
Abstract
Objectives
The number of deaths occurring in private homes in England and Wales had been rising for years, increasingly rapidly from 2020. Media stories and research linked decomposing bodies found in private homes with pandemic-related social isolation. We aim to explore whether these incidents are one-offs or part of a wider trend.
Design
Descriptive analysis of publicly available Office for National Statistics (ONS) data.
Setting
England and Wales.
Participants
All residents of England and Wales, 1979 to 2020.
Main outcome measures
Using data from the Office for National Statistics, we calculate European Age Standardised Rates for deaths coded as R98 (‘unattended death’) and R99 (‘other ill-defined and unknown causes of mortality’) in the 10th version of the International Classification of Diseases (ICD-10), and the corresponding codes in ICD-9, by sex and age group from 1979 (when ICD-9 began) to 2020. These are proxy markers for deaths where decomposition precludes attribution of a specific cause at postmortem.
Results
While mortality from all other causes decreased from 1979 to 2020, the opposite was seen for deaths from R98 and R99 (or ‘undefined deaths’), with men more affected than women. There was a sharp rise in these deaths in both sexes but in men particularly in the 1990s and 2000s, coinciding with a time when overall mortality was rapidly improving.
Conclusions
The increase in people found dead from unknown causes suggests wider societal breakdowns of both formal and informal social support networks. They are concerning and warrant urgent further investigation. We call on national and international authorities to consider measures that would make it possible to identify these deaths more easily in routine data.
Keywords
Introduction
In July 2022, the British magazine The Spectator published an article ‘The mystery of Britain’s surging at-home deaths’. 1 It reported how deaths at home began to rise during the first year of the pandemic in 2020, and that this trend had continued into 2022. However, the rise in deaths at home pre-dates the pandemic. The Office for National Statistics (ONS) reports that the number of deaths occurring at home has been rising since 2007, with a sharp spike in 2020 due to the coronavirus disease 2019 (COVID-19) pandemic. 2 Excess deaths at home continued into 2022. 3
The Spectator story coincided with other media reports of individual deaths. While the increase in deaths at home would not necessarily be a problem, the reported cases raised concerns that there may be a wider problem of growing isolation and lack of social support. For example, Sheila Seleoane, aged 58 years, died in a London social housing block in 2019 – and was not discovered for over 2 years, by which point her body was severely decomposed. A subsequent investigation severely criticised her housing association for repeated failures to follow up on missed contacts.4,5 Laura Winham, aged 38 years, was found ‘mummified’ in 2021, more than 3 years after she had died. 6 Her family blamed care and welfare services for neglecting her. There have been other anecdotal stories of this kind, which have suggested that the reduction in the availability of care and welfare services since 2010 may have contributed to the possible trend.
Against the backdrop of rising deaths at home, as well as growing evidence about the adverse consequences of a decade of austerity, there are concerns about whether those deaths of people found decomposed that have attracted media attention reflect a wider problem. Ideally, it would be possible to track trends in numbers of deaths found decomposing at home, but these data are not routinely coded in national statistics. Furthermore, the existing literature on deaths at home is largely focused on palliative care, recognising that, for many, a ‘good’ death at home is a desirable outcome. However, there are two studies, both from London, linking a significant increase of severely decomposed bodies since the beginning of the first lockdown to social isolation.7,8 Neither looked at longer-term trends, so it is prudent to extend this analysis further back, especially as deaths at home had been increasing before the pandemic, and both deaths cited above were believed to have occurred before 2020, even if the bodies lay undiscovered during the pandemic.
In this exploratory article, we attempt to discover whether there was any increase in the number of people found to be in a state of decomposition at the time of postmortem over time from 1979 to 2020 in England and Wales. We suggest that if we find an increase in bodies found to be in a state of decomposition at postmortem, it would raise concerns about social isolation and neglect both after and before death and might be considered a proxy for a failure of society to safeguard its members.
Methods
Using ICD codes as a proxy for severe decomposition.

ICD-9 and ICD-10 codes used for proxy described in Box 1 for ‘undefined deaths’.

ICD: International Classification of Diseases; NOS: not otherwise specified.
Second, we extract deaths due to R98 and/or R99 (ICD-10) and equivalents in ICD-9 from 1979 to 2020 by 5-year age group and sex.16,17 These data were extracted from all deaths, not deaths disaggregated by place of death (such as at home). However, most deaths that occur outside the home are in a hospital, care home or hospice environment and would therefore be extremely unlikely to end up in a state of decomposition with the R98/R99 code as they would either have a known diagnosis or undergo a postmortem. The very few others outside the home would, almost always, show evidence that could be used to ascertain the cause, such as major trauma causing fractures, or be found in circumstances that would indicate the cause, such as a body pulled out of the sea or being found wearing outdoor equipment on a mountain. In these cases, a cause of death should be able to be given, such as drowning, exposure or violence. Deaths that occur not-at-home, which lead to such severe decomposition that they are given a cause of death as 1a Unascertained, are likely extremely rare (and probably forensic/police cases).
Finally, using the European Standard Population 2013, 18 we calculate the European Age-Standardised mortality rates over time. We excluded all deaths under the age of 20 years due to changes in how sudden infant death syndrome and sudden unexplained death syndrome were coded and recognised throughout the decades examined.
Results
Deaths at home 2006–2021
Figure 1 presents deaths aged 28 days and over at home as a proportion of all deaths from all causes by sex, 2006 to 2021 in England and Wales. 9 This shows a consistently higher proportion of total male deaths at home than women, with a slight narrowing of the gap during the first two years of the pandemic, increasing over time from 16% in 2006 to 21.4% in 2019 and 26.5% in 2021 for women, and from 22.4% (2006), 27.4% (2019) to 31% (2021) for men. When we disaggregate by age group, we see the highest proportion in those aged 15–44 years, followed by those aged 45–64 years.

Deaths at home as proportion of total deaths, 2006–2021, by sex, England and Wales. Authors’ calculations based on data from ONS 2022.9
Standardised mortality rates for ‘undefined’ deaths (R98/R99) and all other causes from 1979 to 2020 by sex
Next, we present age-standardised rates (ASR) of ‘undefined’ deaths (those coded R98 and R99 and ICD-9 equivalents) and all other causes of death by sex for England and Wales 1979 to 2020 (Figure 2). Please note, absolute numbers for these can be found in Table A and Figure C in Supplementary Appendix II. We indicate where the ICD version changed from ICD-9 to ICD-10 to highlight where we might expect to see any artefact due to the transition. For both sexes, the ASR for all other causes decreased steadily over time, with some fluctuations, until stalling after 2010 and increasing in 2020, when the pandemic began. The undefined deaths panel shows the opposite, with an increase for both sexes from 1979 to 2020. For women, the greatest increase is between the mid-1990s to mid-2000s, after which it stabilises. For men, there appear to be two periods of increase, first in the 1990s then again in the early 2000s. By the 2000s, the male rate is more than double the female rate. Note due to the small numbers, over-interpretation of the annual fluctuations should be avoided.
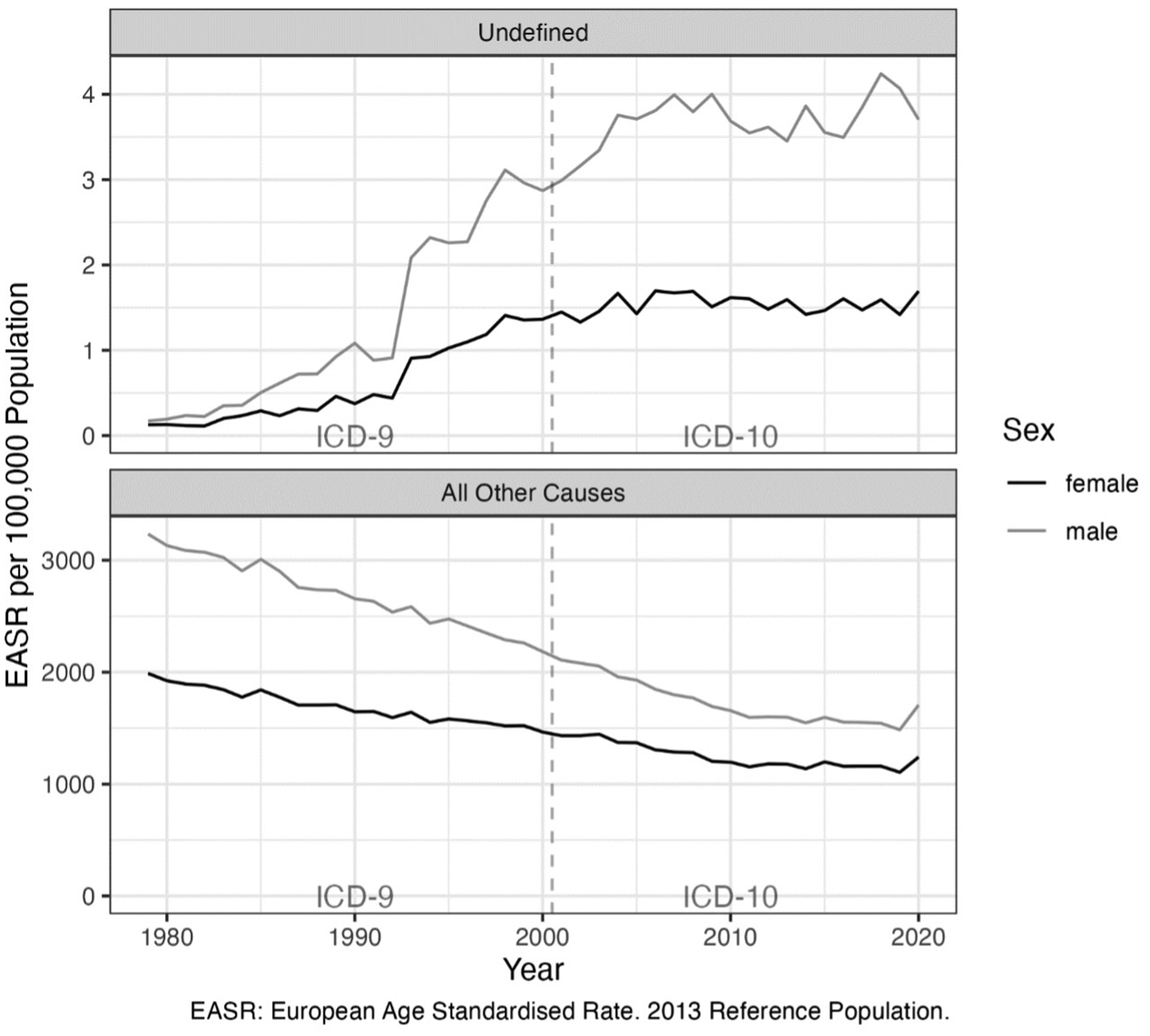
European age standardised rates for ‘undefined’ deaths (i.e. those coded R98/R99) and all other causes of death by sex, England and Wales, 1979 to 2020. Dashed vertical line indicates change in ICD version from ICD-9 to ICD-10 in 2001. EASR: European Age Standardised Rate.
Standardised mortality rates by broad age group
Next, we explore ASRs by broad age group: working years (20–59 years), and older (60 years and over) (Figure 3). These shows similar patterns for both age groups, with a consistently higher rate for men than women (approximately three times as high).
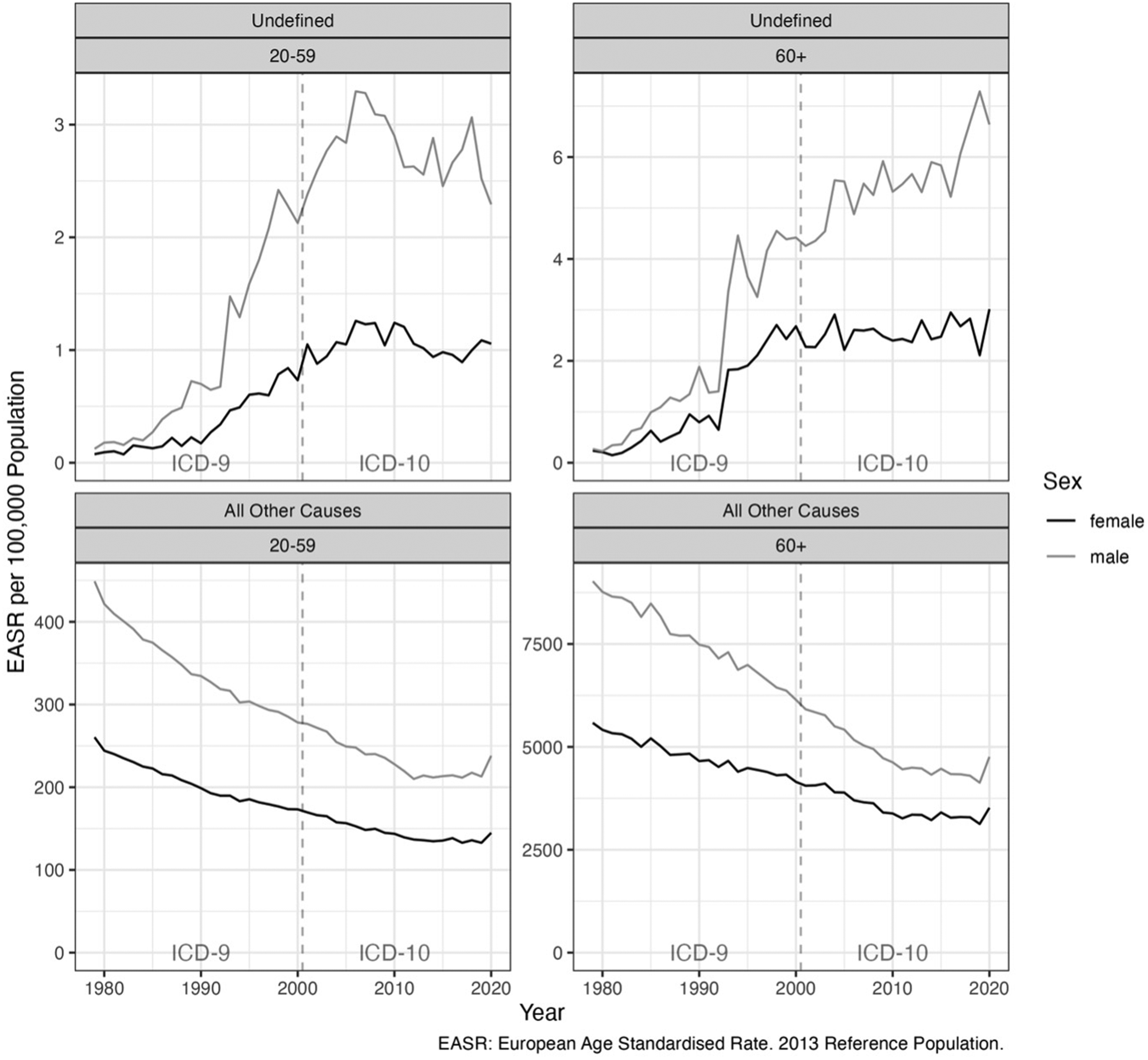
ASRs by broad age group (20–59 years, 60+ years) for men and women, 1979–2020, England and Wales. Dashed vertical line indicates change in ICD version from ICD-9 to ICD-10 in 2001. Note y axes are variable. EASR: European Age Standardised Rate.
We also present the same data indexed to 1980 (Figure 4). This makes it easier to see how relative trends in both undefined and all other causes of death have gone in very different directions. Caution is required in interpretation as it may give the impression that the two trends balance each other out. This is incorrect, as undefined deaths are many orders of magnitude rarer than deaths from all other causes.

Indexed trends in EASRs (the year 1980 = 100) by broad age group (20–59 years, 60+ years) for men and women, 1979–2020, England and Wales. Dashed vertical line indicates change in ICD version from ICD-9 to ICD-10 in 2001. Note y axes are variable. EASR: European Age Standardised Rate.
Discussion
Main findings of this study
We present preliminary findings analysing deaths of people likely to have been found decomposed, using a proxy marker of ICD codes. 2 We have argued that any increase in this measure can be considered as a proxy for long periods of neglect after death and that this, in turn, may be a proxy for prolonged neglect and social isolation before death. This may be a marker of breakdown in formal and informal social support networks. This said, it is important to acknowledge that decomposition is a complex process, caused by many individual and environmental factors, and the speed of it can vary greatly. 19 However, we focused on those deaths where decomposition has reached the stage where it was no longer possible to determine a cause of death. Our reading of the literature suggests that, except in exceptional circumstances such as a summer heatwave or a death in a very hot room, to reach severe decomposition would take some time and would strongly suggest that the deceased was extremely isolated in the perimortem period. Furthermore, while changes in variables such as medical conditions and ambient temperature do matter, on a large population scale, the most important factor that would affect decomposition is postmortem interval, while individual or environmental circumstances would likely be balanced over time. The average body mass index has increased in recent decades, and this can increase postmortem decomposition speed, 20 but this is unlikely to be as important a factor relative to the overall postmortem interval.
We were concerned that recent reports of people found decomposed could signify a longer-term trend that would point to growing failure of society to prevent people falling through the gaps in the welfare state during a prolonged period of austerity and becoming socially isolated. We confirmed that this increase has occurred, and over a prolonged period, the earlier part of which predates austerity. Interestingly, loneliness and isolation are often associated with ageing, as exemplified by National Health Service advice on countering it, 21 with a perception that older women are especially vulnerable, given their longer life expectancy than men. However, while we did find an increase in bodies found decomposed in older women, the rates increased at an even faster rate for both younger and older men, with a rapid increase in the 1990s and 2000s. The increase seen for both sexes in the 1990s and 2000s is particularly surprising given the substantial improvements seen in mortality during this period. There is some suggestion that these deaths may be more common in those born between 1975 and 1985 (see Supplementary Appendix II) but, if true, we can only speculate as to a reason.
What is already known on this topic
From 2012 onwards, trends in mortality worsened, a phenomenon that has been linked to the austerity measures implemented from 2010.22–25 Initially, older age groups were most affected, with the first increase in mortality seen in older women in 2012, and soon after, more groups were affected with now widespread worsening of mortality outcomes for many groups. For example, an increase in mid-age mortality has been reported in the UK in recent years, in particular from so-called ‘deaths of despair’ (i.e. deaths related to drug and alcohol use, or suicide).26,27 However, it important to note that, while the underlying social changes that give rise to these deaths may be similar to those studied here, in particular those that lead to greater social isolation, any substantial overlap is unlikely as, in most cases, a specific cause will be able to be allocated to these deaths of despair by means of toxicological detection of drugs or in overdose with suicidal intent, or from other evidence indicative of suicide. That said, the rise in these deaths could also be a reason for more deaths of men found at home, decomposed, who may have also been socially isolated.
Social isolation and loneliness are increasingly recognised as bad for health – two 2023 meta-analyses found associations with an increased risk of all-cause mortality.28,29 In the analysis of postmortem reports ‘every markedly decomposed case that died at home lived alone’. 7 Data on people living alone in the UK between 1996 and 2021 show significant differences by age group and sex (see Figures D and E in Supplementary Appendix II).30,31 At ages 25–44 years, almost double the number of men than women live alone, according to the latest data, but numbers in both sexes have decreased over time. At ages 45–64 years, the difference is smaller but remained by 2021, but while numbers of women were slightly higher until 2004, both have increased, with men diverging around 2007 after which there was a marked increase. At ages 65 and over, both sexes have seen an increase since 2014. However, here the gender difference is reversed, with a greater number of women living alone than men, although the data demonstrate that the ratio of men living alone relative to women has almost doubled in the 65 and over age group from 1996 to 2021. 30 This should be interpreted with caution as, first, these are crude numbers and do not take into account the population structure, i.e. there are more women than men in the older population (see population pyramid in Figure E in the Supplementary Material).31,32 Second, men have lower life expectancy than women and, in a heterosexual marriage, the husband is less likely to be left alone than the wife due to the death of their spouse, as husbands usually die before their wives.
This changing landscape of living arrangements could in part explain the rise in undefined deaths for both sexes, but specifically the accelerating rise in men relative to women. However, living alone is only one factor contributing to perimortem social isolation. Family, friend and local community social connections can also be expected to play an important role, but these factors are harder to quantify at the population level so data that might show any change in these parameters over time are sparse and fragmentary.
What this study adds
Using a proxy for severe decomposition, we have shown an increase over time among both sexes in ‘undefined’ deaths (which we propose as a proxy for found decomposed). In addition, it found that more deaths among men are coded ‘undefined’ than women in both working age and older groups, suggesting a higher rate of being found decomposed.
Limitations of this study
To our knowledge, the ICD-10 codes R98 and R99 (and equivalents) have not previously been used as a proxy for severe decomposition. These codes will miss those cases where the body is decomposed but with postmortem findings, which can still establish a defined cause of death (for example, as mentioned, in the study of postmortems before and after the pandemic lockdown only 16% of severely decomposed bodies had an unascertained cause of death). 7 Nonetheless, these ICD codes may still act as a reasonable surrogate given that, in the same study, almost all unascertained deaths did demonstrate severe decomposition. However, we cannot say with certainty that these codes are a good proxy for advanced decomposition. There is a paucity in research describing exactly how often decomposed deaths lead to an unascertained cause of death, as the majority of deaths where bodies were found decomposed would still result in a cause of death being given. While the numbers are small in the limited existing research, and although we have demonstrated a possible relative increase in the frequency of unascertained deaths, the absolute number of decomposed bodies as a proportion of all deaths remains low, and so the number included in any potential further studies would be low, and further research in this area would be useful.
Severe decomposition or degradation of a body is the most likely reason for the final cause of death to be given as ‘unascertained’. There may be rare exceptions, such as coronial or administrative issues, which can lead to an ‘unascertained’ cause of death, such as the body being repatriated following an autopsy abroad. However, pertaining to our findings of an increase in this proxy, it may be that more causes of death were reported as ‘unascertained’ in the past, and ICD-9 code ‘sudden death, cause unknown’ may have been used prior to the acceptance of conditions such as SADS or SUDEP. If sudden death syndromes such as these were previously coded as R99 and equivalents, we would have expected to see a decrease in deaths coded as ‘undefined’ over time, but we found the opposite, i.e., that deaths have increased.
Unanswered questions and future research
We are sharing these results in the hope of stimulating further research. Examples include whether there is a more suitable proxy for a body found in a state of decomposition, or whether our proxy is considered valid by experts in the field. We also hope to encourage others to report preliminary findings, and to raise the alarm about a possibly concerning trend that is challenging to investigate. Furthermore, future research may want to further explore the effects of living alone on mortality and, in particular, being found decomposed.
All bodies found in a state of decomposition should be referred for postmortem; however, research using coroners’ reports is challenging, given variation in reporting across the country. Notably, the two cited studies were undertaken in an individual city.7,8 Furthermore, we cannot easily link the anonymised, coded death data to compare to individual postmortem reports to validate whether the proxy is indeed appropriate.
Recording bodies found decomposing would be a useful addition to publicly available data. Thus, while recognising that the duties of coroners are strictly delineated in law, 33 we encourage the Chief Coroner of England and Wales, the Coroners’ Society for England and Wales (and their counterparts in Scotland and Northern Ireland), to explore whether and how they might report whether the deceased was severely decomposed or not. This could permit decomposition data to enter public record and subsequently be coded and analysed by the ONS in a similar way to other mortality data such as cause of death and place of death. In the longer term, we would encourage the World Health Organization to consider adding a code to indicate advanced decomposition to the ICD, perhaps using the ‘U’ chapter, which allows for the adoption of new codes to address emerging concerns, as has been done with COVID-19 and vaping. 34
Conclusion
Many people would be shocked that someone can lie dead at home for days, weeks, or even longer, without anyone raising an alarm among the community they live in. Being found decomposed after days, weeks, months or even years might indicate a high level of neglect, but this is speculative without further investigation. We share these inconclusive and preliminary results in the hope of encouraging others to take up this important topic, and we propose that future mortality data could include information about the severity of postmortem decomposition to enable further investigation into this topic.
Supplemental Material
sj-pdf-1-jrs-10.1177_01410768231209001 - Supplemental material for A deathly silence: why has the number of people found decomposed in England and Wales been rising?
Supplemental material, sj-pdf-1-jrs-10.1177_01410768231209001 for A deathly silence: why has the number of people found decomposed in England and Wales been rising? by Lucinda Hiam, Theodore Estrin-Serlui, Danny Dorling, Martin McKee and Jon Minton in Journal of the Royal Society of Medicine
Supplemental Material
sj-pdf-2-jrs-10.1177_01410768231209001 - Supplemental material for A deathly silence: why has the number of people found decomposed in England and Wales been rising?
Supplemental material, sj-pdf-2-jrs-10.1177_01410768231209001 for A deathly silence: why has the number of people found decomposed in England and Wales been rising? by Lucinda Hiam, Theodore Estrin-Serlui, Danny Dorling, Martin McKee and Jon Minton in Journal of the Royal Society of Medicine
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.