
Abstract
Objectives
Transgender people in the UK face uncertainties and inequalities in healthcare provision, especially for treatment required for gender transition. Existing studies have found that doctors’ ideological tendencies, in particular socially normative conceptions of gender, influence their treatment of gender minority patients. This study explores doctors’ understanding of their role in transgender care, their thoughts on the current processes in place to enable gender affirmation, and their theoretical views of sex/gender that underpin these conceptions.
Design
One-on-one, semi-structured online interviews. Clinicians were recruited through societies representing both specialties and then snowballed. Recruitment stopped with data sufficiency, according to the tenets of ‘information power’. Data analysis was conducted in line with Braun and Clarke’s Reflexive Thematic Analysis guidelines.
Setting
UK doctors working in general practice and endocrinology.
Participants
Convenience and purposive sampling of 16 participants (8 endocrinologists and 8 general practitioners).
Main outcome measures
Our dataset explores clinicians’ conceptions of their role in transgender care and identifies current structural and organisational obstacles.
Results
The interviews found that the division of labour in transgender care is contested. GPs felt their role was to understand the patient’s narrative, and therefore were reluctant to prescribe, believing this to be within the purview of specialists. Endocrinologists described themselves as ‘technicians’ simply carrying out the task of providing hormonal treatment. Almost all interviewees emphasised the importance of multidisciplinary involvement, and none were willing to treat without a mental health professional.
Conclusions
Our findings suggest that doctors may inadvertently communicate gender norms, but that they do so within the constraints of a system over which they have limited control, and that their conceptions of transgender care are informed by serious resource pressures. We offer some practical suggestions for how these pressures could be ameliorated.
Keywords
Introduction
The historical relationship between doctors and transgender people has been marked by deep entwining, and consequently, by misapprehension and friction.1,2 Transgender respondents to the 2018 National LGBT Survey reported lack of knowledge among medical staff, fear of discrimination, inappropriate curiosity and long waiting lists as contributing factors to their negative experiences when accessing general healthcare services. 3 Gender identity provision for children, in particular, has received extensive media scrutiny following the 2024 publication of a review by Dr Hillary Cass, commissioned by NHS England. 4 This review acknowledged that many clinicians have concerns about their competence to work with this population and cast doubt on the quality of the evidence base for interventions for gender incongruence and dysphoria. It was not received without contention: the British Medical Association council took the rare step of censuring a report and commissioning its own alternative study. It is within this context that our study has relevance.
In the 2021 UK census, roughly 262,000 individuals identified as transgender, and 30,000 as non-binary. 5 This population is served by 20 UK adult gender identity clinics (GICs), which have average waiting times of 52 months from referral. The clinics provide psychological assessment, counselling and peer support. If patients are approved for further treatment, the GICs are the gateway for state provision of hormonal and surgical therapies. The present centrality of doctors to this process is controversial.2,6 Transgender people in the UK need a doctor (or psychologist) to obtain legal recognition in the form of a Gender Reassignment Certificate, as well as any gender-affirming treatment, although this is currently being reformed in Scotland. Some transgender activists have tried overturning this medicalisation of gender incongruence. In the recent Diagnostic and Statistical Manual of Mental Disorders (DSM-5), the entry for ‘Gender Identity Disorder’ has been replaced with ‘Gender Dysphoria’. This is more than just semantics: gender incongruence – the knowledge that one’s gender does not align with sexual characteristics – is no longer a medical condition. 7 The resulting negative affect – gender dysphoria – is still classified as a psychiatric illness, which some argue maintains pathologisation.5,7,8
Waiting times for gender identity assessment have placed increasing responsibility with general practitioners (GPs). The Royal College of General Practitioners notes that many of its members lack experience in transgender health and that the gaps in ‘education, guidance and training … needs to be urgently addressed’. 9 Surveys in North America have assessed endocrinologists’ and primary care doctors’ preparedness-to-treat, finding that clinicians were more willing than ready. Clinicians identified unfamiliarity with the transgender community, insufficient training, diagnostic overshadowing and lack of experience as significant barriers to effective care.10–12 A recent study examining UK healthcare professionals’ perspectives on transgender health highlighted structural, educational, cultural and technical barriers. 13 While this research, which found that significant resource pressures inform doctors’ experiences, focused on GPs and mental health workers, our study includes both GPs and endocrinologists to examine how these shortages affect provision of transgender care across the UK health system. To our knowledge, no other study has concentrated on this grouping. Interviewing both primary and secondary care doctors allowed us to explore how key barriers to treatment play out along this patient journey, including discontinuities in care, difficulties in multi-disciplinary working and struggles over prescribing responsibilities.
Ethnographic work has drawn attention to the underlying ideological structures that shape doctors’ decisions to treat transgender patients, highlighting medicine’s ‘essentialist’ investment in sex differences.14–16 This reported emphasis on classifying patients into two distinct gender poles can translate into difficulty navigating consultations with patients who do not define as either male or female. 17 While this body of work has usefully drawn attention to the norms underpinning medical intervention, it can read as if doctors, with a monolithic ‘medical gaze’, invented sex by committee.18,19 Narratives of gender transition are rich and contradictory; we hypothesised that doctors may have similarly multifarious understandings. 20 Our study examines the interplay between clinician’s theoretical conceptions of gender variance, and their practical experience in this area, which have hitherto been discussed separately. Rather than assume that doctors always mould people into binary genders, we propose that they shuttle between understandings that are specific to the biomedical sciences, and wider cultural norms; they bring ethical, legal, financial and social concerns to consultations with transgender patients, which emerge as much from structures of care as from their personal opinions.
It is within this background of doctor–patient power relationships, the resource pressures of the NHS, and clinicians’ uncertainties of the intricacies of the transgender narrative that we approached the design of this project. Overall, we aimed to discover how doctors mediate sex in ways that stem from both their theoretical commitments and practical exigencies, with the view that a deeper understanding of their motivations and theorisations can usefully bolster transgender care in the UK. 19
Method
Recruitment
We recruited trainee and qualified GPs and endocrinologists with past, present or anticipated care of transgender patients. Institutional Review Board (IRB) approval was granted (BSREC.156/20-21). We sent invitations to participate to organisations representing both specialties, and a smaller organisation representing practitioners of gender medicine. We also utilised our own social networks as medical students, and asked senior colleagues to approach established doctors in the field, using an approved advertisement. Participants were then purposively snowballed, which we deemed necessary due to the relatively small number of endocrinologists. Participants were not compensated for involvement. Informed consent was obtained electronically. We recruited 16 participants, all cisgender (we asked participants to define their gender identity at the beginning of the interview), six of whom identified as female and 10 as male (Table 1).
Participant demographic data.
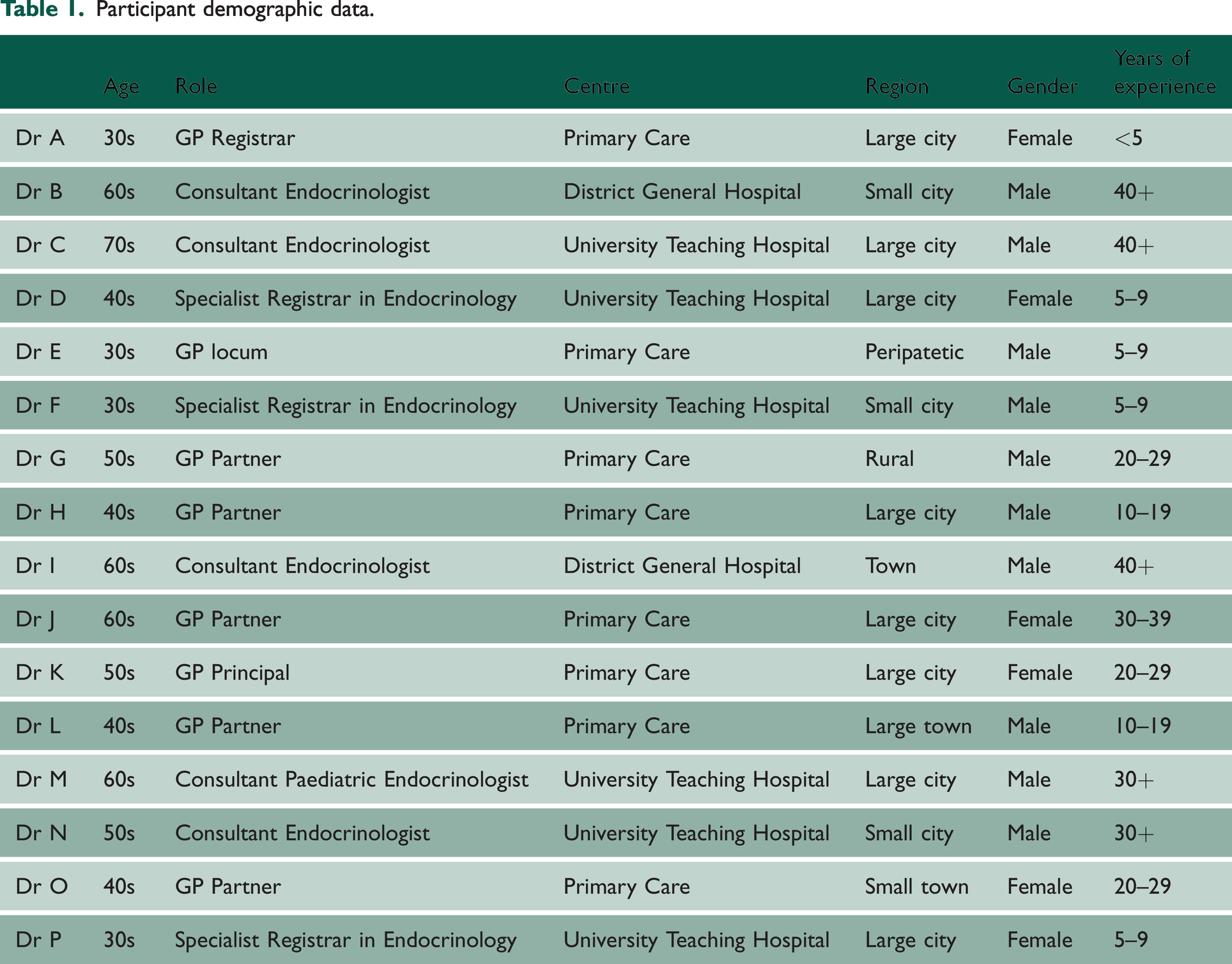
Sample size was guided by ‘information power’: the number of participants needed to reach ‘data sufficiency’ (rather than ‘saturation’). 21 Instead of attempting to determine the hypothetical sample size at which no new codes would emerge (saturation), an ‘information power’ approach holds that the sample size should be in inverse proportion to the quality of information held by the sample population. A more specialised field, with experienced practitioners, and a well-developed existing theoretical literature requires fewer interviewees than an investigation of an uncharacterised broad field.21,22 In this study, nine participants reported over 20 years of experience, with their interviews offering copious material. In line with the tenets of reflexive thematic analysis, this does not necessarily mean that all possible responses have been exhausted, but rather that the ‘selected patterns’ offer enough material to extend and challenge our existing theoretical understanding of this topic.21–23
Interview design
The interview schedule (Supplementary Appendix SA1) was initially formulated around themes from existing literature focusing on the clinical experience of transgender care, and theories of sex and gender. It was then iteratively redesigned to adapt to emerging foci. The interviews lasted from 25–60 minutes and were conducted over Microsoft Teams by the two first authors in 2021–2022, who were medical students at the time.
Data analysis
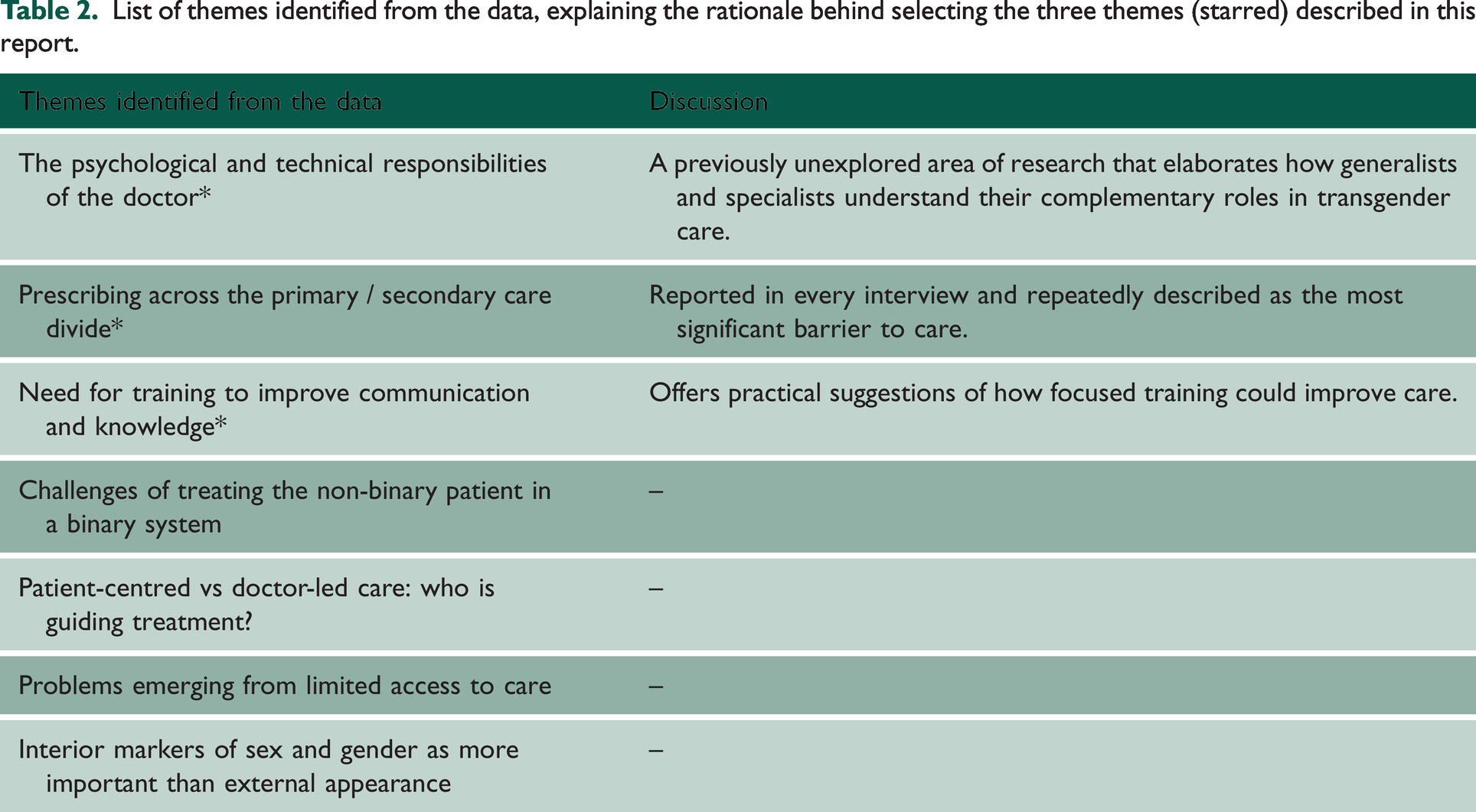
We followed the guidelines for reflexive thematic analysis as developed by Braun and Clarke. 23 Interview transcripts were auto-generated by the video call software. Each interview was conducted by one of the two first authors; the other verified and anonymised the transcript. Transcripts were then re-read by both authors, for familiarisation with the dataset, and then inductively coded independently using NVivo for Mac. Major themes were generated by each author and then discussed to encourage validity and representativeness. Finally, themes were mapped against concerns from the existing literature. We chose themes using two criteria: (1) representativeness to the dataset, and (2) ability to contribute to prescient issues in transgender health research. Seven themes were identified, but for brevity, we have focused here on three that we believe are the most exigent (Table 2).
List of themes identified from the data, explaining the rationale behind selecting the three themes (starred) described in this report.
Results
‘I know my language isn’t adequate’: training needs in transgender medicine
Many doctors felt that they had not received enough training in transgender medicine. Our respondents used alternative sources of information: academic research, expert patients, YouTube videos and younger family members. Dr G reported that he would ‘ask my children what it means’. Dr L noted that ‘I’ve got kids and they’re very, very open about this stuff’. This reinforced the sense of transgender care as a generational issue amid changing social norms. Our respondents deferred their understanding of transgender issues to their patients and wanted their use of terminology to be patient-led (‘common courtesy’ according to Dr G). While this approach shows less political dogmatism than some studies report, it risks turning patients into ‘reluctant educators’. 24
There were three clusters of thought about what training might improve transgender care. First, many doctors wanted a general level of training to be offered to all staff. This would include measures to reduce unconscious bias, present correct terminology (including pronoun usage) and dealing with inherently gendered situations. For example, binary gendered wards lead to transgender patients being placed in side rooms away from their specialty, which evocatively renders them ‘outliers’ in hospital nomenclature. Second, some endocrinologists advocated general medical training to support transgender patients with physical comorbidities. Dr F had ‘heard experiences of people who went to see a cardiologist and they said, “‘I'm transgender’” and the cardiologist said, “I've got no idea what you're talking about. Please go home and book another appointment with someone else”’. Dr M imagined a ‘trans man with abdominal pain’: How do you sensitively take a history and make a diagnosis in a situation like that, you know, with respecting the person’s gender identity? … Clearly something like pregnancy is a differential diagnosis, for instance. All these things are challenging, and all doctors need to know how to deal with that.
Third, some GPs requested training on peer support and organisations to which patients could be signposted. A few GPs thought that patient perspectives and case studies would provide more exposure to transgender voices, while those who anticipated being asked to continue private prescriptions requested more pharmacological training. Although two experienced GPs were happy with the current provision of training, reporting that they saw relatively few transgender patients, most doctors were keen for further learning opportunities. The endocrinologists-in-training described the difficulty of gaining clinical experience in gender clinics ‘with enough frequency to understand what’s happening’ (Dr D). Many of our respondents, echoing studies from North America, thought lack of training was compromising care. 26
‘Second violin, really’: specialty roles in transgender care
Every doctor interviewed described the importance of a multi-disciplinary team in managing gender transitions, and few respondents saw themselves as leaders. Two main roles emerged from the interviews, which we labelled ‘technicians’ and ‘supporters’. An endocrinologist described his role as looking after the patients’ ‘best interests in hormonal terms. In that sense, I’m almost a technician’ (Dr C). Another endocrinologist described his position as ‘second violin’, with mental health teams leading the orchestra (Dr M). This had implications for their theorisation of their patients’ gender roles. One endocrinologist questioned whether he was involved in gender ‘transition’: ‘transition … implies to me that they’re in the process of changing, whereas most of those I’ve seen have been fairly established in their gender roles’ (Dr C). He saw his role as the biochemical confirmation of a pre-existing, settled, gender decision.
By contrast, many GPs figured their roles as ‘supporters’ and signposters: they saw patients at an earlier stage of gender incongruence, where they may not have a full understanding of their own gender identity. Dr J, who regularly saw transgender patients, stated that she ‘luckily’ does not have to make ‘the decision’ of where a patient’s gender identity should be treated to, so she could be ‘guided by them’. Dr K saw this as intrinsic to the field: ‘it doesn’t feel odd [for GPs] to be guided by a patient’s narrative’. When GPs were asked to maintain hormone regimens, they found this to be ultra vires. One GP described this in trenchant terms: ‘You wouldn't ask a plumber to deal with your electrics, or you would be very stupid … and the plumber would be very foolish too’ (Dr H). This division of labour – into emotional and technical work – reflects Isabel Menzies’ thesis that the division of the patient into multiple body systems defends against clinical anxiety. 27 Rather than any individual doctor taking on the overwhelming responsibility of remodelling someone’s sex, the clinicians helping patients consider their gender identity sequestered their role from those implementing the change.
Psychiatry had a particularly fraught role. Some scholars have called for the removal of gender identity treatment from the purview of mental healthcare.6,8 However, no doctor we interviewed was willing to treat without the input of a mental health professional. This was not because our respondents saw gender incongruence as a psychiatric disorder. Instead, doctors emphasised the difficulty of dealing with the psychological consequences of biographical disruption. Dr E, a GP who had served many transgender patients, thought psychiatric services were needed ‘from start to finish’ to ‘help with stigma’ post-transition. Dr K, a GP, reiterated she did not ‘feel that the person has a pathology, just that [psychological services should be] available to have support’. Dr K explicitly located the pathology in social stigma and suggested that psychological support would not be necessary if society ‘was kinder and more open’. One endocrinologist thought psychiatrists earned their place because they were ‘more trained’ in being ‘less judgemental’ than other specialties (Dr I).
Other interviewees proposed that psychiatrists were needed as transgender people might be at greater risk of psychopathology. Some attached this to the ‘psychological comorbidities that go with trying to figure out what gender you are’ (Dr F). It was suggested that transgender people may have histories of abuse or family breakdown: one GP noted that many transgender patients had changed their surnames, which she took as a sign of disrupted familial relations. She imagined that changing one’s sex involves ‘incredibly drastic’ changes to the body and new ways of interacting socially,28,29 and she noted the ‘courage it takes to … and the distress that must have been underlying to want to go down that route’ (Dr J). It is noteworthy that although many transgender patients acknowledge co-existing psychological pressures from gender variance, many studies have reported a suspicion of mental health involvement, such as feeling pressure to conceal distress to present as a ‘perfect patient’. 25 In one study, a transgender man described avoiding going ‘to the GP for medication for mental health [as it might] risk the referral [not] being put through’. 30 A concern about underlying psychological pathology slows down care by mandating psychological assessment prior to treatment. The relationship between comorbid psychological distress and gender diversity, if it exists, is an argument for swifter treatment. Many doctors interviewed noticed the remission of mental health concerns after medical affirmation therapy.
‘How am I gonna get my Zoladex?’: prescribing hormone therapy
Many GPs were concerned about hormone therapy prescription practices, especially in the transition between primary and secondary care. The reasons included gender clinics expecting primary care doctors to absorb the prescription costs, GPs lacking experience in prescribing these medications off-licence, differences between primary and specialist care formularies and GPs’ mistrust of assessments performed at private clinics. GPs were cautious about the legal responsibility of prescribing medication for unfamiliar uses: ‘Even though I might have a professor of gender identity medicine giving me advice, if it's ultimately my prescription … then I am liable’ (Dr H). The lack of best practice guidance compounded this anxiety. Dr E was concerned that testosterone therapy could increase risk of cardiac issues. There is ‘nothing to say how to treat people … I looked it all up that night and there’s very little data on cholesterol levels in … men taking oestrogen, women taking testosterone’.
Some interviewees thought that any personal discomfort on the part of the GP should not affect prescribing practices: ‘It's a bit like the GPs who used to refuse to prescribe contraceptive pills … You were obliged to signpost the patient to someone who would’ (Dr H). More formal signposting might counteract the phenomenon, noted by many interviewees, of transgender patients resorting to word-of-mouth to find a willing doctor, creating clusters of demand in certain surgeries. One GP’s surgery had formulated internal guidelines for continuing hormones to encourage consistency between the partners.
Doctors who were willing to prescribe emphasised the ‘sense of relief’ (Dr B) that their patients expressed: I will tell them right at the onset that I’d be perfectly happy to give you the female hormone, the male hormone and supervise you, but I would like to know a lot more about – a bit more about – your background as it were. So I put them at ease, because usually what happens is that they have to do a presentation to me, as it were, that's what they feel, about ‘why I want to be male’ or ‘why I want to be female’ but I say, right, OK, you've made your mind up. That's fine, I can supervise you now. (Dr B, endocrinologist)
Many researchers have discussed the pressures on transgender patients to present a coherent narrative during medical consultations, which may ride roughshod over the idiosyncrasies of their gender identity.14,15 Our respondents showed how pressures in service provision, such as delays in prescribing, may contribute to this. Doctors should be aware that patients’ anxieties about the provision of their hormone therapy may lead to these self-misrepresentations.
Discussion
Our respondents were aware of the medical, psychological and social complications of gender affirmation but felt that they were often required to work beyond their core expertise. GPs resented being asked to take on responsibility for specialist care without further training; endocrinologists were not willing to manage care without multidisciplinary support. This study corroborates existing findings that have noted significant barriers to care, and shows that doctors are aware of, and frustrated by, the limited gender identity services available.11,13 However, while much of the sociological literature asserts that doctors ‘sort out’ transgender patients into binaristic and normative narratives of gender dichotomies, we suggest that doctors are less ideologically consistent, and more marked by theoretical ambivalence, educational uncertainty and material pressures.14–16,31 Like recent research from other European countries, we found that while doctors were increasingly willing to treat transgender patients in non-pathologising ways, the restricted access to care occasioned by austerity measures had more of an impact on doctors’ experiences than any totalising ideological commitment. 32
There were some strong thematic consistencies from participants: a need for quicker multidisciplinary support, concern about the cause of increased numbers seeking gender identity treatment and anxiety related to the long-term effects of medication. While many respondents found the current state of UK transgender care to be unsatisfactorily slow and dishearteningly disjointed, it has an ethical urgency for patients. Delays and inadequacies in care contribute to an increased burden of psychological distress among transgender patients and is possibly a factor in the increased mortality of transgender people.33,34
By speaking to both primary and secondary care doctors, we can report recommendations that would aid both hospitalists and generalists. These recommendations were formulated by correlating issues raised by patients in other studies with the perspectives that we have gleaned by interviewing clinicians on the root causes of these issues. They are delineated in Table 3.
Recommendations for clinical and administrative change.
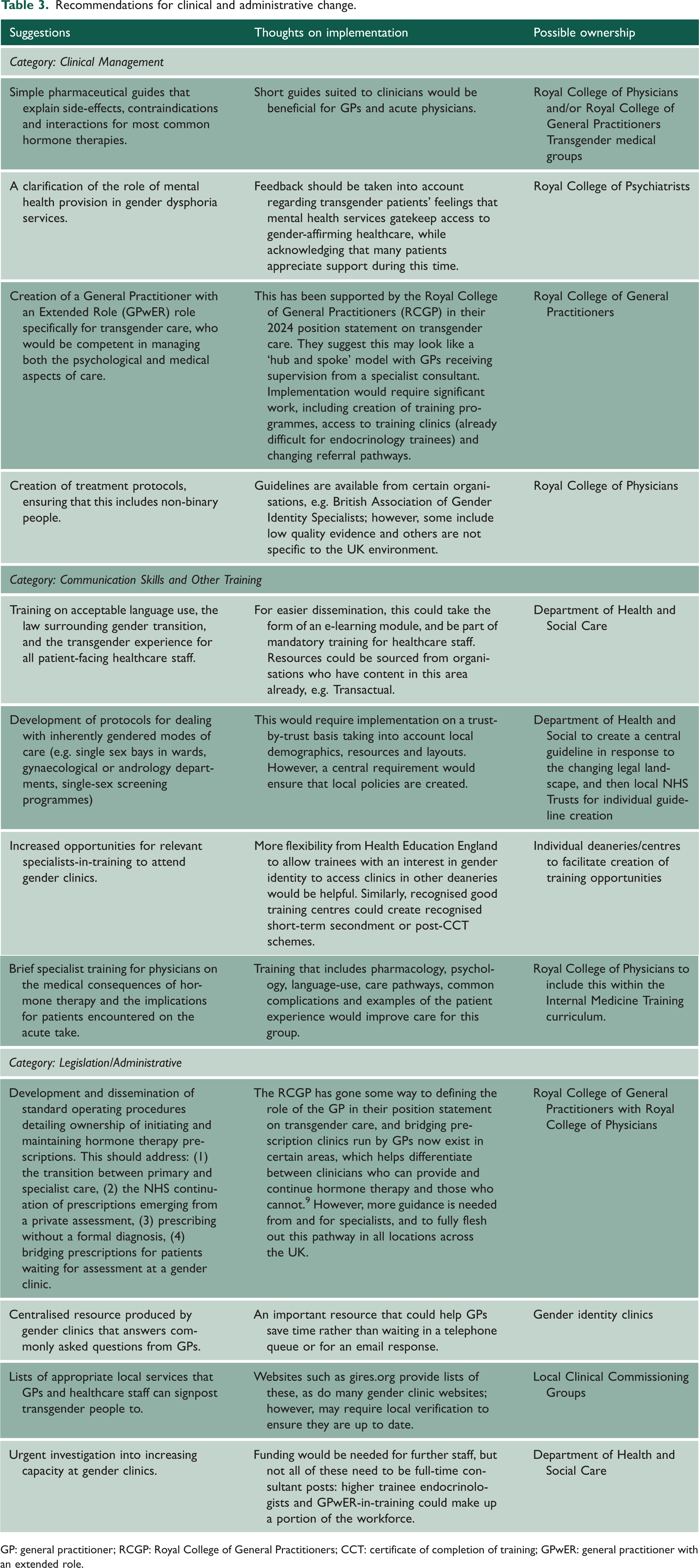
GP: general practitioner; RCGP: Royal College of General Practitioners; CCT: certificate of completion of training; GPwER: general practitioner with an extended role.
Limitations
This study offers a novel account of cisgender clinicians (although two described themselves as gender-fluid) with varying degrees of interest and experience in transgender care. We were unable to recruit any gender minority clinicians, despite advertising through LGBT medical networks, as the pool of endocrinologists, in particular, is limited. Transgender practitioners would be likely to have particularly rich insights, and would be able to account for the effect of clinical pressures on those seeking and providing care. Future work that explores these experiences might help bridge the binary between the provider and the patient.
Our participants were all prepared to treat transgender patients. We note that some doctors who were invited refused due to lack of interest in, or suspicion of, the field. Many spoke to us of colleagues who used delaying tactics or poor practice to avoid treating transgender patients, but none admitted to doing this themselves: a study designed to elicit doctors’ reasons for refusing to treat transgender patients could make a crucial contribution. This study also predominantly recruited clinicians working in urban centres, although did have respondents working in rural general practice. Transgender patients living in rural areas report facing more difficulty transferring their care to different doctors or hospitals. 35 Further research targeting rural doctors, who see fewer transgender patients but may not be able to use referral to opt-out of transgender care, would offer insights into improving services for patients with the fewest options.
While this study helps characterise doctors’ understandings of working with ‘transgender patients’, it is important to note that this is a heterogenous community, including non-binary, gender variant and gender fluid people, some of whom will never seek medical treatment. Fluidity is particularly central in children, for whom gender identity often evolves with other aspects of social development. While any non-cisgender patients can face misunderstanding, misgendering and hostility, the constituent groups may face different challenges, depending on the type of medical care they seek. Our endocrinologists mostly reported feeling comfortable with the hormonal technicalities of treating non-binary adults, but they found the process not adequately accounted for by existing guidelines or hospital structure. This research elucidates the difficulties for clinicians of managing both the psychological and pharmacological aspects of gender transition. Further research that helps improve care for children questioning their gender identity, and for non-binary and gender fluid people of all ages, some of whom may want improved care without needing hormonal treatment, emerged as particularly urgent.
Conclusion
As the first study that combines UK doctors’ theorisation of their role in the management of gender incongruence and their thoughts on the material circumstances of transgender care, this article supports existing research that highlights the importance of resource pressures. Doctors felt unprepared for the increased demand for gender affirmation care. They lacked a clear structure for managing treatment, including uncertainty about their professional role, pathways for providing continuity of care, and for accessing up-to-date information or advice on the side effects of treatment. They were concerned that a shortage of specialist services meant that transgender patients were treated without nuance or due care, and that most clinicians were not ready to take on an expanded role. Transgender medicine is compartmentalised with significant barriers to accessing specialist care, and then further obstacles to having care continued in the community. We found that endocrinologists were comfortable with initiating hormone therapy but lacked a framework for evaluating or following up patients. GPs were required to use assessments from unknown private providers or compel patients to wait years for an appointment at a gender dysphoria clinic. They shared their patients’ feelings that the current system is not adequate for the increased demand for gender identity care. Our findings suggest that doctors are willing to be led by their patients’ formulations of their gender identity, but few clinicians have the resources and training to manage both the technical and psychosocial aspects together.
Supplemental Material
sj-pdf-1-jrs-10.1177_01410768251363407 - Supplemental material for How doctors think about their role in transgender care: a qualitative study of UK general practitioners and endocrinologists
Supplemental material, sj-pdf-1-jrs-10.1177_01410768251363407 for How doctors think about their role in transgender care: a qualitative study of UK general practitioners and endocrinologists by Jonathan Franklin, Apoorva Thakur and Vinod Patel in Journal of the Royal Society of Medicine
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.