
Abstract
Objectives
A range of public inquiries in the English National Health Service have indicated repeating failings in complaint handling, and patients are often left dissatisfied. The complex, bureaucratic nature of complaints systems is often cited as an obstacle to meaningful investigation and learning, but a detailed examination of how such bureaucratic rules, regulations, and infrastructure shape complaint handling, and where change is most needed, remains relatively unexplored. We sought to examine how national policies structure local practices of complaint handling, how they are understood by those responsible for enacting them, and if there are any discrepancies between policies-as-intended and their reality in local practice.
Design
Case study involving staff interviews and documentary analysis.
Setting
A large acute and multi-site NHS Trust in England.
Participants
Clinical, managerial, complaints, and patient advocacy staff involved in complaint handling at the participating NHS Trust (n=20).
Main outcome measures
Not applicable.
Results
Findings illustrate four areas of practice where national policies and regulations can have adverse consequences within local practices, and partly function to undermine an improvement-focused approach to complaints. These include muddled routes for raising formal complaints, investigative procedures structured to scrutinize the ‘validity’ of complaints, futile data collection systems, and adverse incentives and workarounds resulting from bureaucratic performance targets.
Conclusion
This study demonstrates how national policies and regulations for complaint handling can impede, rather than promote, quality improvement in local settings. Accordingly, we propose a number of necessary reforms, including patient involvement in complaints investigations, the establishment of independent investigation bodies, and more meaningful data analysis strategies to uncover and address systemic causes behind recurring complaints.
Introduction
Patient and family complaints (hereinafter: complaints) are increasingly recognised as a critical source of insight for quality improvement. Representing complex narratives of healthcare failures, complaints include social, institutional and clinical problems not always identified by hospital-driven monitoring systems (e.g., incident reporting systems, case reviews), 1, 2 and have been associated with hospital mortality rates and adverse surgical outcomes. 3, 4 Critically, most patients and families submit complaints to prevent harm from occurring to others, 5 but are currently often left dissatisfied. 6, 7
In the English National Health Service (NHS), which receives over 200,000 formal complaints per year, failures to detect and respond to harm and negligence reported in complaints have been illustrated across a range of public inquiries (e.g., The Mid-Staffordshire Inquiry, The Shipman Inquiry, Morecambe Bay Investigation). 8 –10 In acknowledgement of these failures, several reforms were introduced to improve learning from complaints, such as the regulatory requirements for hospitals to formally investigate and collect data from complaints. Yet, as the most recent Inquiry at The Shrewsbury and Telford Hospital NHS Trust has unfolded, it appears that system-wide progress has been limited (Table 1).
Key inquiries and policy reviews indicating failings in learning from complaints in English NHS hospitals.
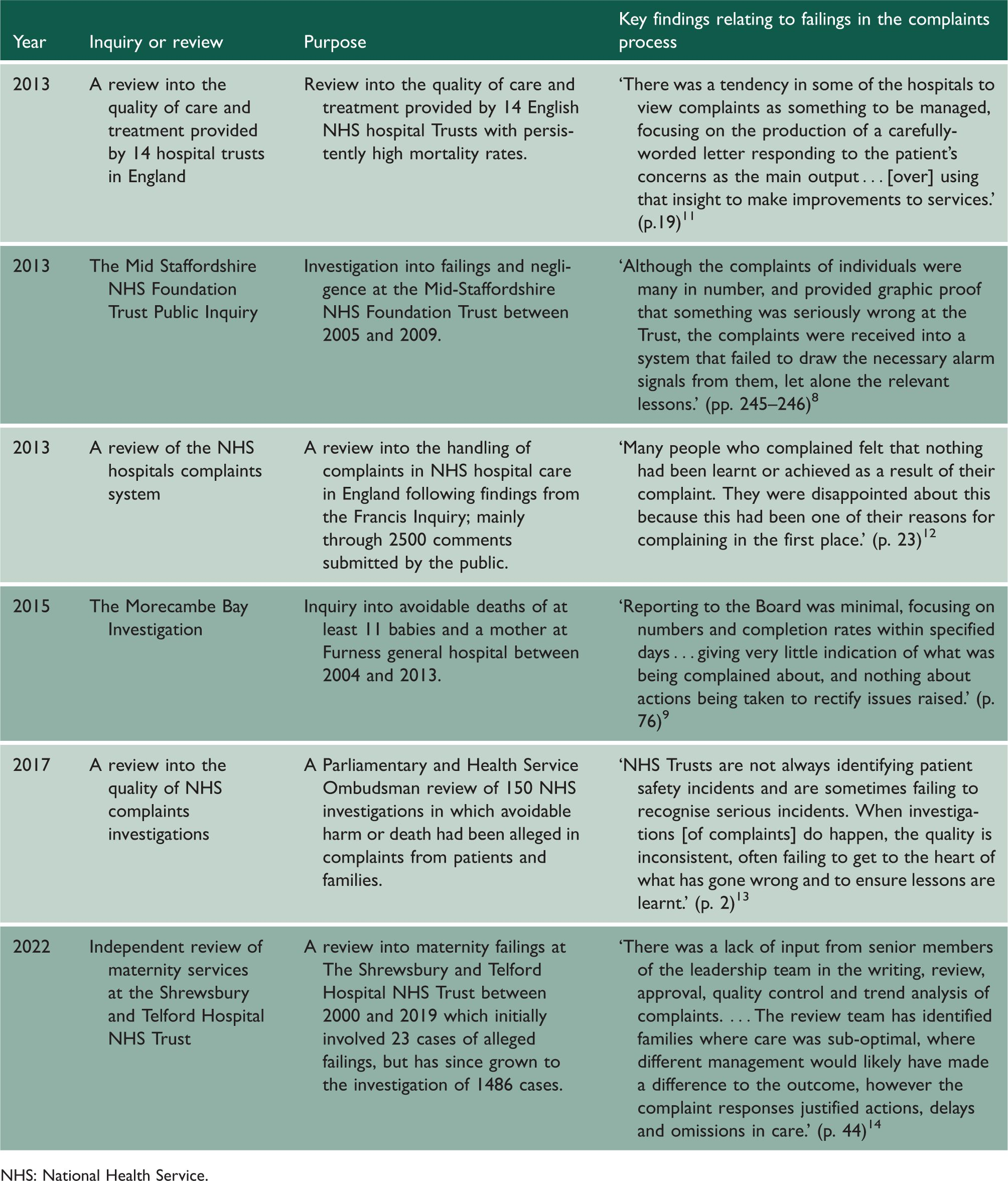
NHS: National Health Service.
The complex, bureaucratic nature of the NHS complaints system is often cited as an obstacle to effective complaint handling, but a detailed examination of how such bureaucratic rules, regulations and infrastructure shape complaint handling, investigation and monitoring within institutions has yet to be conducted. This study sought to examine how national policies structure local practices of complaint handling, and how are they understood by those responsible for enacting them within local practice.
Methods
Study setting
This study was conducted at a multi-site acute NHS Trust in London (England) which consists of five acute sites and a range of community services. The trust was selected based on convenience. The lead researcher was located at the Trust, but had limited pre-existing relationships with the complaints department or frontline. The most recent 2018 Care Quality Commission inspection report at the time of study described the Trust as treating complaints seriously and deriving lessons from investigations. The site was therefore considered an ‘information-rich case’ 15 to explore complaint handling, relative to existing evidence that is mainly generated in poor performing hospitals through public inquiries. A distinctive feature of this Trust is the presence of a centralised complaints department with designated non-clinical ‘investigators’, who occupy a certain degree of distance from frontline practice. The Trust is one of the largest in the country, with an average of over 1,000 complaints per year between 2015 and 2019.
Participants
Staff were recruited using purposive sampling supported by the complaints manager and frontline contacts. This enabled the identification of relevant staff roles with systematic involvement in complaint handling or with direct experience of receiving a complaint (Table 2). Efforts were made to recruit across different levels of seniority, service types and sites within the Trust. The number of participants per staff group reflects their relative degree of involvement in complaint handling.
Description of participants by staff group.
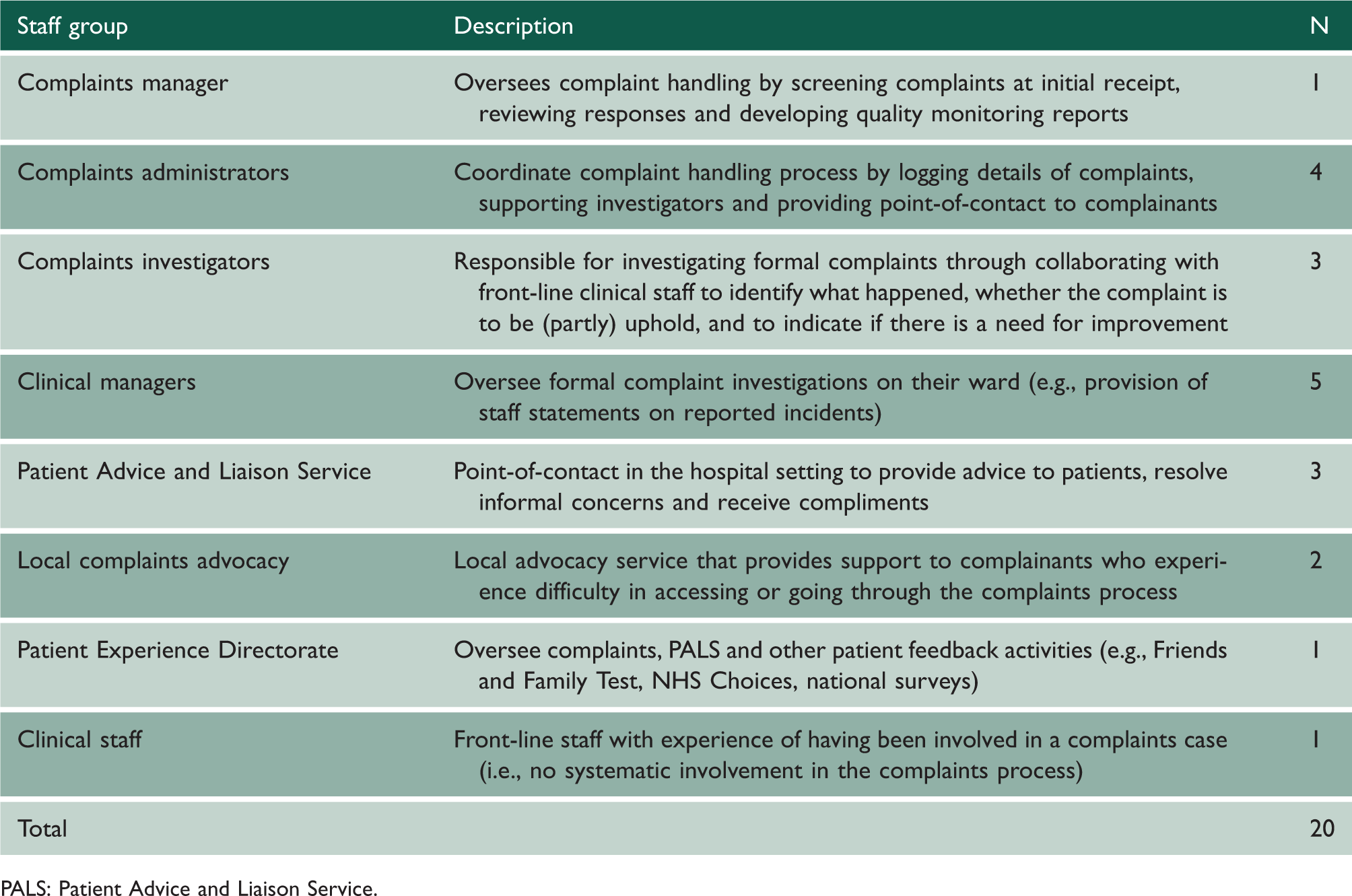
PALS: Patient Advice and Liaison Service.
Procedure
Semi-structured interviews were held at the organisation’s main hospital between June 2018 and June 2019, lasting an average of 43 minutes (range 10–81 minutes). Interviews were shorter when interviewees had limited regular involvement in the complaints process (e.g., front-line clinical staff). Questions explored staff understandings of how complaints handling routine is enacted. Inconsistencies, workarounds and adverse impacts were explored through follow-up questions, such as through using alternative representations (‘interesting, staff member X said Y’) and problem prompts (‘what happens if [unexpected problem]?’). 16 The topic guide was developed based on informal observations, document analysis and scoping of existing literature on complaint handling. Informal observations included five hours of shadowing, attending meetings in the complaints department, and informal conversations with the complaints manager and advocacy service. Document analysis included a review of national regulation and policy reports, organisational complaints policy and workflow charts, and hospital records.
Data analysis
Interviews were audio-recorded and transcribed verbatim. Data were analysed thematically by the lead researcher (JD, social scientist). Open codes were initially developed based on transcripts and documentation, which were then grouped into higher-order organising themes. 17 A sample of four interviews was also coded by a second researcher (LF, health policy researcher) and discussed to refine codes and interpretations. Interviews were analysed concurrently with the data collection, and alongside documentary analysis, to enable exploration of inconsistencies and to probe emerging themes in subsequent interviews. A process map was developed to describe the routine for handling a complaint as understood by those responsible for enacting it (derived from the interviews with supporting material from national regulatory and local policy documentation to guide interpretation).
Results
Triangulation of policy documentation and interview transcripts identified four critical areas of practice where the design of national rules and policies functioned to undermine a patient-centric and improvement-focused approach to complaints, relating to access, the conduct of investigations, data collection systems and performance targets. A detailed map of the organisational routine for handling a complaint as described by interviewees can be found in Online supplementary file 1.
Access: muddled routes for raising concerns
A frequently mentioned issue across staff groups was the confusing landscape of routes for raising concerns. Central to this was the lack of awareness, among both patients and frontline staff, regarding the distinct functions of formal complaints and the Patient Advice and Liaison Service (PALS), a point-of-contact within hospitals created to resolve lower-level concerns and queries directly on the ward. The visibility of PALS (one of its main attributes) positions the services as a catch-all destination for patient concerns and queries, and served to overshadow complaints departments in some cases. One of the biggest challenges that patients face in contacting us is knowing the difference between informal and formal complaints. They automatically go to PALS because it is there in the hospital, easy to see, and they think that they can help them to make a formal complaint. So, trying to distinguish the difference is something people are really struggling with and they come to us and say ‘I have been to complaints’, but they have not, they have been to PALS. (Patient advocacy worker) Honestly, everyone automatically goes: ‘PALS, if you want to make a complaint, you go to PALS’. I used to do it. I used to work in the booking office. All I knew was, ‘If you want to make a complaint, you go to PALS’. (PALS officer)
Investigation: scrutiny, corroboration and defensive tactics
Formal investigative procedures at the Trust were predominantly structured to judge the ‘well-foundedness’ of complaints, as stipulated by national regulations. The legitimacy of complaints was appraised by investigators through cross-validating raised issues with corresponding hospital documentation and staff statements, with internal evidence being regarded as superior. That is really the key for our investigations, is to make sure there has been some learning. Unless, of course, it is completely unwarranted, the complaint, in which case we will be very direct about that and say, ‘sorry, there is no root to this complaint, and it is well documented that this did not happen.’ (Complaints investigator) If the complainant's recollection is different, mainly different from what you have actually ascertained yourself, then I would say that was not upheld, because our opinion is completely different from theirs. Even though they’re stating that harm was done. (Complaints investigator)
In some cases, the ability for involved staff to shape investigations started long before the investigation. Accounts from investigators described a tendency on the frontline to pre-emptively report detailed accounts of incidents when expecting a complaint. When the staff realise, I think, on the ward, that a family could possibly put a complaint in, whether warranted or otherwise, they tend then to start to document very detailed summaries of the care. It is very unusual for you to send a complaint through, and the ward not to be expecting it. From that moment on, really, they make sure that everything is documented correctly. (Complaints investigator) I am chasing seven actions right now that have not been done, or they might be done in real-life, but they have not been closed on Datix. I have chased most of them three times. (Complaints administrator) If people did not view complaints as such a negative thing, if there was not a mindset of ‘us’ versus ‘them’ when it comes to people working with us, it would make things a lot easier. Because people just are not overly cooperative at times which can be frustrating because we it is like ‘We work for the same Trust. We are on the same team. Why?’ We are trying to take the negative and make it positive. (Complaints administrator)
National data collection systems: creating ‘false information’
Although a national data collection system (named ‘KO41a’) was introduced in response to the Mid-Staffordshire Inquiry to ‘improve the patient experience by listening to public voice’,
18
all four complaints administrators responsible for enacting coding through this scheme considered it inappropriate for use. They consistently referred to the issue that categories did not describe the problems that complaints tend to report and were further insufficiently granular for actionable learning. Two complaints administrators provided the example of a single category to reflect all issues related to clinical care. You will have a whole load of Clinical Treatment, Clinical Treatment, but you are thinking ‘it is not the Clinical Treatment’. It is not broken down correctly at all. For me, I see it as false information. It is not accurate so, therefore, how can you know how to improve? (Complaints administrator) I know that [the complaints manager] will run reports from the hospital’s informatics system and pull out the trends, so he will see how many complaints were logged, for example, under Clinical Treatment. So, yes, he will say, ‘Okay, 80 per cent of my complaints'. I do not know what he does with that information because that cannot be useful. (Complaints administrator)
Unsurprisingly, the data collection system did not adequately support the complaints manager in identifying recurring themes across complaints, who was necessitated to rely on memory rather than recorded data. Accordingly, the complaints manager noted the need for a ‘smarter’ system to record and monitor incoming complaints. To see trends, see emerging themes, perhaps things that I might not have been able to spot. I think that would be really good, because often we are relying on our feel for it, but if there was a way to flag up – ‘you’ve had five about this in the last week’ – it would be really good. (Complaints manager) I think we probably should do more following up and trying to gauge whether there are similarities across areas and whether there is deeper learning that we can take from the complainants. Because I think we probably do the learning from an individual complaint in an individual department reasonably well, but does that ripple out further? I am not sure we follow up a lot with: ‘are there similarities between these and does that reveal a bigger need?'. (Complaints investigator)
Performance targets, adverse incentives and workarounds
At managerial levels, monitoring relating to complaints was primarily focused on national performance targets for complaints handling, which in turn are mainly related to timescales for investigating and responding to complainants, and volumes of complaints received, leaving their relative severity unexplored. The Trust like numbers because it is easier to get your head around than outcome targets. This year we have had something like 50 fewer complaints than last year, so that is a good thing because it shows we are getting better. But it does not tell you that actually the complexity and severity of some of the complaints this year were beyond anything we have ever seen before. (Patient Experience Directorate) This year we have got number targets which I am in two minds about … if you've got a reduction in formal complaints, it could suggest that actually our care is getting better and people have less reason to complain. It could, however, indicate that we don't have a very open culture and we're suppressing complaints, so we could be saying we'll just pass this one on to someone else or we'll have people in the divisions discouraging people from raising concerns. (Patient Experience Directorate) So let’s say, it’s a joint complaint with different trusts, that automatically goes as medium risk because they need their time and we need our time to get our details straight. (Complaints coordinator) Medium is 45 [days to investigate], and high is 65. … It’s more about time. That’s how I’d see it, now. Obviously, if there is a very serious complaint, of course it’s going to be medium, but it’s just more about time. (Complaints administrator)
Discussion
Our study contributes to existing complaint handling research by illuminating how national policy can shape local practices and can impede an improvement-focused approach to complaints.19–22 The procedural problems identified in our findings speak to a recent complaints study in the English NHS which concluded that failures in learning are not necessarily ‘a consequence of sinister or malign organisational actors seeking to impose silence’ (p. 7)23, and, instead, can be a case of (often) well-intentioned staff confined by an overly formalised and bureaucratic system. Through a detailed examination of the enactment of this system within local practice, we have generated a number of recommendations for reform (Table 3).
Lessons and recommendations for the NHS complaints process based on this study’s findings.
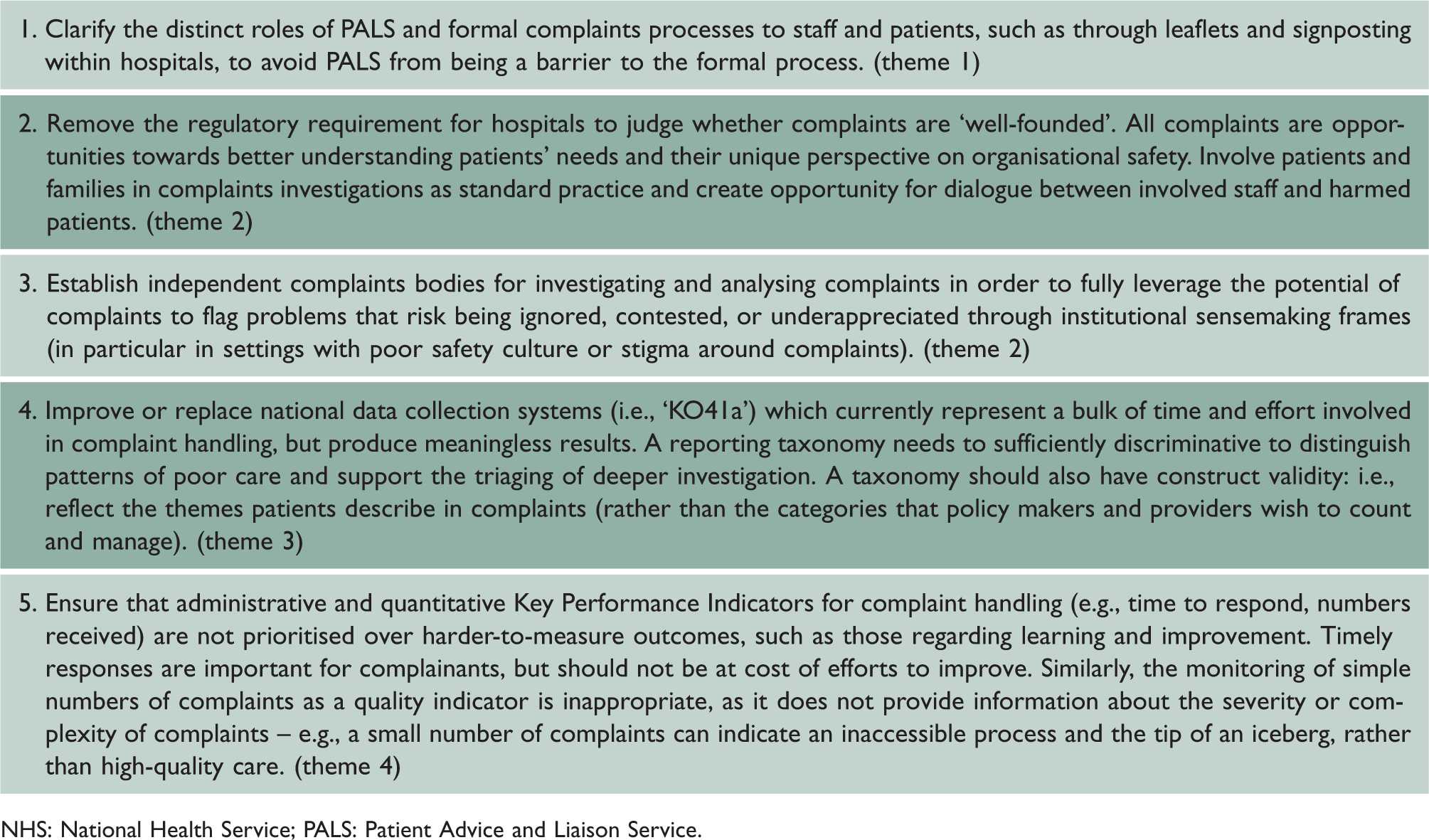
NHS: National Health Service; PALS: Patient Advice and Liaison Service.
Unlike countries with (semi-)independent complaints bodies (e.g., Finland, Sweden), English settings are required to investigate their received complaints, and report whether they are ‘well-founded’ 24 . Although, in theory, local investigations enable hospitals to action immediate improvements, our study suggests this may only occur for the small proportion of complaints that are corroborated by internal points of view, or already part of existing quality improvement workstreams, and thus reflect the already known and managed. This serves not only to uphold unequal power dynamics through assuming the superiority of clinical perspectives, but also negates the precise value of complaints as a means to uncover problems that tend to be missed, discounted or underappreciated by those within institutions. Unsafe or poor practices in healthcare often reflect issues that are normalised and thus, to some extent, blind to those enacting them. 25 Dissonant, outsider perspectives, such as those captured in complaints, are needed to highlight and challenge these practices.2,26
Further, asking hospitals to grade their own homework carries particular risks in the context of organisations with poor safety culture. The impact of a hospital’s shared norms, values and beliefs on the effectiveness of safety practices is well known in the case of incident reporting systems and safety investigations, 27, 28 and may have similar effects on a hospital’s conduct of complaints investigations – meaning complaints mechanisms may be least effective in settings where they are most needed.
Although national efforts have been made to improve learning through national data collection systems (e.g. ‘KO41a’ 18 ), this did not generate meaningful quality monitoring outputs at the investigated setting. This is in sharp contrast to the growing body of research that has developed and validated methods to reliably analyse complaints. 29 Regardless, it can be argued that narrative and dialogical approaches that enable the juxtaposition of sensemaking between patients and providers, such as patient involvement in investigations, listening clinics or public committees, may offer greater potential in understanding the needs and experiences of patients, and uncovering the implicit assumptions, beliefs and practices that make organisations unsafe.
Study strengths and limitations
Although findings resonate with earlier reviews at other English NHS settings, 8, 12 it must be noted that this study was conducted at a single multi-site NHS organisation, meaning that the findings cannot be assumed to be generalisable across settings or countries. To aid interpretation of findings relative to other settings, a detailed description of the study setting was included. A strength of the case study design was that it allowed for an in-depth exploration of enactments and adverse impacts of national policies in local practice. 30
Critically, ‘work-as-imagined’ often varies from ‘work-as-done’. 31 We aimed to gain insight on the latter by querying the activities of staff (‘what do you do?’, ‘what do you do next?’, ‘and then?’), triangulation with policy documentation, problem prompts and alternative representations. However, given that the study predominantly relied on interviews, the data represent a mix of how staff envision they are required to conduct the work and how this can play out in different ways, and we acknowledge that the study would have benefited from direct observations.
Conclusion
This study has contributed to existing evidence by demonstrating how challenges to translating complaints into quality improvement can originate from nationally defined policies and regulations for complaint handling. Recommendations for change include patient involvement in complaints investigations, the establishment of independent investigation bodies, and more meaningful data analysis strategies to uncover and address systemic causes behind recurring complaints at national and organisational levels.
Supplemental Material
sj-pdf-1-jrs-10.1177_01410768221098247 - Supplemental material for Do national policies for complaint handling in English hospitals support quality improvement? Lessons from a case study
Supplemental material, sj-pdf-1-jrs-10.1177_01410768221098247 for Do national policies for complaint handling in English hospitals support quality improvement? Lessons from a case study by J van Dael, TW Reader, AT Gillespie, L Freise, A Darzi and EK Mayer in Journal of the Royal Society of Medicine
Footnotes
Declarations
Funding
This work is supported by the National Institute for Health Research (NIHR) Imperial Patient Safety Translational Research Centre and Imperial College London. Infrastructure support was provided by the NIHR Imperial Biomedical Research Centre. The research was enabled by the iCARE environment and used the iCARE team and data resources.
Ethics approval
Not applicable (this study was conducted as part of a service evaluation).
Guarantor
EM.
Contributorship
This manuscript was written by JD with comments from AG, TR, and EM. Analysis was conducted by JD and LF. JD, AG, TR, AD and EM contributed to the conceptualisation of this study. All authors reviewed and approved the manuscript.
Acknowledgements
We thank the reviewers for their insightful comments on an earlier version of this manuscript.
Provenance
Not commissioned; peer-reviewed by Peter Ross, Bill Kirkup, Charles Vincent and Julie Morris.
Supplemental material:
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.