
Abstract
Summary
Objectives
To identify associations between success following application for consultant physician posts and demographic factors.
Design
Logistic regression analysis of nationwide survey data.
Setting
United Kingdom (UK) physicians with a recent certificate of completion of training (CCT).
Participants
All UK trainee physicians who received a CCT between 2010 and 2019 were surveyed. Respondents were excluded if they had not applied for a consultant post or if application data were incomplete.
Main outcome measures
The primary outcome measure was success over the entire consultant application process, i.e. shortlisted and offered the post following the first application. Secondary outcomes were: shortlisted following first application and offered a consultant post at first interview.
Results
From 7037 CCT holders surveyed, 50.7% responded. While 1198 (59.7%) respondents were white, 760 (37.9%) were from minority ethnic groups and 50 (3.5%) were of unknown ethnicity. Primary medical qualification (PMQ) country was the UK in 75.3% (n = 1512). On multivariable logistic regression analysis the independent negative associations with success were: minority ethnicity (odds ratio [OR] 0.55, 95% confidence interval [CI] 0.43–0.71); p < 0.001) vs. white; PMQ from Europe (OR 0.47, 95% CI 0.28–0.79; p = 0.004) or Asia (OR 0.68, 95% CI 0.49–0.96; p = 0.027) vs. UK PMQ; year of CCT 2012 (OR 0.40, 95% CI 0.24–0.68; p = 0.001), 2013 (OR 0.39, 95% CI 0.23–0.65; p < 0.001), and 2014 (OR 0.26, 95% CI 0.15–0.43; p < 0.001) vs. 2019. Specialties associated with lower success rates included Cardiology, Endocrinology, Genitourinary medicine, Palliative care, Renal and Respiratory, compared to Acute medicine.
Conclusions
Minority ethnic group candidates for consultant physician posts had lower success rates compared to white candidates after correction for important variables including specialty, time from and country of PMQ. This finding requires further evaluation to identify the causes for this variation.
Background
The United Kingdom (UK) National Health Service (NHS) employs a higher proportion of staff from minority ethnic groups compared to the general UK population. 1 Similarly, the proportion of doctors from minority ethnic groups (37.8%) in the UK is higher than the proportion of minority ethnicity people in the UK (13.7%).2,3
Despite the large number of minority ethnicity doctors in the UK, there is evidence of unequal attainment among different ethnicities in both undergraduate and postgraduate assessments. White students achieve better results than minority ethnicity students in both undergraduate and postgraduate assessments. 4 This includes the practical component of the postgraduate MRCP examination. 5 However, ethnicity doctors also do less well in multiple choice postgraduate examinations for General Practice and Physician trainees, both of which are computer marked, which should eliminate any suggestion of examiner bias.4,6,7 This pattern extends beyond the setting of undergraduate and postgraduate examinations, as minority ethnicity doctors are also less successful in research funding applications and are more likely to receive unsatisfactory Annual Review of Competence Progression training outcomes.8,9
Senior physicians in the USA from minority ethnic backgrounds report experiencing higher rates of discrimination than their white counterparts. This is reportedly from both their faculty colleagues and patients.10,11 minority ethnicity consultant physicians in the UK also report higher rates of discriminatory behaviour or language than white consultants. 12 There is also variable remuneration by both race and gender in the NHS. 13 The proportion of minority ethnicity doctors is higher within specialties in which posts have historically been harder to fill, such as care of the elderly and paediatrics. 14 NHS minority staff are also more likely than their white counterparts to report low job satisfaction and a sense of not being valued by their employing organisation. 15
The aim of this analysis was to establish whether ethnicity was associated with success during the consultant physician application process.
Methods
Overview of physician training and application to consultant posts
Physician training in the UK comprises three stages. Immediately following completion of their primary medical qualification (PMQ), doctors complete a two-year foundation programme. Doctors wishing to train as physicians must complete internal medicine training (three years) followed by higher specialist training in their chosen specialty (generally over four years). A certificate of completion of training (CCT) is then awarded. Physician training is overseen by the Joint Royal Colleges of Physicians Training Board (JRCPTB).
Trainees may apply for a consultant physician post six months prior to the expected date of award of a CCT. Following an application, trainees may be shortlisted and invited for competitive interview. Trainees can apply for more than one consultant post at a time. Consultants in the UK are senior decision makers who lead a team of typically trainee doctors to manage their patients. All patients in the UK NHS have a named consultant, who is ultimately responsible for their treatment.
Participants
The JRCPTB provides the Royal College of Physicians (RCP) Medical Workforce Unit (MWU) annually with the contact details for trainees in all medical specialties who have gained their CCT in the previous 12 months. The MWU undertakes an annual survey of all trainees obtaining a CCT in the previous 12 months. In the survey, CCT holders are asked if they have applied for a substantive consultant post since their CCT was awarded. If they had applied for a consultant post, they were then asked how many consultant posts they had: applied for; been shortlisted for interview for; and been offered at interview.
The MWU created the dataset for this analysis, including all respondents from the annual surveys. The dataset was anonymised before being provided to the researchers.
Exclusion criteria
Respondents were not included if they had not yet applied for a consultant post or if data pertaining to their consultant applications were incomplete when supplied.
Unfortunately, data were not available for 2016 due to an error in the survey software that year that erroneously excluded CCT holders who already held a consultant post at the time of the survey.
Data collection
Between 2011 and 2019, Verint questionnaire software was used to distribute the survey to all doctors who had obtained their CCT in the previous 12 months, from 1 January 2010 to 31 December 2018. Data specifying if a respondent applied for a post outside of their deanery were available from 2014 onwards.
Data collected included demographics (gender, ethnicity and age), primary specialty, UK geographical region of training, date of PMQ and country of PMQ, and if a respondent had worked less than full time (LTFT) at any point while training. Based on CCT holders’ responses, ethnicity was based upon the standard Office for National Statistics categories: white – English/Welsh/Scottish/Northern Irish/British, Irish, Gypsy or Irish Traveller, any other white background; mixed – white and black Caribbean, white and black African, white and Asian, any other mixed/multiple ethnic background; Asian – Indian, Pakistani, Bangladeshi, Chinese, any other Asian background; black – African, Caribbean, any other black/African/Caribbean background; Middle Eastern – Arab, other Middle Eastern; and any other ethnic group.
Missing demographic data from the surveys were obtained from RCP annual census data where possible. The date and country of PMQ and CCT date were obtained from the General Medical Council.
Outcome variables
The primary outcome variable was self-reported success rate over the entire consultant application process, i.e. shortlisted and offered the post following interview for the first application (or if more than one application made in parallel, success following all applications made). This primary outcome is hereafter referred to as the ‘entire application process’.
Secondary outcomes were twofold: shortlisted following first application (or if more than one application made in parallel, shortlisted following all applications); and offered a consultant post following first interview (or if more than one interview for applications made in parallel, offered following all interviews).
The interview outcome analyses were performed for all respondents who had been shortlisted following any application.
Receiving any offer of a consultant post following all applications (whether in parallel or in series) was not included as an outcome variable because nearly all candidates were eventually successful in obtaining a consultant post and thus there was limited variability in this outcome.
Statistical analysis
A chi-square test was used to assess statistical associations between categorical predictor variables and the outcome measures.
Multivariable logistic regression models looking at the effect of ethnicity on each outcome measure controlling for potential confounders were then constructed. Numbers for some specific ethnicities among doctors from minority ethnic groups were small, and minority ethnicity respondents were therefore grouped together for the multivariable analyses. Goodness of fit was confirmed with the Hosmer-Lemeshow test. p values of <0.05 were considered statistically significant. Statistical analysis was performed using Stata version 15. 16
Results
Participants and missing data
Of 7037 CCT holders who had completed their training between 1 January 2010 and 31 December 2018, 3571 (50.7%) responded, with annual response rates between 47.2% and 52.0%.
A total of 2008 responses were available with complete data for the analysis. A flow chart for the study is shown in Supplementary Figure 1. Respondents were excluded if they had not yet applied for a consultant post (n = 1032) or if data on the number of applications, shortlisting or offered consultant posts were incomplete (n = 417). The demographic characteristics of included CCT holders compared with those excluded due to incomplete data on applications, shortlisting or offered consultant posts are shown in Supplementary Table 1.
The analysis of interview outcomes included the 1975 respondents shortlisted following any application. Data on LTFT training were not available for 5.8% of respondents. No other variables had significant quantities of missing data (>2.5%).
Respondent demographics
Descriptive statistics for all variables in the study.

CCT: certificate of completion of training; PMQ: primary medical qualification.
‘Other’ specialty group comprises specialties with fewer than 40 responses, including: Allergy, Audio-vestibular medicine, Genetics, Neurophysiology, Clinical pharmacology, Immunology, Infectious disease, Intensive care medicine, Medical ophthalmology, Medical oncology, Nuclear medicine, Paediatric cardiology, Pharmaceutical medicine, Rehabilitation medicine, Sport and exercise medicine, and Stroke medicine.
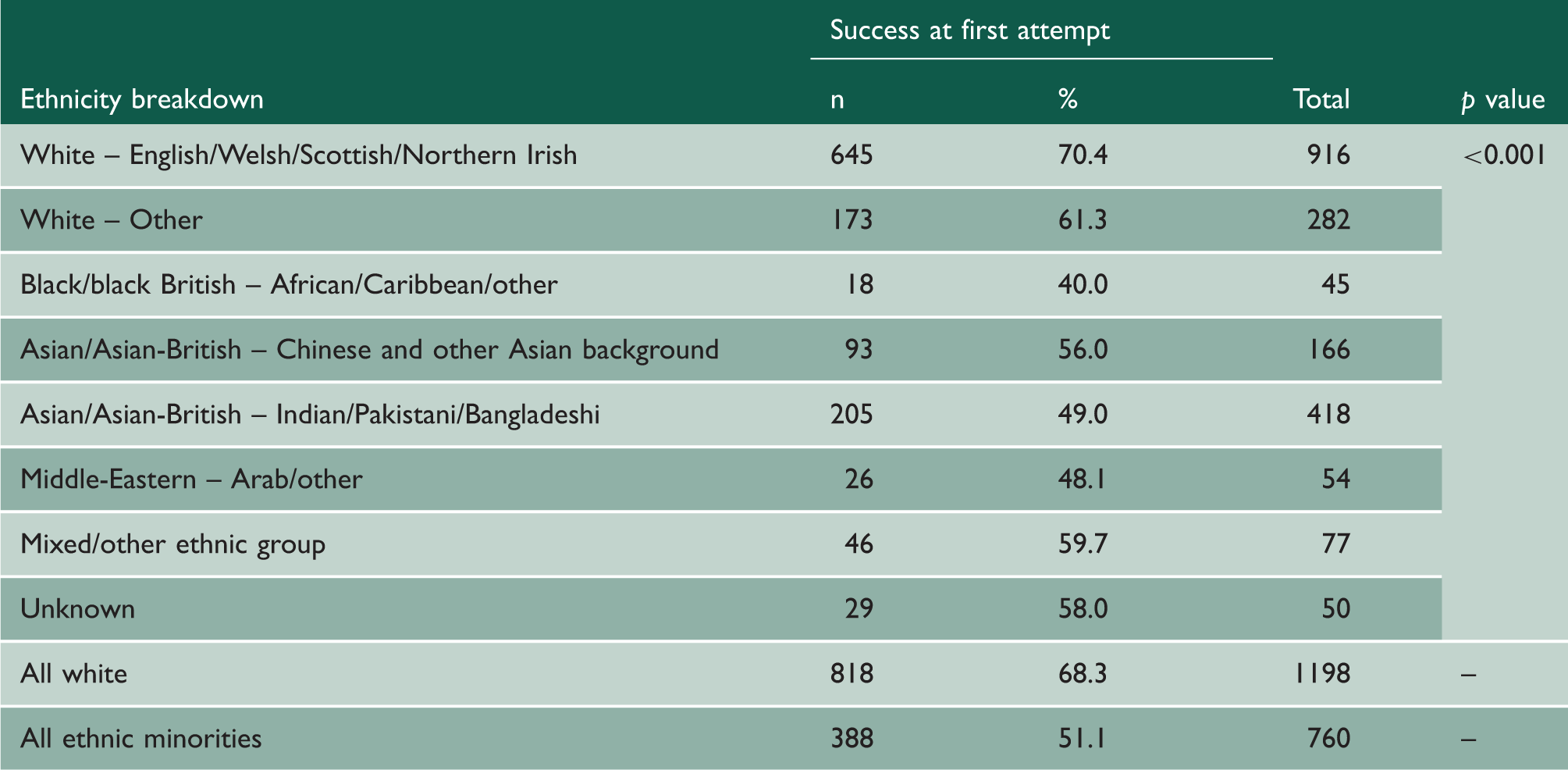
Ethnicity is provided as the broad groups used in analyses. Detailed ethnicity data for respondents can be found in Table 3.
The majority of respondents were from a white (English, Welsh, Scottish or Northern Irish) (n = 916; 45.6%) or white (other) (n = 282; 14.0%) ethnic background; 418 (20.8%) were Asian (Pakistan, India and Bangladesh), 166 (8.3%) were East Asian (including Chinese and other Asian backgrounds), 45 (2.2%) were black, 54 (2.7%) Middle Eastern, 77 (3.8%) mixed or other ethnic groups, and 50 (2.5%) were of unknown ethnicity.
Success rates over the entire consultant application process by ethnicity with number of successful applications at first attempt and success rate in each ethnic group.
Among white respondents, 53.2% were female, compared with 32.6% of minority ethnicity respondents (p < 0.001). LTFT training was more prevalent among white than minority ethnicity respondents (18.8% vs. 9.6%, p < 0.001) and such trainees were almost all female (95.2%). The proportions of white and minority ethnicity respondents varied significantly by specialty. These are shown in Supplementary Table 2.
Application, shortlisting and interview success
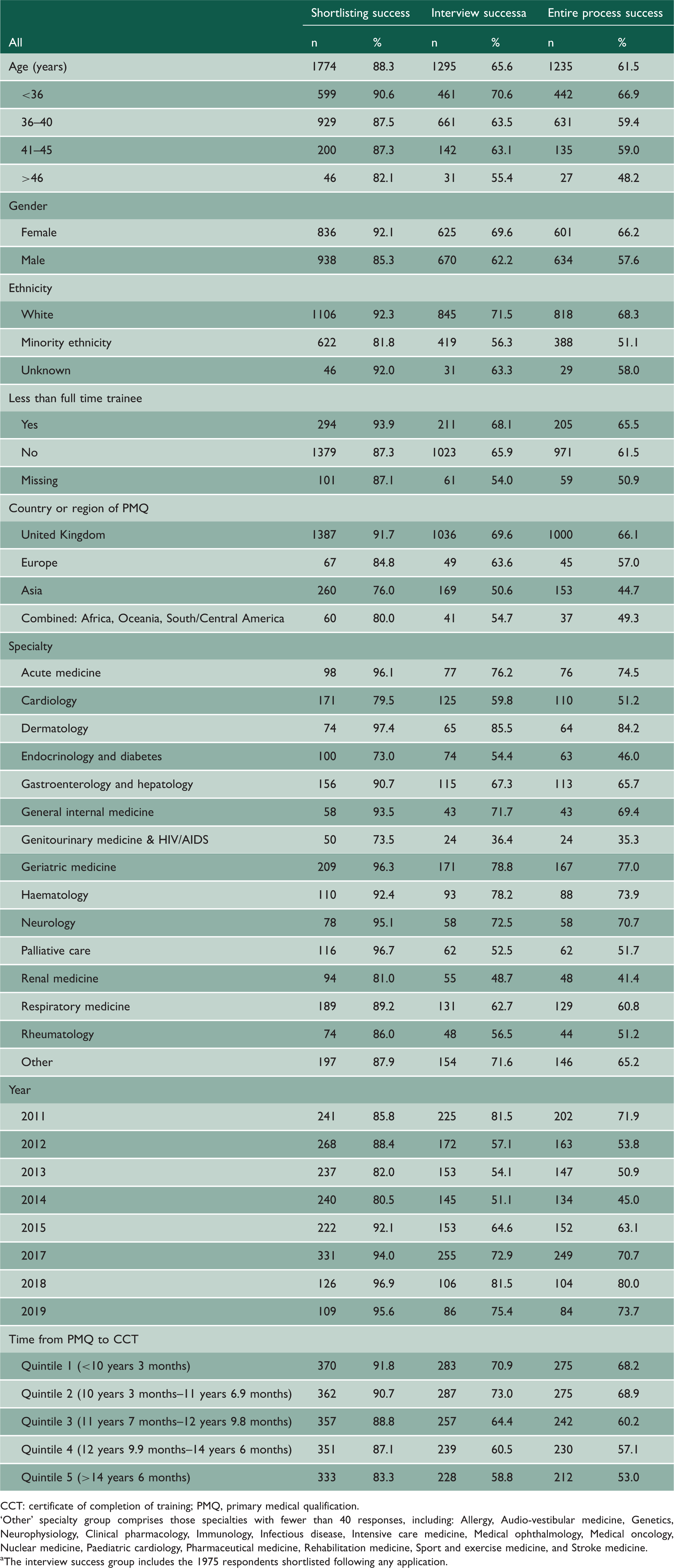
Respondents reported applying for one (n = 1201; 59.8%), two (n = 414; 20.6%), three (n = 216; 10.8%) or more than three (n = 177; 8.8%) consultant posts, with 38.5% applying outside their UK training region. Of the CCT holders who had applied for a consultant post, 98.4% were shortlisted for at least one post and 88.3% were shortlisted following their first application.
Over the entire application process, 61.5% of respondents were successful following their first attempt. Among those shortlisted, 65.6% were successful in being offered a consultant post following their first or all interview attempts, regardless of the number of applications and 90.2% were eventually successful in being offered a consultant post after any number of interviews (median interviews 1 [range 1–14]).
Univariable analyses
First time success rate during the consultant application process for shortlisting, interview success and over the entire application process.
CCT: certificate of completion of training; PMQ, primary medical qualification.
‘Other’ specialty group comprises those specialties with fewer than 40 responses, including: Allergy, Audio-vestibular medicine, Genetics, Neurophysiology, Clinical pharmacology, Immunology, Infectious disease, Intensive care medicine, Medical ophthalmology, Medical oncology, Nuclear medicine, Paediatric cardiology, Pharmaceutical medicine, Rehabilitation medicine, Sport and exercise medicine, and Stroke medicine.
aThe interview success group includes the 1975 respondents shortlisted following any application.
Ethnic differences in applications, shortlisting and consultant post offers
White CCT holders applied for a median of 1 (interquartile range [IQR] 1–2) consultant posts and minority ethnicity CCT holders for a median of 2 (IQR 1–3) posts (p < 0.001). Compared with 46.6% of minority ethnicity CCT holders (p < 0.001), 33.9% of white CCT holders applied for posts outside their deanery.
Respondents from minority ethnicity backgrounds were less likely than white respondents to be shortlisted following their first application (81.8% vs. 92.3%; p < 0.001), less likely to be successful at interview having been shortlisted (56.3% vs. 71.5%; p < 0.001) and less likely to be successful over the entire application process for their first application (51.1% vs. 68.3%; p < 0.001). Black applicants had the lowest success rate for the entire application process for their first application (40%), which was markedly lower than the minority ethnic group overall (51.1%) (Table 3).
Country of primary medical qualification
Asian graduates were least likely to be successful over the entire application process for their first application (44.7%), followed by graduates from Africa, Oceania and America (49.3%) and Europe (57.0%), with UK graduates the most likely successful (66.1%) (p < 0.001).
Time from PMQ to CCT
A longer time from PMQ (median 12.2 years, IQR 3.3 years) to CCT was associated with lower success rates after first application (when comparing those requiring less than 10.3 years with those needing more than 14.5 years) over the entire application process (68.2% vs. 53.0% respectively; p < 0.001), as well as at shortlisting (91.8% vs. 83.3% respectively; p = 0.002) and at interview (70.9% vs. 58.8% respectively; p < 0.001).
Gender
Male respondents were less likely to be successful following their first application than female respondents across the entire application process (57.6% vs. 66.2%; p < 0.001), at shortlisting (85.3% vs. 92.1%; p < 0.001), and at interview (62.2% vs. 69.6%; p < 0.001).
Less than full time training
Full time training was associated with lower success over the entire application process compared to LTFT (61.5% vs. 65.5%; p = 0.022), at shortlisting (87.3% vs. 93.9%; p = 0.004) and at interview (65.9% vs. 68.1%; p = 0.022).
Year of CCT
Success at first attempt for the entire application process varied between survey years; however, in general, success rates have improved in more recent years (71.9% in 2011, 53.8% in 2012, 80.0% in 2018, 73.7% in 2019).
Region
The UK region in which CCT holders applied for a consultant post was not included in this analysis. A subgroup analysis including a univariable logistic regression model was constructed for the primary outcome measure, using London as the reference category. Only Scotland (OR 1.63, 95% CI 1.09–2.44; p = 0.017) had significantly better success rates (Supplementary Tables 3 and 4).
Multivariable analysis
Multivariable logistic regression analysis of first time success rates over the entire consultant application process.

CCT: certificate of completion of training; PMQ: primary medical qualification.
‘Other’ specialty group comprises those specialties with fewer than 40 responses, including: Allergy, Audio-vestibular medicine, Genetics, Neurophysiology, Clinical pharmacology, Immunology, Infectious disease, Intensive care medicine, Medical ophthalmology, Medical oncology, Nuclear medicine, Paediatric cardiology, Pharmaceutical medicine, Rehabilitation medicine, Sport and exercise medicine, and Stroke medicine.
Multivariable logistic regression analysis of first time success rates for shortlisting and at interview during the consultant application process.
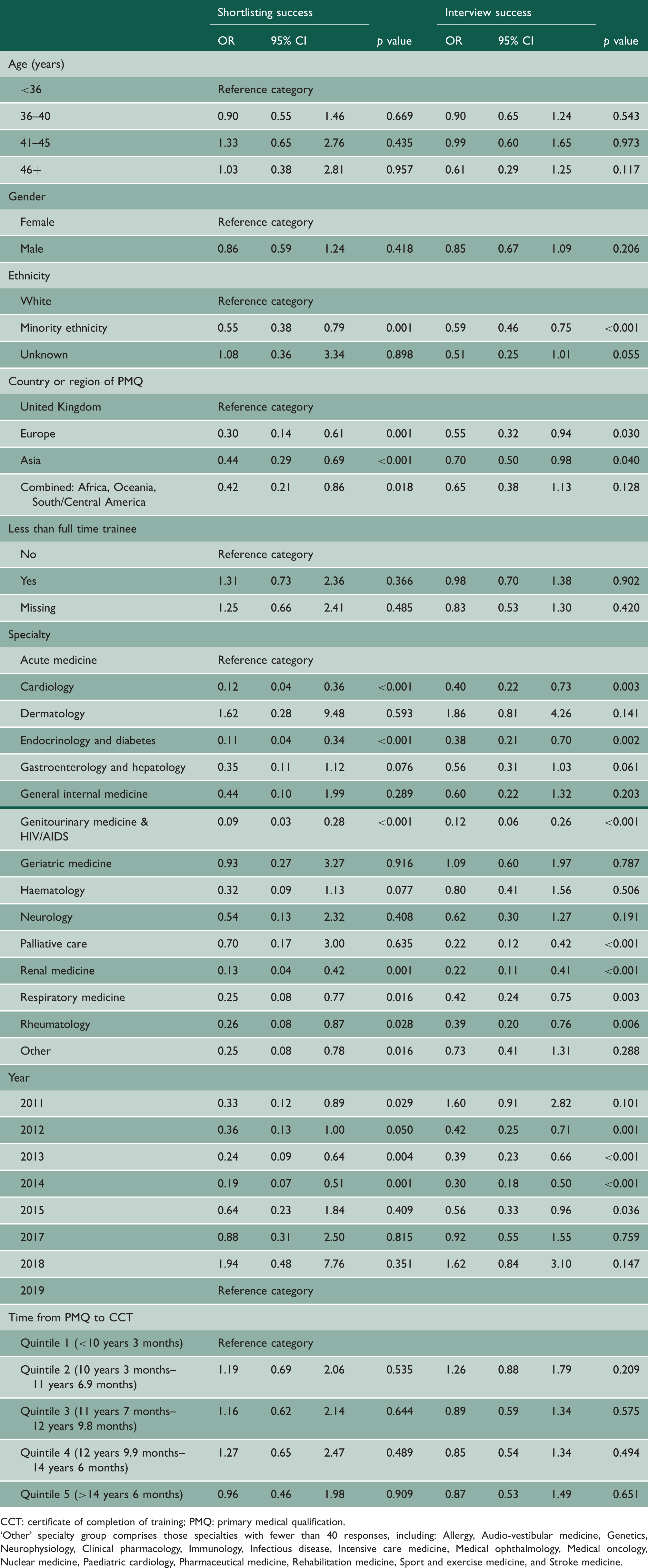
CCT: certificate of completion of training; PMQ: primary medical qualification.
‘Other’ specialty group comprises those specialties with fewer than 40 responses, including: Allergy, Audio-vestibular medicine, Genetics, Neurophysiology, Clinical pharmacology, Immunology, Infectious disease, Intensive care medicine, Medical ophthalmology, Medical oncology, Nuclear medicine, Paediatric cardiology, Pharmaceutical medicine, Rehabilitation medicine, Sport and exercise medicine, and Stroke medicine.
Discussion
This study demonstrates a strong association between successful applications for consultant physician posts and ethnicity. White applicants had higher success rates compared to their minority ethnicity counterparts. Black CCT holders had the lowest success rate of all ethnic groups. The negative association between minority ethnicity CCT holders and success on first application was observed despite adjusting the analysis for other important factors including: country of PMQ; other demographics factors; LTFT training status; specialty; and CCT year. This relationship was consistently seen in both the face-to-face setting of consultant interviews and at the paper-based shortlisting stage.
These findings are in keeping with results of previous research. Differential levels of attainment between ethnic groups have been documented in both UK medical undergraduates and in the postgraduate medical workforce. However, to observe in a multivariable analysis adjusted for many potentially important confounding factors, that minority ethnicity CCT holders are 17% less likely to be successful at first application for a consultant job compared to white candidates is highly significant. There may be conscious or unconscious selection bias in favour of white CCT holders during the consultant application process. Unfortunately, detailed information regarding the strength of applications is not available. It is therefore not possible to exclude the possibility that white applicants were better qualified. Considering the differential levels of attainment previously reported, it is also possible that some minority ethnicity candidates are less competitive applicants due to their previous experiences of bias leading to reduced opportunities earlier in their careers. 17
The analysis is reassuring with respect to CCT holders who had trained LTFT and female trainees. Both groups were equally, if not more successful, compared to full-time and male trainees. In multivariable models there was no association with success in the consultant application process based on these characteristics.
The year of CCT was a significant factor in application success. Both shortlisting and interview success rates were generally higher in more recent years. This is likely to be the result of the increasing number of consultant posts being advertised in medical specialties in the UK. Applying for consultant posts has become less competitive and the ability to appoint to advertised posts has fallen. 12 However, despite more consultant posts and difficulties filling them, lower success rates for minority ethnicity CCT holders persist.
This is in contrast to the time taken from PMQ to CCT. Although this was associated with application success on univariable analysis, no association was seen in the multivariable models. There are a number of different explanations for trainees requiring longer to achieve their CCT. These include additional experience that makes them more likely to be successful such as a research or an experiential fellowship, some neutral factors such as time out of training before starting specialist training, and some factors that may make CCT holders less likely to be successful, such as failure at annual assessments.
The overall survey response rate was 50.7% and therefore the present study includes a substantial proportion of CCT holders surveyed. A comparison of CCT holders included and those excluded due to incomplete consultant application data suggests that there are some differences between these groups, notably by ethnicity, age and country of PMQ (Supplementary Table 1). The likelihood of responding to the survey was also potentially lower if CCT holders felt that the application process or any other aspect of training had not treated them equitably. It is a limitation that data regarding non-responders’ success on consultant application are not available to us. However, this seems unlikely to be a major source of bias given the large number of CCT holders who were successful on first or subsequent application but this cannot be excluded. Furthermore, if this issue was reducing the response rate significantly, it would likely lead to the opposite pattern of results to that which was observed.
It was not possible to correct for CCT holders seeking posts in more competitive hospitals, compared to those that are less competitive. This might therefore reduce the success rates for those CCT holders. All UK training regions include both competitive and less competitive hospitals for consultant posts and controlling for region would therefore not account for this potential source of bias and this was confirmed in a sub-analysis of success rates by region. Medical speciality was included in the logistic regression models and therefore it is likely that a significant component of variation in competition between posts will be accounted for through this. A further limitation was that when applicants had applied for multiple consultant posts, but were not offered a consultant post each time, it was assumed for the analysis that they had not been successful at their first attempt. However, this may, in a small group of CCT holders, represent a CCT holder applying for a second job unsuccessfully, after already having been appointed successfully at their first attempt. Such respondents were not considered to be successful at their first attempt in this analysis.
Conclusions
This dataset is unique, in both the number of respondents and nationwide coverage. Although the results are striking, they are not unexpected given other data suggesting differential attainment by ethnicity at other stages of medical training. All applicants had successfully completed a higher specialty training programme in the UK. Our findings suggest that there may be conscious or unconscious selection bias in favour of white candidates. This bias may be a component of the application process but may also be a result of cumulative experience of bias at prior career stages. These findings require urgent evaluation of the consultant application process to ensure fair treatment of all applicants for consultant posts.
Supplemental Material
sj-pdf-1-jrs-10.1177_01410768221085691 - Supplemental material for Ethnic differences in success at application for consultant posts among United Kingdom physicians from 2011 to 2019: a retrospective cross-sectional observational study
Supplemental material, sj-pdf-1-jrs-10.1177_01410768221085691 for Ethnic differences in success at application for consultant posts among United Kingdom physicians from 2011 to 2019: a retrospective cross-sectional observational study by PR Harvey, C Phillips, N Newbery, D Nagamoottoo, K Woolf and NJ Trudgill in Journal of the Royal Society of Medicine
Supplemental Material
sj-pdf-2-jrs-10.1177_01410768221085691 - Supplemental material for Ethnic differences in success at application for consultant posts among United Kingdom physicians from 2011 to 2019: a retrospective cross-sectional observational study
Supplemental material, sj-pdf-2-jrs-10.1177_01410768221085691 for Ethnic differences in success at application for consultant posts among United Kingdom physicians from 2011 to 2019: a retrospective cross-sectional observational study by PR Harvey, C Phillips, N Newbery, D Nagamoottoo, K Woolf and NJ Trudgill in Journal of the Royal Society of Medicine
Footnotes
Declarations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.