
Abstract

Reports and recommendations concerning professional development of doctors and other healthcare practitioners often use the term ‘role model’ imprecisely. Given that role models are considered important in shaping careers, 1 this is surprising.
The Oxford English Dictionary (www.oed.com) defines a role model as ‘a person regarded by others as an example to be imitated’. Role models may be from any walk of life and inspire others by their personality, individuality and actions, through face-to-face relationships or at a distance. Rather like ‘beauty is in the eye of the beholder’, role models are defined by the onlooker, so we do not choose whether or not to be one. Also, unlike for formal educational or mentoring responsibilities, one cannot train specifically to be a role model.
This essay aims to clarify the concepts, nature and effects of role models. It explores role models, with reference to a ‘witness seminar’ about United Kingdom National Health Service psychiatric hospitals in the 1960s. 2 A witness seminar is an established method of oral history whereby people associated with a set of events meet to discuss their involvement and experience. The meeting is recorded, and the transcript becomes a unique primary source for historical research. Our ‘witnesses’ included doctors, nurses, a social worker, a psychologist, an occupational therapist and a patient (see supplementary Appendix). The ‘audience’ included psy-professionals at all stages of their careers. They posed questions, commented and stimulated discussion. One theme which emerged was the impact of good and bad role models on people’s careers. Although the witnesses were recalling events from very early in their professional lives, over 50 years ago, they identified profound and often life-long influences that individuals had on them, on their values and perspectives, their careers and their clinical practice. We draw on the witness seminar to highlight the effects of some senior staff, mainly psychiatrists, on the careers of their junior colleagues. Placed in the context of recent literature on role models and the medical profession, our witnesses’ accounts provoked thought on: medical training and careers; positive and negative role models; and how, as doctors, we might unwittingly influence others.
The historical material
Witness seminar participants recalled influential role models from the 1960s with whom they had professional workplace encounters or observed from afar. Several mentioned William Sargant (1907–1988), a London-based consultant psychiatrist. Sargant’s approach to patients and colleagues, and his almost exclusively biological methods of treatment, were controversial. 3 Peter Tyrer, a trainee psychiatrist at the time, recalled Sargant’s manner, including that he would shout down abusively anyone who challenged him. Tyrer worried that he was complicit in Sargant’s unconventional treatments by failing to confront him, even though that would almost inevitably have failed. He also attributed to Sargant his early interest in randomised controlled trials, but ‘learnt more from him by what he did to excess than from others who taught me more correctly’.
Witnesses also discussed RD Laing (1927–1989), an exponent of ‘anti-psychiatry’ who refuted biological causes and treatments of mental illness and emphasised psychosocial aetiologies and treatments. John Bradley recalled Laing drinking almost a bottle of whisky during a lecture, not a role model to follow, but Tom Burns referred to Laing’s inspirational writing impacting on Cambridge medical students: ‘I think he brought lots of people into psychiatry.’ David Jolley recalled another psychiatrist, Russell Barton (1926–2002). He was vociferous in the 1960s about providing humane and dignified care for mentally ill people in psychiatric hospitals, but his adversarial style when advocating for his patients was controversial (some said foolhardy 4 ). Other witness seminar participants recalled strong career-formative emotions associated with interactions with senior people as role models. Two nurses recalled harsh attitudes and styles of nursing leaders, which they were determined never to emulate, and a psychologist was ‘very well supported [after a patient’s suicide], an act of real compassion and concern by a very experienced psychiatrist to a very young and green clinical psychologist. It’s one of those events I’ll never forget.’
Sargant, Laing and Barton were all radical, charismatic and visionary personalities. All three stood on the fringes of conventional psychiatry. Their habits, intransigence and styles of communication were as contentious as their clinical methods. Despite their intellectual inspiration, their styles of behaviour as role models influenced onlookers, some of whom sought to avoid imitating them.
As with all historical sources, context changes with time so interpreting and learning from the past requires caution. Changing circumstances, such as flatter institutional hierarchies and different methods of evaluating clinical and scientific ‘evidence’, mean that role models today may be different from those in the past. However, the 1960s’ role models’ personal qualities, as described by the witnesses, resonated across our multi-generational audience. The overall impression given by the witnesses was that those who encountered good role models wished to emulate them, and those who encountered bad, sought never to do so. Role models, whether known personally or observed at a distance, influenced people’s careers long term.
Role models today
Qualities associated with positive role models.
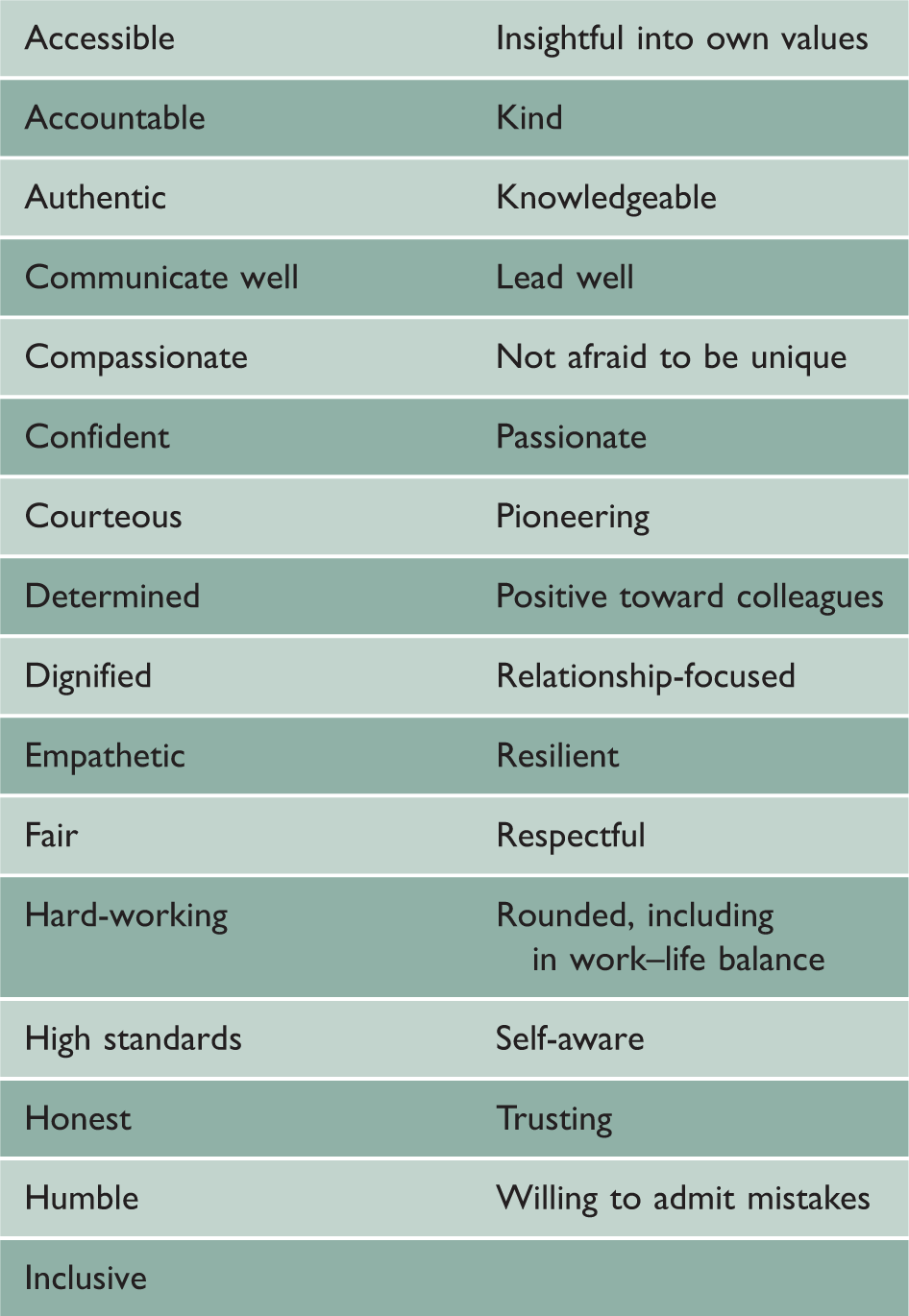
Exceptional achievements, such as excellence in research and publications, senior management positions, power, status, public accolades and high earnings were relatively low on lists of attributes ascribed to role models. 5 Although these may be desirable ends in themselves, they do not imply that the achiever had personal qualities which one would seek to emulate across the course of a career.
The General Medical Council instructs doctors to act ‘as a positive role model in their behaviour towards patients, colleagues and others’. 11 The General Medical Council and other healthcare education bodies emphasise the importance of role models in professional development and in making career choices. 12 Nevertheless, some people report that they could not identify role models who had influenced their careers, but found personal contact and dialogue with officially appointed mentors, supervisors and research collaborators more useful. 9
Encounters with negative role models may distress medical students and doctors. 5 However, negative role models may be useful insofar as they clarify how not to practise, and may incentivise the onlooker to work differently. One single person may convey both negative and positive role model qualities, 13 and a dedicated and model clinician can be transformed into a less than ideal role model if working in an excessively pressurised, under-valued or under-funded discipline. Dinesh Bhugra (past-president, World Psychiatric Association) cautions us: ‘If our trainees see us as tired, fed up and demoralised, they are likely to question not only our commitment but also their own professional attributes’. 14 This may be detrimental to the onlooker’s professional development and to recruitment into a discipline. We all like to think we would constructively challenge unacceptable behaviour. However, as Tyrer reminded us when talking about Sargant, personality and rank may make that a fearful proposition, with the complainant foreseeing possible adverse consequences, such as receiving a poor reference or being ostracised as a whistleblower. 15
Variability in senior staff’s personal attributes, and how they are perceived, raises debate about whether role models can reliably impart professional values, attitudes and behaviours. Some medical educationalists advise that professional attributes should be taught through peer group discussion, access to trained mentors and exposure to the views of people outside medicine. 5 Others disagree: ‘I don’t think you can teach those attributes any more than the army can teach people courage. I admire those who possess that most important aspect of being a role model – to teach the things that can’t be taught’ (said Sir Simon Wessely,16 past-president, Royal College of Psychiatrists, and Royal Society of Medicine).
The witness seminar pointed to long-term legacies of medical role models, particularly of senior staff who shaped personal qualities of being and doing in up-and-coming colleagues, in contrast to the often more fleeting effects of the scientific-clinical contexts in which they worked.
Today, the emergence and pervasion of online social media, such as Twitter, allows clinicians to connect with a wider-than-ever pool of potential role models. The growing popularity of connecting with others online (e.g. through #MedTwitter and #PsychTwitter as well as user-compiled clinician account ‘lists’) speaks to our enduring curiosity to seek out role models. The GMC offers guidance to doctors about using social media, emphasising that it requires the same standards of professionalism as face-to-face encounters, and that ‘new challenges can arise’. 17 The British Medical Association acknowledges benefits of social media, but also its risks, such as trolling, harassment and compromising privacy. 18 Social media ‘followers’ need to be discerning about the nuances of behaviour of potential online role model ‘influencers’, and insightful into the context and purpose of the ‘posts’ viewed. Recent research about social media use by the medical profession has tended to consider role models as secondary to other main themes, 19 so further specific research would be timely. Perhaps ‘Thinks before sharing’ might be appropriate to add to the list of qualities associated with positive role models. 18
Both good and bad may shape our careers and we need, more than ever, to reflect on how and why this occurs, and to what ends. Pioneer of evidence-based medicine, Dave Sackett, was quoted as saying: ‘Half of what you'll learn in medical school will be shown to be either dead wrong or out of date within five years of your graduation’, 20 further emphasising the importance of developing personal qualities and professional attributes. As the variously attributed and timeless quote sums up: ‘people may forget what you said – but they will never forget how you made them feel’.
Supplemental Material
sj-pdf-1-jrs-10.1177_01410768221080776 - Supplemental material for The best and worst of role models across the generations
Supplemental material, sj-pdf-1-jrs-10.1177_01410768221080776 for The best and worst of role models across the generations by Claire Hilton and Thomas Stephenson in Journal of the Royal Society of Medicine
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.