These figures indicate that some children in the study were diagnosed at birth but some as late as 6 years of age, the oldest children in the study. The possibility that children may be diagnosed later than 6 years of age exists and the mean ages of diagnosis may be higher in other provinces.
AoA of a Sign Language
The diagnosis of deafness is crucial in families with hearing parents for the decision to be taken to offer the child a sign language. Following diagnosis, the information offered to parents in counselling services is critical to indicate that the choice for a sign language is possible. The opportunity to learn the local sign language also needs to be available. Across the world, it is common that the first contact with any sign language input is at a school for DHH children. Before school entry, the child does, therefore, not have access to full language input and communication with the child in the family is minimal at best. In Europe, there is considerable availability of counselling services, although a 2016 study indicated that these could be greatly improved (Allen et al., 2016). In South Africa, information is not always accessible for families living in rural areas and the services that exist take different formats. Davids et al. (2023) make strong recommendations for services in the South African context. They emphasise the need for counselling for parents, the facilitation of parent-to-parent support groups and specific programmes for engaging fathers, connecting parents with deaf mentors and connecting them to, or developing, programmes within the domain of parenting and parenting styles. Most schools for DHH children in South Africa admit children as young as 3 years of age. Some children are diagnosed extremely late and, even when diagnosed, they are not necessarily sent immediately to a school for DHH children.
In previous research, AoA has been shown to contribute to sign language proficiency in both deaf adults and children (Lillo-Martin et al., 2020). Studies have highlighted that the younger the child learns a sign language, the greater their later proficiency (Lillo-Martin & Henner, 2021). Furthermore, late AoA can affect the acquisition of specific linguistic structures (Krebs et al., 2021), and brain function and linguistic abilities (Malaia & Wilbur, 2010), meaning that full adult competence may not be achieved (Mayberry, 2010).
Schönström and Hauser (2022) tested both deaf adults and children with a Swedish Sign Language Sentence Repetition Task (STS-SRT). The AoA in the adult group ranged from 0 to 7 years old, mean 1.33, while in the child group AoA ranged from 0 to 9 years old, mean 1.79. They found that, despite Sweden having a relatively low occurrence of late diagnosis and thus early exposure to STS, AoA nevertheless accounted for 14.4% of the variance in the correct repetitions of their participants, with delayed sign language acquisition (implicitly defined by the authors as after the age of 3) associated with lower scores. This confirms observations by Mayberry and Kluender (2018, p. 892).
Quality of Sign Input
Many children arrive at a DHH school with no previous exposure to any signed form of language (see, Batchelor, 2010, p. 499, for a description of the South African situation). In many countries, prior to schooling, communication in hearing families with a DHH child is based on the use of gestures combined with words from the local spoken language. This is usually referred to as home signing (Hill et al., 2018). Home signing systems are also usually specific to a particular family in terms of the gestures and structures used. 1 At school, the child will then be exposed to full sign language input, probably for the first time.
Even once at school, the input of a sign language can be problematic. Most teachers of DHH children are hearing and rarely native signers. In most countries, it is not a legal requirement that teachers of DHH children have any sign language proficiency, although this is expressed as a preferable option. Some countries, such as the Netherlands, have specific training for teachers of deaf children, including proficiency in Sign Language of the Netherlands. In South Africa, teachers of DHH children have to obtain their general teaching qualification, but there is no stipulation that the student teachers must learn SASL. There is also a lack of in-service training (Ngobeni et al., 2020).
In the past, teachers of deaf children have been encouraged to offer Total Communication. This approach uses all available means of communication, including spoken language, sign language, written language, gestures, and other visual supports. It is flexible in that individual needs and preferences of each learner can be accommodated. This approach has been shown to be effective with children with complex language and communication needs (Luckins et al., 2025). However, Scott and Henner (2020) have argued strongly against anything but the use of a full sign language in deaf education, since mixtures of communication forms result in a confusion of models with little consistency.
Currently, in South Africa, hearing teachers frequently offer a mixture of a spoken language and a sign language, sometimes called a sign system. A sign system takes the grammar from a spoken language and the lexicon from a sign language (Morgan et al., 2016, p. 21). Such sign systems are intended to teach the students the structure of the spoken language, but there are no clear guidelines on how this should be done. Common practice is that SASL as a subject is taught by competent signers but that other subjects are taught using a sign system. In South Africa, such a sign system might be sign-supported English (SSE), sign-supported Afrikaans, or sign-supported Zulu. Example sentences illustrate a well-formed sentence in SASL (1) and its version in SSE (2).
(1) tomorrow rain index1 swim index1 South African Sign Language
“If it rains tomorrow, I am not going to swim” Conditional clause + negative
(2) if rain tomorrow, index1 not will swim Sign-supported English
“If it rains tomorrow, I am not going to swim” 2
Despite materials for teaching SASL having been continually in development since 1996, 3 many schools lack resources (Ngobeni et al., 2020). Some schools for DHH children also adopt materials from other sign languages, meaning that language structures and lexicons become mixed.
To summarise, we have indicated the relevance of the factors age of diagnosis of deafness, AoA, and quality of input. As discussed, DHH children in South Africa can be in highly diverse situations with respect to learning SASL. In the empirical study reported on in this article, we explore the influence of the individual factors of age and AoA on the acquisition of SASL as evident through learners’ accuracy on an SRT.
A Study Using the SASL-SRT
The aim of this empirical study was to investigate the impact of two factors, age and AoA, on the first language acquisition of DHH children learning SASL. An SRT was chosen as the appropriate instrument to evaluate children’s acquisition level. In an SRT, pre-recorded sentences of different lengths and with different structures are presented; the children are then asked to produce an exact repetition of these sentences. The children need to be able to process the sentences, make linguistic representations, extract meaning, and have the memory capacity to reproduce what has been presented (Marinis and Armon-Lotem, 2016, p. 6). 4 Marinis and Armon-Lotem (2015, p. 5) have shown that such SRTs are useful in testing language proficiency in children acquiring a spoken language. Hauser et al. (2008) and Marshall et al. (2015), among others, have shown the same for sign language. Hauser et al. (2008) found that the ASL-SRT distinguished between hearing and deaf users of ASL, as well as native and non-native users. It was judged suitable for use with children. Marshall et al. (2015) found that the BSL-SRT differentiated between Specific Language Impairment and language-input delay.
Mayberry and Fischer (1989) were the first to show a significant effect of AoA using a shadowing task (essentially an SRT), examining the performance of young DHH adults with AoAs from birth to 18 years old. Bogliotti et al., (2020) found significant effects of both chronological age and AoA in a group of 62 children (6;9–12;8 years), acquiring French Sign Language. Schönström and Hauser (2022), in turn, tested 30 adults and 14 children using the STS-SRT, based on the ASL-SRT, and also found significant effects of AoA in both their adult and child groups. Their analysis, using a linear mixed model, indicated that adults scored 20.2% higher than children. The children had a range of scores from 1 to 14 out of a maximum of 31 (3%–45%), with a mean of 5.86 (19%).
To date, no studies have been published on the acquisition of SASL in deaf children examining the impact of the factors discussed above. To start filling this gap, the present study was guided by the following research questions:
What is the performance of deaf primary school children (7–9 years) on the SASL-SRT?
Do the SASL-SRT scores of deaf primary school children change with chronological age, and if so, how?
Is there an effect of AoA, and if so, what is the nature of this effect?
We hypothesised that there would be a gradual improvement in scores based on chronological age and that AoA would have a strong effect, with an earlier AoA correlating with a higher score.
Method
Participants
Two schools for DHH children were approached in the Western Cape to participate in this study. On the basis of available information, the schools were judged to be similar. They both have a policy of using SASL as a language of teaching and learning and have comparable SASL resources. They both employ deaf teaching assistants. 5 From the children in the age range 7;0 to 9;11, 40 children were selected: 21 from School 1 and 19 from School 2. Selection criteria were that the child should have had at least 1 year of full exposure to SASL, that there should be no impairments additional to deafness, that written consent from parents/legal guardian should have been provided, and that the child assented to participate. The selection was based on a background questionnaire which parents, legal guardians, and/or teachers were asked to complete in writing.
The spread across the age groups was fairly even. There were slightly more boys than girls as is common in this population. A background questionnaire, developed by the authors for use in various SASL-related projects, elicited information, amongst other things, on the age of the child, the age of diagnosis of deafness and the age of first exposure to SASL, (i.e. AoA) (see Supplemental Appendix 2 for the full background questionnaire). Selected information about the participants is presented in Table 1.
The Mean Age, Range of Age of Diagnosis, and Range of AoA of Participants in the Three Age Groups.
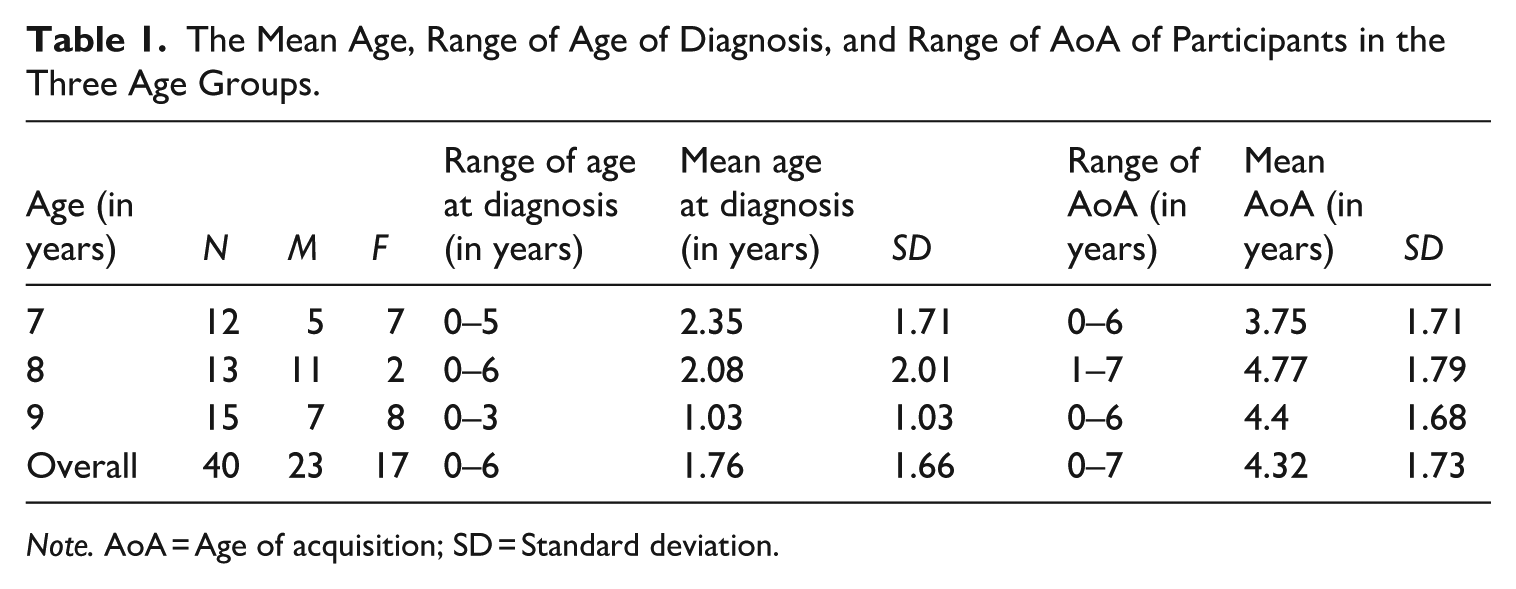
Note. AoA = Age of acquisition; SD = Standard deviation.
According to the questionnaire data, two children had been exposed to SASL from birth, having been born into deaf signing families (AoA = 0). Eight other children were also diagnosed at birth but were not exposed to SASL until they started attending school, which resulted in a considerable delay in any SASL input. The AoA for these children ranged from 2 to 6 years old. It is important to note that 28 out of the 40 children started acquiring SASL after the age of three, which is generally considered delayed acquisition.
From Table 1, it is relevant to note that the age of diagnosis varies considerably, but the mean of 1.76 years (21.12 months) is somewhat lower than the 31.4 months found by Kuschke et al. (2020), who conducted their study in the same province. As described earlier, screening procedures for deafness such as post-natal testing are not systematic in South Africa.
From the background questionnaire, it emerged that there was a range of spoken languages used as the home language, most commonly Afrikaans, English, and isiXhosa. It was also clear that many families used more than one spoken language at home.
Materials
The SASL-SRT, developed by the authors for use with adults and children, was employed in this study. The sentences were created by two deaf native SASL signers, one of whom is a linguist, in consultation with the authors, and were not translations of sentences from other SRTs. These sentences were constructed to include simple declarative sentences (e.g. one predicate with two arguments, negation), simple questions, and more complex sentences with complex nominals, and different types of subordinate clauses. Some of the grammatical constructions used necessarily involve non-manual markers (NMMs), namely raised or lowered eyebrows for questions or wh-clefts, headshake for negation, and raised eyebrows marking imperatives and conditional clauses. There is not enough research on SASL to determine a valid complexity measure for these different structures. The sentences also varied in length in terms of manual signs; NMMs were not included in this calculation (see Supplemental Appendix 1 for the full list of SASL-SRT sentences). The SASL-SRT contained 20 test sentences and three practice sentences (see the illustrated examples in Figure 1).
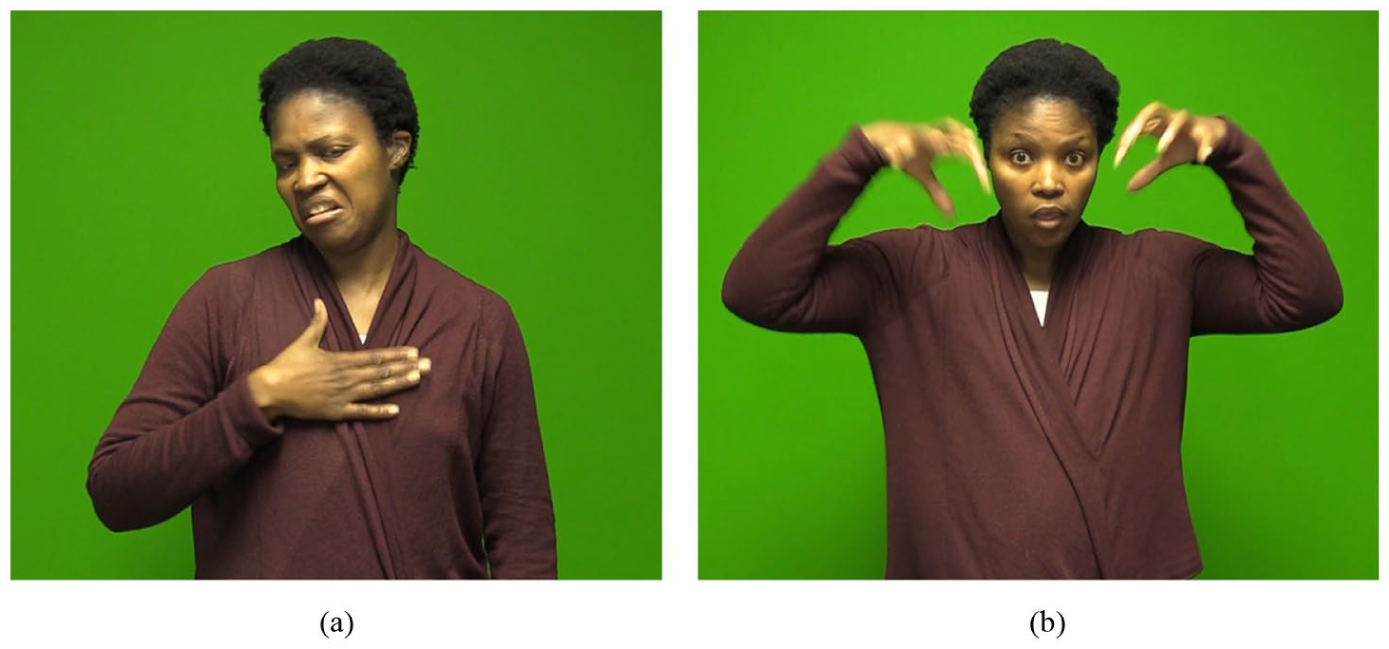
Two example stimulus sentences from the SASL-SRT.a (a) “S/he does not like milk” see glossed version in sentence (3) (b) “If it rains tomorrow, I am not going to swim.” see glossed version in sentence (2)
The sign vocabulary used and the grammatical constructions were subsequently tested with two native DHH signers from the local deaf community and discussed with the teaching staff of the two schools. There is considerable lexical variation in SASL between schools for the deaf (Huddlestone et al., 2025), and it was important to choose lexical items which the children would be familiar with.
After the children had been tested, a pilot with adults (N = 35; 18–47 years) was conducted. Six sentences were adapted between the child and adult administrations (S6, S7, S15, S16, S17, and S18). Reliability for the full adapted 20-item adult form was high (α = .86) with most items showing acceptable to strong corrected item–total correlations (median r_it ≈ 0.52). Only one item (S16) showed zero variance and was excluded from psychometric modelling (see section “Analysis”). The adult participants obtained a mean total score, including NMMs, of 7.23 out of 20 (SD = 4.49; Median = 8; Interquartile range = 5; range 0–16), 95% confidence interval (CI) [5.69, 8.77], with floor and ceiling effects of 8.6% at 0 and 0% at 20, indicating a difficult test. For a like-for-like comparison with the children in this study, we later restricted both datasets to the 14 unchanged items (S1–S5, S8–S14, and S19–S20).
Procedure
An introduction video, an instructional video, and the 3 practice sentences and 20 test sentences were recorded using 2 native signers of SASL. The introduction video gave a simple explanation of the purpose of the recording (referred to as an activity) and presented a signed version of the consent form. The instructional video explained the structure of the activity with first the practice sentences (when the children could ask questions) and then the test phase (when an exact repetition of the sentence was required).
A different deaf assistant, an L1 signer of SASL, conducted the procedure in each of the two schools using SASL. They received training in how to conduct the test and signed confidentiality agreements. They confirmed whether the child understood the procedure. The children seemed at ease and asked questions in the initial phase.
The setting for the data collection was a classroom in the school. There was a laptop and monitor on the desk, and a video camera to the side for recording the responses. The child was placed so that they could only see the monitor. A hearing researcher controlled the presentation of the videos but did not communicate with the child during the test.
Each child was welcomed by the deaf assistant and introduced to the researcher. They then watched the introduction video and had the chance to ask questions of the deaf assistant. The deaf assistant made sure that the children understood that they could refuse to take part and could end their participation at any time, with no negative consequences. The child then signed the physical assent form. The deaf assistant repeated the questions asked on the assent form and assisted those who could not yet read by showing them where the “yes” and “no” options were for them to make their choice.
The instructional video was then shown and the deaf assistant checked whether the child understood what they would be doing. The practice sentences were then shown. The video clip of the sentence was played to the child using the system default video player, and then, they were asked to repeat the sentence as accurately as possible. Each child’s repetition was recorded with the video camera. In the case of there being any confusion with the task instructions, the deaf assistant clarified. After the practice sentences had been completed, the child could then discuss and query any parts of the procedure about which they were feeling unsure.
This procedure was then followed for the elicitation of the 20 sentences in the main test except that no questions were encouraged or answered. The sentences were presented in a different random order for each child, as is standard practice in psycholinguistic experiments to avoid fatigue effects in the longer sentences. The children were finally thanked for their time and offered a small treat. The testing took an average of 30 min to complete per child.
Analysis
In the primary scoring phase, a score of 1 was awarded for a correct repetition (an exact match to the model sentence); a score of 0 for an incorrect repetition (a mismatch). Responses were coded as incorrect both when no attempt was made to produce a repetition (i.e. skipped) and when the response contained extra material not present in the model sentence (i.e. unanalysable). A skipped response was typically indicated by the child not producing any signs, signing
Sign order and lexical substitutions were also considered. The order of the signs in the sentence had to be as in the model. The lexical signs had to have at least three of the four manual parameters correct (handshape, orientation, location, and movement). In accordance with practice in sign language research, a difference of one parameter between two signs means that both forms are regarded as phonological variants of each other, unless the two forms have a different lexical meaning (McKee & Kennedy, 2000). For example, if the sign for
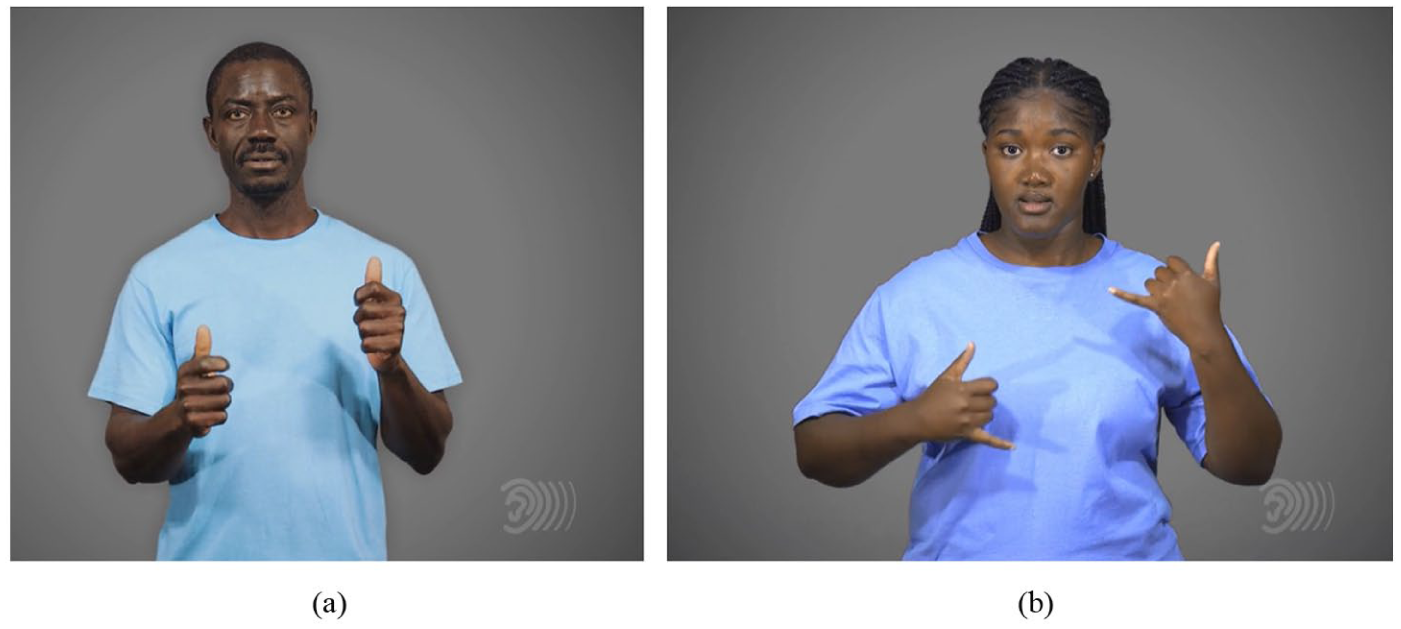
Two variants of MILK (source: NID SASL dictionary https://www.learnsasl.com/). (a) Variant MILK-1. (b) Variant MILK-7.
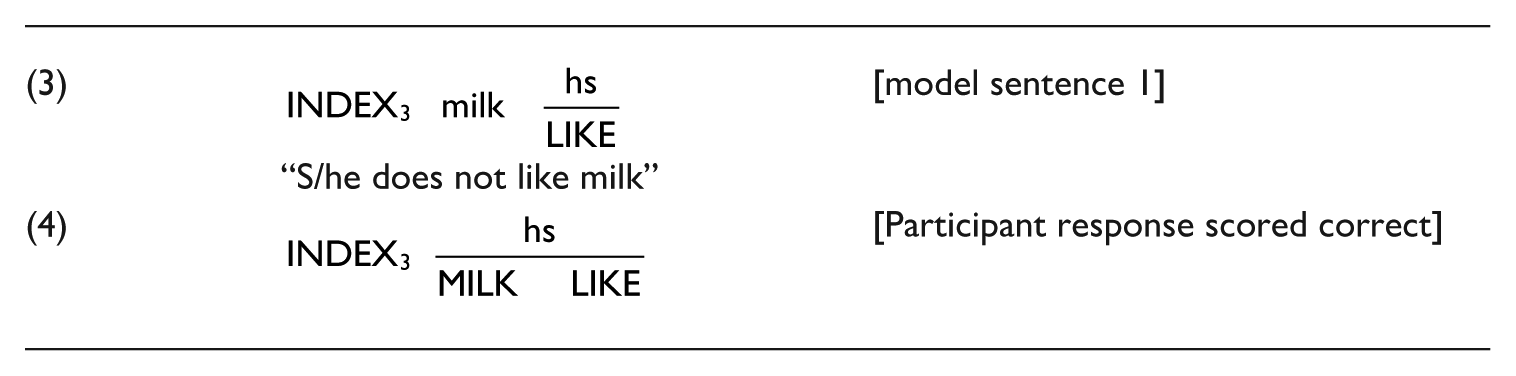
Only the NMMs required for grammatical marking contributed to achieving an exact match repetition. These were, for example, a headshake in negative sentences, the eyebrow movement in questions, and the eyebrow raise marking imperatives and conditional sentences (see Supplemental Appendix 1 for the full list of sentences including NMMs). Other pragmatic NMMs, such as an emphatic head nod, were disregarded. The scope of the NMM was not considered. Thus, for example, the model sentence in (3) indicates a headshake synchronised with the manual sign
After the data had been scored, data processing and statistical analysis were performed with R Statistical Software (v4.4.2; R Core Team, 2024). Internal consistency of the SASL-SRT was assessed using Cronbach’s alpha and Guttman’s Lambda-6 via the psych package (Revelle, 2025), along with item-total and inter-item correlations. Dimensionality was explored using parallel analysis; however, further factor-analytic approaches (e.g. Kaiser–Meyer–Olkin and Bartlett’s tests) were limited by restricted item variance.
A mixed effects logistic regression model with mean-centred predictors and sum-coded factors was used to model item-level accuracy (binary: correct/incorrect), with participant characteristics (age, AoA, school, and gender) and item characteristics (sentence length and NMM presence) as fixed effects, and incorporating random intercepts for participants and items. This approach accounted for the repeated-measures structure of the data while estimating fixed effects of participant- and item-level predictors. We report both model coefficients (sum-coded deviations from the grand mean) and pairwise contrasts (e.g. School 2 vs. School 1) to facilitate interpretation and ensure results are invariant to coding choices. The model was fitted with the lme4 package (Bates et al., 2015), using a binomial distribution with a logit link. Odds ratios (OR) and 95% CIs were calculated by exponentiating log-odds coefficients, using broom.mixed (Bolker & Robinson, 2025) and dplyr (Wickham et al., 2019). Multicollinearity was assessed using variance inflation factors (VIFs) from the car package (Fox & Weisberg, 2019).
Results
Overall Results
The full sample of 40 children produced 800 responses in total. Unfortunately, the recording of two responses to one test sentence was corrupt and could not be used. The total dataset, therefore, consists of 798 responses. Table 2 shows the total correct responses for the three age groups.
Overall Correct Responses for the Three Age Groups.
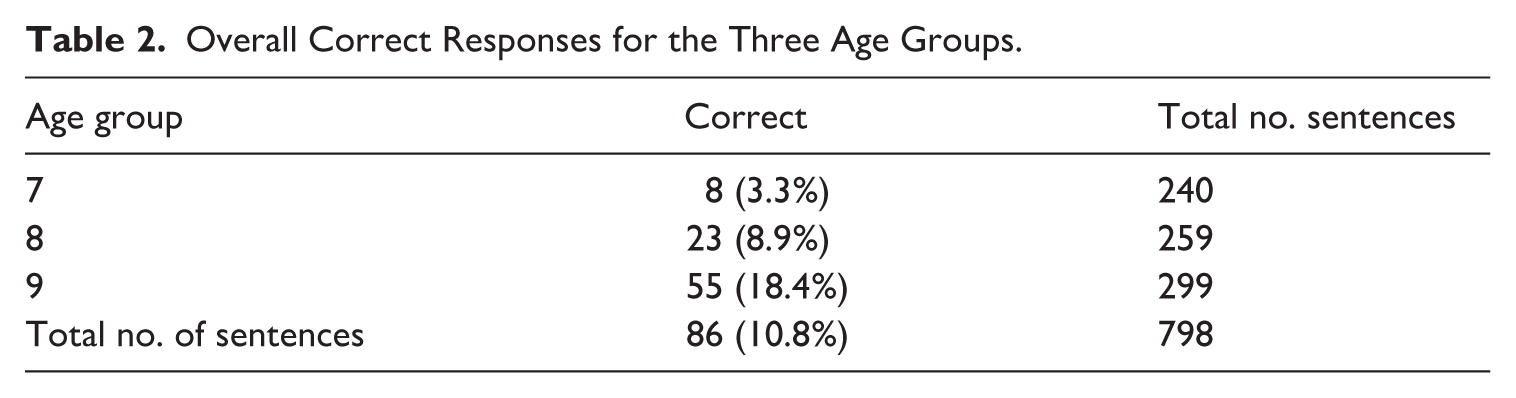
Of the 40 participants, 28 produced one or more correct responses. The distribution of total scores ranged from 0 to 10, out of a maximum of 20, with a mean of 2.2 (SD = 2.45) and a median of 1.5. Most children scored between 0 and 3, as indicated by the lower quartiles (Q1 = 0, Q3 = 3), suggesting that performance was generally low. See Figure 3 for a histogram of the total scores distribution. The distribution was positively skewed, with a small number of participants achieving relatively high scores, while the majority demonstrated limited repetition accuracy. These results indicate considerable variation in performance and suggest that the task posed a challenge for many of the participants.
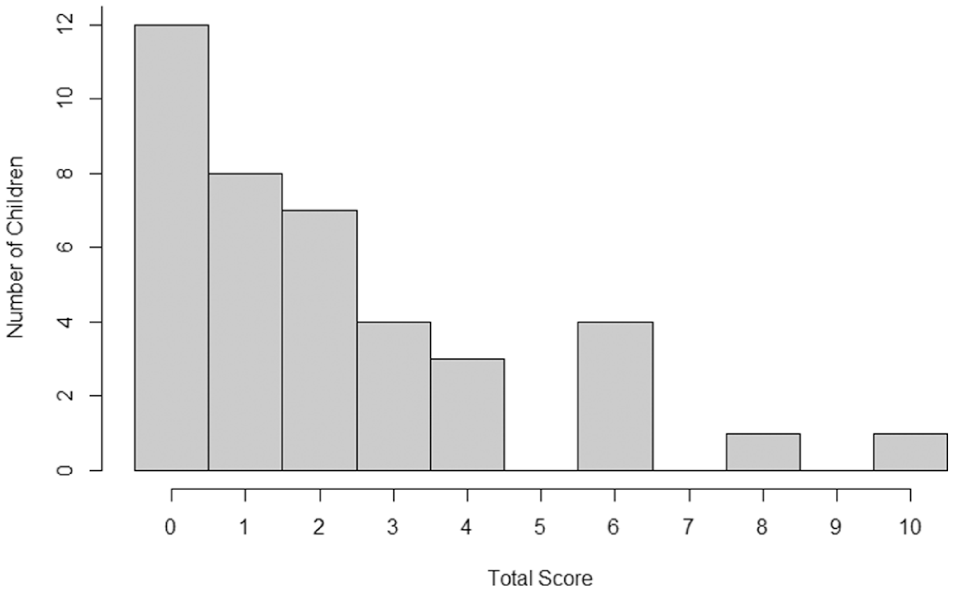
Histogram of distribution of total scores.
Skipped and Unanalysable Responses
Skipped and unanalysable responses were examined separately from other incorrect responses. There were 18 (2.3%) skipped responses and 50 (6.3%) unanalysable responses. With respect to skipped responses, there was one child (7 years old) from School 1, who was an outlier, having 12 skipped responses to the 20 items presented (>50%). This child had appeared to understand the task in the practice items; however, the responses produced for the other eight test sentences were incorrect. Skipped responses are not necessarily related to the child’s grammatical abilities, as they are not an attempt to repeat the model sentence exactly. The majority of responses in this category was due to this one child, whose results were, therefore, removed from the model analyses.
With respect to unanalysable responses, 10 children of the 40 children produced such responses, but only 4 produced more than 5 unanalysable sentences (⩾30%). Again, these children’s results were removed from the model analyses. The data from these four children, all from School 1, together with the child who produced the majority of skipped responses, are presented in Table 3. It is interesting that most of these children had learned SASL relatively early, that is, had relatively low AoAs.
Children Producing More Than Five Skipped or Unanalysable Responses.
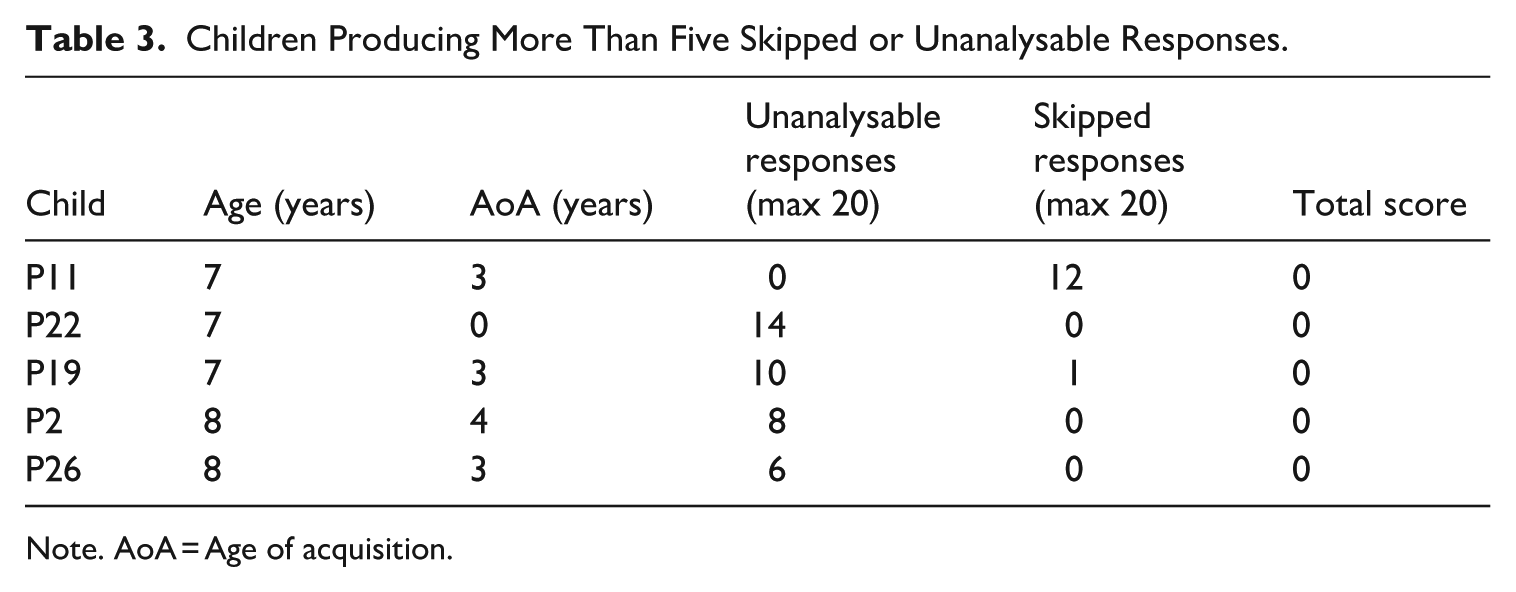
Note. AoA = Age of acquisition.
As discussed, these types of responses do not necessarily reflect the child’s grammatical competence or their ability to perform the SRT, but rather a lack of analysable data. Including these participants would have introduced noise and potentially biased the results of the statistical models, which rely on interpretable, scorable responses to identify meaningful patterns in performance.
Reliability and Validity of the SASL-SRT for the Child Group
To evaluate the psychometric properties of the SASL-SRT for this study, internal consistency was evaluated using Cronbach’s alpha, which yielded a value of α = .80, indicating acceptable reliability for group-level comparisons. The Guttman’s λ6 (G6) value of .91 and an average inter-item correlation of .23 further supported the internal coherence of the test. A filtered analysis excluding the five children discussed above produced α = .78, G6 = .87, and an average inter-item correlation of .21. See Table 4 for the reliability and dimensionality results.
Reliability and Dimensionality Results for the SASL-SRT.
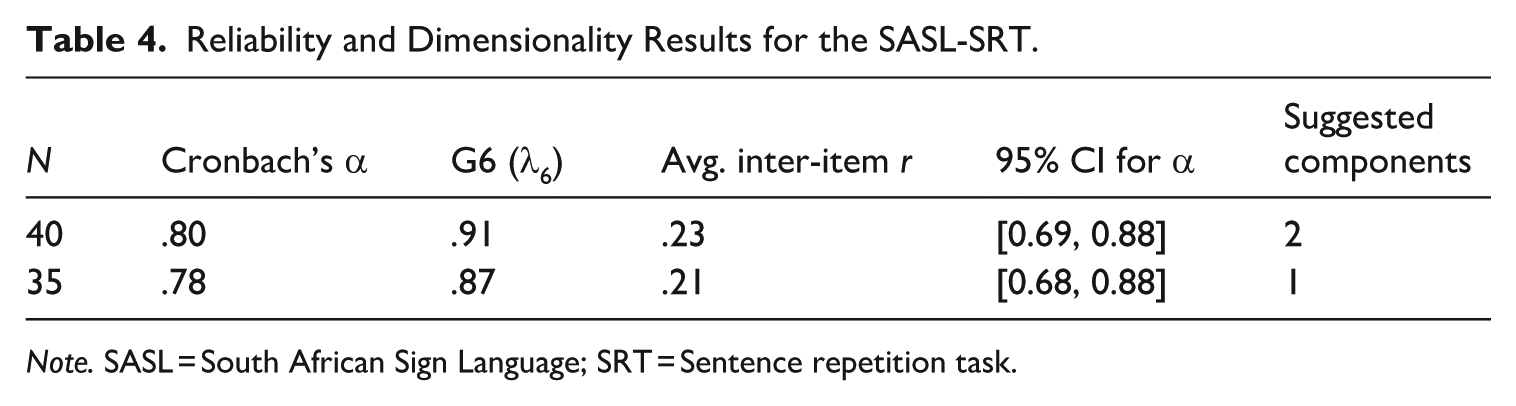
Note. SASL = South African Sign Language; SRT = Sentence repetition task.
Item-level analysis revealed a range of item difficulties, with most items contributing positively to overall consistency. Several items displayed limited variance and were excluded from the filtered analysis due to non-informative response patterns (all participants scoring 0). For the filtered set, parallel analysis on tetrachoric correlations and the Kaiser rule each indicated a single dominant component, 6 supporting the interpretation that the SASL-SRT functions as a reasonably reliable, essentially unidimensional measure for this developing group.
Because 6 sentences were adapted between the child and adult versions, as discussed in the Materials section, we conducted a like-for-like comparison on the 14 unchanged items. This alignment situates children’s performance against an adult benchmark without confounding by adapted content. Reliability on the shared set was acceptable for children and high for adults, as indicated in Table 5. 7 Adults scored higher on average, with greater spread, than children. Item difficulties were uniformly higher in the adult group than the child group, and adult-corrected item–total correlations were broadly positive and moderate.
Psychometric Summary on 14 Shared Items (S6, S7, and S15–S18 Excluded).

On reduced totals (max = 14), children scored M = 2.03 out of 14 (SD = 2.01; median = 1; range 0–8) and adults M = 5.43 out of 14 (SD = 3.70; median = 5; range 0–13). Floor and ceiling effects were low for both groups (children: 22.9% at 0, 0% at ceiling; adults: 14.3% at 0, 0% at ceiling), with a clear rightward shift in the adult distribution consistent with higher proficiency and the post-hoc item adaptations.
Participant and Item-Level Predictors of Sentence Repetition Accuracy
To account for repeated measures across items and participants, we fitted a generalised linear mixed effects model. The binary outcome variable indicated whether a child produced a correct repetition (1) or not (0). Fixed effects included chronological age, AoA, school (sum-coded −1/+1; levels “School 1” and “School 2”), sentence length (in number of signs), and the presence of NMM (binary: 1 = present, 0 = absent). Random intercepts were included for both participants and items to account for repeated measures. Adding gender (M vs. F) left all other estimates virtually unchanged and did not improve model fit (Change in Akaike Information Criterion ≈ +1; Likelihood Ratio Test p = .49). This variable was, therefore, omitted in the analysis.
A Pearson product-moment correlation was conducted to test for collinearity between age and AoA. The analysis revealed a small, positive correlation that was not statistically significant, r(38) = .14, p = .38, 95% CI [−0.18, 0.44]. This indicates that there was no reliable linear relationship between age and AoA in the sample and, therefore, no concerns with respect to collinearity of these variables.
A VIF analysis, in turn, indicated no problematic multicollinearity among the predictors (all VIFs < 1.2). Residual diagnostics suggested no major violations of normality or homoscedasticity.
Model parameters were estimated via maximum likelihood with Laplace approximation.
Table 6 provides the mixed effects model results (N = 35; centred predictors; sum-coded factors). Age was a significant positive predictor of item-level accuracy; each additional year increased the odds of a correct reproduction by about 160%. Later AoA was associated with lower odds of correctness, with each one-year delay reducing the odds of a correct response by approximately 28%. School showed a large effect relative to the grand mean; School 1 was roughly 53% lower than the grand mean, whereas School 2 was roughly 112% higher. For the direct School 2 versus School 1 contrast, see Table 7. This suggests systematic differences between institutions. Sentence length had a strong negative effect, as longer sentences sharply reduced accuracy. Adding an additional sign reduced the odds of producing an accurate response by over 80%. NMM presence, while negatively associated with performance, showed no reliable effect. A sensitivity model including all children (N = 40) produced the same pattern, with AoA negative but trend-level (OR = 0.78, p = .068) and all other effects materially unchanged.
Mixed Effects Logistic Regression Results.
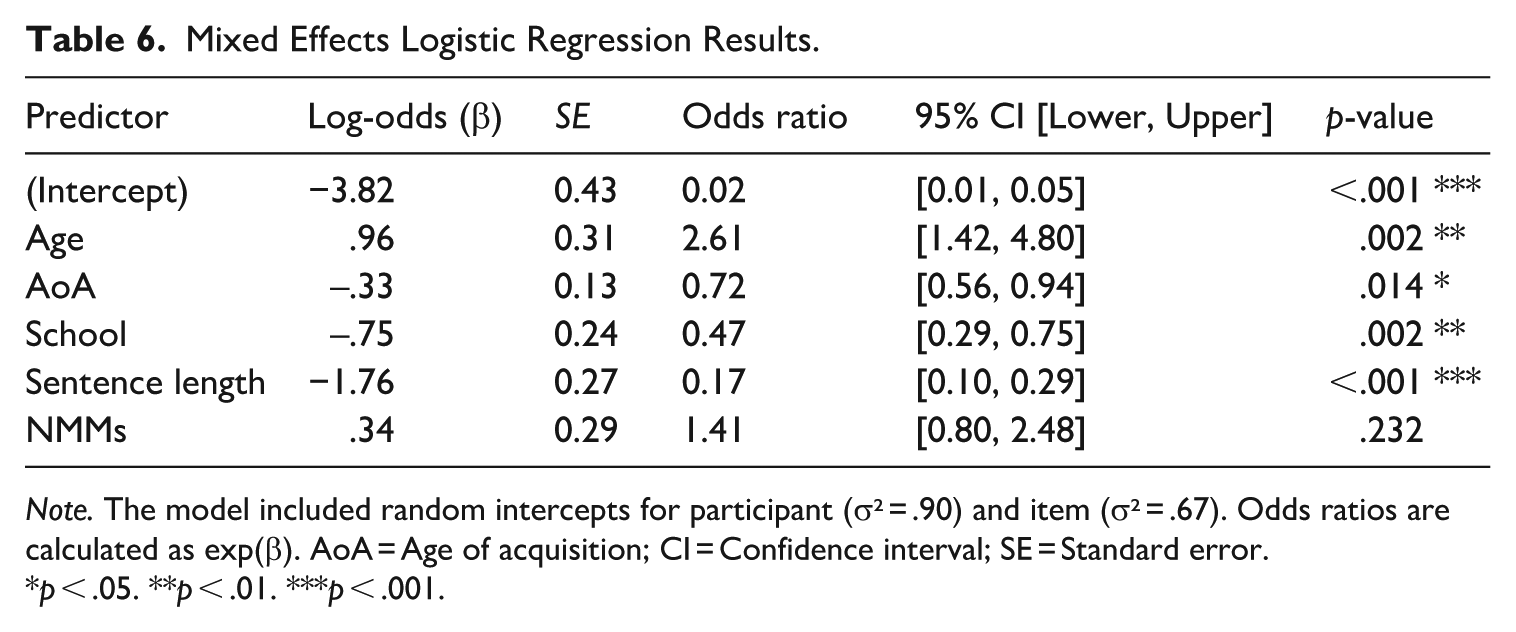
Note. The model included random intercepts for participant (σ² = .90) and item (σ² = .67). Odds ratios are calculated as exp(β). AoA = Age of acquisition; CI = Confidence interval; SE = Standard error.
p < .05. **p < .01. ***p < .001.
Equivalent Pairwise Contrasts for Two-Level Factors.
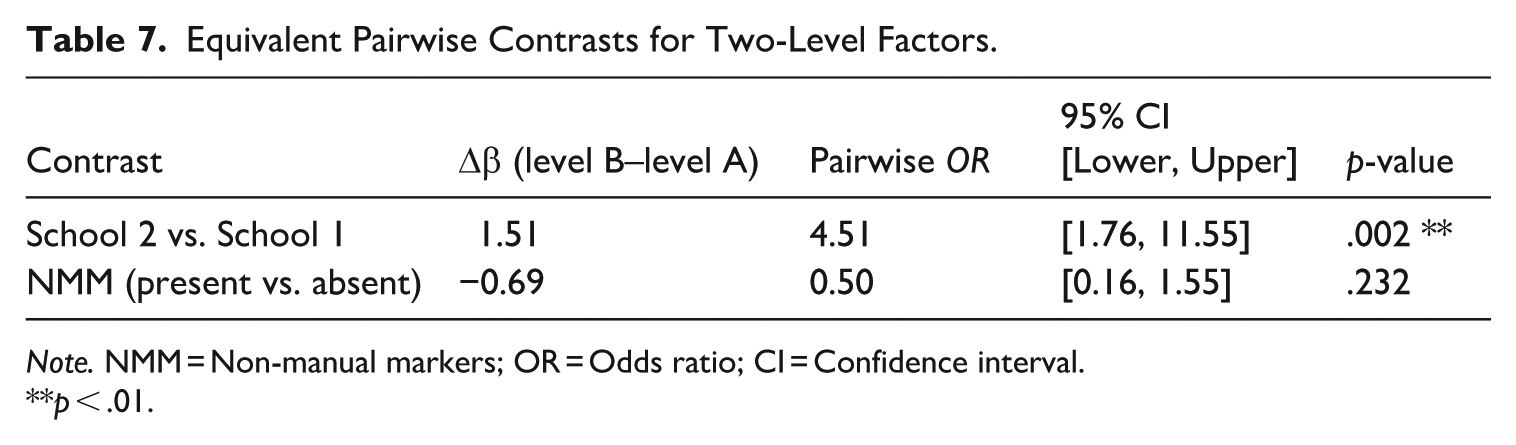
Note. NMM = Non-manual markers; OR = Odds ratio; CI = Confidence interval.
p < .01.
Sentence-level accuracy ranged from 0% (S12, S14–S16, and S18–S19) to 57% (S1). Six sentences had 0% correct responses, and these were all between five and seven signs long. There is not enough research on SASL to determine a valid complexity measure, but the sentences with estimated greater grammatical complexity sometimes contained fewer manual signs and resulted in more correct answers (for example, sentence 2 in Figure 1).
Although the model estimates a 50% reduction in odds with the presence of NMMs, the association was not statistically significant. There were many errors with NMMs, predominantly omission. The NMM for negative sentences (headshake) was, however, mostly correct (83% of relevant responses) with few omissions. This non-manual marking can be optionally paired with a manual negative sign in SASL (Huddlestone, 2021). This is as may be expected from research with children who have native exposure to a sign language (Anderson & Reilly, 1997; Van den Bogaerde, 2000), which shows that non-manual marking of negation is acquired early. Even a child in this study with less than 2 years of exposure to SASL had mastered this marking.
Other NMMs involving eyebrow movement had a much lower percentage of responses matching the model (11%–35%). Very little is known about the acquisition of such markers in other sign languages but a study of ASL (Reilly et al., 1991) indicated that it was only around 6 or 7 years of age that children finally manage proper coordination of wh-signs and the wh-NMM (lowered eyebrows).
Discussion
The SASL-SRT appears to function as a psychometrically sound tool for assessing sentence-level repetition ability in young SASL users. Reliability metrics indicate consistent performance across items (α = .80; G6 = .91). This is encouraging given the limited item set and the variability in children’s backgrounds. Items with limited variance were probably too difficult for the children at this age and should be refined in future iterations with children. The limited sample size and item variance means that findings need to be confirmed by larger studies with wider age groups.
The comparative analysis with an adult reference group (N = 35) reinforces the test’s internal reliability and supports its dimensional coherence. When aligned on the 14 shared sentences, reliability remains acceptable in children and high in adults, and a one-factor structure holds in both cohorts. Adult performance situates the low child scores as difficulty-driven rather than measurement failure, and highlights which sentences are too hard or non-discriminating for younger signers. While further refinements and confirmatory validation are required, these results collectively suggest that the SASL-SRT is a valid and reliable instrument for measuring sentence repetition in both developing and fluent SASL users.
The overall performance of children on the SASL-SRT was low, with a mean score of 2.2 out of 20 (11%) and a positively skewed distribution. While concerning at first glance, this low performance aligns with existing findings in sign language acquisition studies, where delayed exposure to a signed language often results in reduced morphosyntactic and lexical proficiency (Mayberry, 2010; Mayberry & Kluender, 2018). The children in Schönström and Hauser’s (2022) STS-SRT study had a mean of 5.86 out of 31 (19%), and a range of scores of 3% to 45%. As such they performed better overall than the children in this study, but the range of scores was similar. However, the children in the STS-SRT study were older (10–16 years old) and had much lower AoAs (only two children had an AoA higher than 2 years old). Furthermore, the scoring of the STS-SRT excluded NMMs, making the two studies not strictly comparable.
The inclusion of NMMs, which adds precision and ecological validity, may have contributed to the low scores as this introduces potential scoring bias and demands greater training for scorers (see Hauser et al., 2008; Schönström & Hauser, 2022). However, although the inclusion of NMMs was associated with lower odds of correct responses, this relationship failed to reach conventional levels of statistical significance.
It is interesting to note that the comparison of the adult and child scores on the 14 common SASL-SRT items show a clear differentiation, with the adults mean score being 38.8%, compared to 14.5% in the children. The overwhelming majority of children only produced between 0 and 3 correct responses. As noted in relation to Table 2, 70% of the children in this study had delayed acquisition (first exposure to SASL after age 3). This indicates that many children were still in the early stages of SASL acquisition, despite their age.
Both chronological age and AoA emerged as significant predictors of repetition accuracy, as hypothesised and as previously observed by Bogliotti et al. (2020) and Schönström and Hauser (2022), among others. However, the effect of AoA on repetition accuracy was weaker than chronological age. Chronological age, age of diagnosis, and age of first exposure to SASL were typically reported by parents in years and did not include months. This highlights the difficulty of using a background questionnaire with a population of this nature. Eliciting more precise data would clarify the importance of these factors. Further investigation with a larger sample size would also strengthen the current findings.
Five children in our study with an early AoA scored low, due to the number of skipped and unanalysable responses (see Table 5) and were excluded from the model analysis. It can only be speculated what the reasons for these responses were. Unanalysable responses may reflect task misunderstanding, overconfidence, or even divergent sociolinguistic goals (e.g. narrating or role-playing). It is possible that the children who produced unanalysable responses saw the task as an opportunity to show off their language skills and ignored the instructions. In other studies, responses of this type have not been reported. As noted in the methods section, we repeated the same model on all 40 children as a sensitivity check. The results were materially unchanged (age positive, sentence length negative, and school difference large). However, AoA remained negative but only at trend-level (OR = 0.78, p = .068). This emphasises the importance of future research using SRTs being alert to these types of responses.
Inclusion, post-hoc, of school as a factor revealed unexpected significant differences in performance between institutions. After controlling for age and AoA, school still accounted for a substantial portion of variance. The significant effect of school on repetition accuracy may indicate that children at School 1 were unused to formal testing formats or expected evaluative repetition so that they felt less pressure to follow instructions exactly or to provide an exact match response. Even when the five children, all from School 1, who produced more than 30% unanalysable or skipped responses were removed from the sample, the model analysis still indicated a significant school effect. This suggests the probable variability of the language learning environment, including differences in teaching approach, teacher proficiency in SASL, opportunities for interaction with fluent signers, and the availability of rich and consistent input. As has been documented in the South African context, many DHH learners, once in school, receive limited native-like input due to a lack of deaf teachers or fluent SASL users, as discussed in the section on the factors influencing language acquisition. However, these observations remain speculative at this time as no relevant data on the differences between the schools could be collected. Potential differences between schools, in terms of pedagogy and assessment procedures, should be considered in the planning and administration of SRTs in future research.
Conclusion
This study contributes much-needed data on L1 acquisition of SASL, a severely understudied area. The results support previous findings that emphasise the necessity of early diagnosis of deafness and the importance of early and sustained access to a natural language for linguistic development. Early diagnosis can lead to earlier exposure to a sign language. Our findings show that older participants tend to score higher, reflecting the cumulative benefits of age-related development. However, it is clear from the background questionnaire data (Table 2) that children’s chronological age is not always an indicator of how long they have been exposed to SASL. AoA is dependent on the age of diagnosis of deafness and then, in turn, the age of first attendance at a school for DHH children. Earlier AoA significantly improves performance, suggesting that interventions targeting earlier acquisition may yield better outcomes.
The difference between the results from School 1 and School 2 are suggestive of the importance of educational context. Given the challenges in ensuring native or near-native input at school, future studies should investigate ways of increasing exposure to fluent SASL – through video resources, family education, or increased recruitment of deaf professionals in schools. In addition, the inclusion of adult data in future SASL-SRT research could provide valuable developmental baselines and allow for comparison across age groups (Schönström & Hauser, 2022). Future work should also examine how SASL proficiency (as measured by SRTs or other methods) correlates with literacy, cognitive development, and academic outcomes. Longitudinal studies would also help trace the developmental trajectory of children with varying AoAs and exposure histories.
The results of this study have implications not only for educational planning but also for medical and early intervention services, and services providing information to parents. Professionals involved in diagnosis, audiology, and early childhood care must be equipped to offer timely referrals and to provide parents with accurate, accessible information about the importance of early sign language input.
Supplemental Material
sj-docx-1-fla-10.1177_01427237251400454 – Supplemental material for Learning South African Sign Language as a First Language – The Results of a Sentence Repetition Task
Supplemental material, sj-docx-1-fla-10.1177_01427237251400454 for Learning South African Sign Language as a First Language – The Results of a Sentence Repetition Task by Kate Huddlestone and Anne E. Baker in First Language
Footnotes
Acknowledgements
The authors are grateful to Amy Palmer and the staff at the two schools for the deaf for assisting with data collection, to the children and parents for being willing participants, to Modiegi Njeyiyana and Zulfah Shabodien for assisting with the creation of the SRT materials, and to Robyn Berghoff for assisting with the statistical analysis.
Ethical Considerations
The method, materials, and procedure of the project were approved by the Stellenbosch University Research Ethics Committee: Human Research (Humanities) (9091).
Parents/legal guardians provided written informed consent on behalf of the children. The children also gave their written assent.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was partly supported by a South African National Research Foundation (NRF) Human and Social Dynamics grant HSDI170602236563. Any opinion, findings, and conclusions or recommendations expressed are those of the authors and do not necessarily reflect the views of the NRF.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.