
Abstract
Objective
To investigate the relative impact of generic entry and National Institute for Health and Care Excellence clinical guidelines on prescribing using statins as an exemplar.
Design
Retrospective analysis of statin prescribing in primary care and cost simulation model.
Setting
Royal College of General Practitioners Research and Surveillance Centre (RCGP R&SC) database and Prescription Cost Analysis (PCA) database.
Participants
New patients prescribed statins for the first time between July 2003 and September 2018.
Main outcome measures
Shares of new patients prescribed one of the five statins available in the British National Formulary, and cost of prescribing statins to new and existing patients in primary care in England.
Results
General trends of statin’ prescriptions were largely driven by a decrease in acquisition costs triggered by patent expiration, preceding NICE guidelines which themselves did not seem to affect prescription trends. Significant heterogeneity is observed in the prescription of the most cost-effective statin acrossGPs. A cost simulation shows that, between 2004 and 2018, the NHS could have saved £2.8bn (around 40% of the £6.3bn spent on statins during this time) if all GP practices had prescribed only the most cost-effective treatment.
Conclusions
There is potential for large savings for the NHS if new and, whenever possible, ongoing patients are promptly switched to the first medicine that becomes available as generic within a therapeutic class as long as it has similar efficacy to still-patented medicines.
Introduction
In a context where national health systems of all high- and medium-income countries are confronted by ballooning costs of caring for an ageing population and an increase in prevalence of long-term conditions, promoting cost-effective prescribing represents an important part of controlling healthcare expenditure.1,2 In the English National Health Service (NHS), the National Institute for Health and Care Excellence (NICE) publishes national guidance aimed at promoting clinical and cost-effective evidence-based recommendations for the clinical management of different conditions. In therapeutic markets where treatments have similar safety and effectiveness, NICE recommendations may vary over time following changes in acquisition costs, e.g. due to patent expirations and the ensuing entry of generics. However, persistence of prescribing habits and prescribers’ lack of awareness of medicines’ actual cost may mean that the uptake of NICE recommended medicines can vary substantially across general practitioners and practices, despite efforts at local level, including Clinical Commissioning Groups (CCG), to encourage more cost-effective prescribing.3–7 Since low responsiveness to adopt NICE recommendations can substantially undermine NHS efforts to contain drug expenditure, it is important to understand the pervasiveness of such behaviour.
Statins represent an ideal market to investigate the relative importance of prices and clinical guidelines in explaining prescribing behaviour for at least two reasons. First, statins are the most widely used treatment for primary and secondary prevention of cardiovascular disease, conditions with an estimated cost to the NHS of roughly £7.4 billion a year.8,9 Second, there are five main events that have shaped the statins market over the last two decades. In May 2003, simvastatin (brand name Zocor) lost patent protection and became available as a generic drug. In January 2006, NICE published Technological Appraisal 94 (TA-94), stating that all statins were equally effective from a therapeutic point of view, advising general practitioners to consider costs of statins when choosing the initial treatment and advising that simvastatin was the cheapest. 10 Clinical Guideline 67 (CG-67), released in May 2008, stated that treatment initiation should start with simvastatin. 11 In May 2012, atorvastatin (brand name Lipitor) lost patent protection and became available generically. Finally, two years later, in May 2014, NICE published Clinical Guidelines 181 (CG-181) recommending atorvastatin as initial treatment. 12 The reduced cost after patent expiration coupled with its relatively greater potency made atorvastatin the most cost-effective statin in the market.
Using statins as an exemplar, this study investigated the prescription dynamics in a large sample of the English primary care sector between 2004 and 2018. First, we explored the relationship between aggregate prescription trends and two sets of events that shaped the statin market: patent expirations and generic entry on the one hand, and publication of national clinical guidelines on the other. Second, we investigated variation in prescribing activity across general practices. Third, we quantified the forsaken savings for the NHS by assuming perfect therapeutic substitution, that is by comparing actual treatment choices to a hypothetical scenario where only the most cost-effective treatments are prescribed.
Methods
Data
Our data are retrieved from Royal College of General Practitioners Research and Surveillance Centre (RCGP R&SC) database, a nationally representative sample of 243 general practices in England. The population representativeness of this database has been addressed in previous studies, including its representativeness of the distribution of cardiovascular disease in England.13,14 From this database, we retrieved all first prescription episodes for more than 400,000 patients treated with statins between Q3-2003 and Q4-2018. This database contains complete information of each prescription issued and an anonymised identity code of the general practice issuing the prescription.
We also retrieved from the Prescription Cost Analysis (PCA) database, yearly statistics on the total quantities of each drug prescribed in primary care in England, with the corresponding total spending, obtained from net ingredient cost (NIC). 15 This is the basic cost of a drug as used in primary care. NIC is used in Prescription Services reports and other analyses, as it standardises cost throughout prescribing nationally, and allows comparisons of data from different sources.
By aggregating the total spending of each strength of statin prescribed and dividing it by the corresponding total quantity, we obtained a measure of the average acquisition cost per strength of each statin in each year. In Appendix A, we compare the prescription data in the PCA dataset to those in the RCGP R&SC dataset to demonstrate that the latter constitutes a representative sample of national prescription of statins.
Trends and heterogeneity in statins prescription
Since 2003, the statins market has experienced five exogenous changes to prices and clinical standards as explained above that may have triggered changes in general practitioners’ prescribing choice. To document how prescription trends change in proximity of those events, we plotted the average proportion (across the 243 practices in the RCGP R&SC dataset) of new patients starting with one of the five statins for the period 2004 to 2018, as well as the average acquisition cost per defined daily dose for each statin. To explore heterogeneity in prescription patterns, we split general practices in the RCGP R&SC dataset into quintiles for every month in the data according to their share of new patients treated with simvastatin and plotted the average shares of new patients treated with simvastatin in each of the resulting five groups. Although this offers an insight into the evolution of overall heterogeneity in the data, it does not allow us to characterise persistency in general practitioners’ prescribing choices. Hence, we additionally plotted the average share of new patients treated with simvastatin, keeping the composition of groups fixed at the quintile computed at Q3-2003.
Cost savings simulation
According to NICE, all statins are equally therapeutically effective. As stated in TA-94 (2006), ‘from the evidence available […] [and] for the purpose of initiating therapy, there were no data on clinical events to suggest the superiority of any one Statin over all the others in reducing cardiovascular events’.10,16-20 Under the assumption that general practitioners cannot consistently anticipate whether a new patient would benefit from starting treatment with any given statin different from the one recommended by NICE, we evaluated prescription decisions according to a cost-minimisation criterion. Specifically, we quantified the potential savings for the NHS by comparing the actual cost of the observed prescription decisions with a hypothetical cost constructed by substituting the actual original treatments with a therapeutically similar treatment containing either simvastatin (before May 2012) or atorvastatin (from May 2012 onwards). By computing the difference between actual and hypothetic costs, we obtained a measure of the potential savings, both in absolute and relative terms.
The cost simulation was performed under two different scenarios. In the first scenario, the analysis was limited to the first 28 days of treatment for patients newly treated with statins. By focusing only on the first prescription episode, we compared the evolution of the spending on statin treatments using the same unit on analysis in different time periods, leaving aside the problem of following patients throughout their drug-treatment history. Clearly, the absolute value of savings obtained by considering only the first prescription episode for new patients is a partial account of the overall potential savings, as patients treated for cardiovascular disease risk will usually be on treatment indefinitely.
For this reason, we considered a second scenario where we computed hypothetical savings if practitioners had changed all (new and ongoing) patients to simvastatin (up to May 2012) and atorvastatin (after May 2012). This second simulation can be considered an upper bound to the absolute savings under the strong assumption that existing patients could be immediately switched to the NICE-recommended treatments, regardless of any patient’s preference or professional decision that led to the observed prescription choices. A detailed explanation of the methodology used for our cost simulation is presented in Appendix B.
Results
Trends in prescription and price
Figure 1(a) plots the evolution of the market shares for new patients starting treatment with statins between 2004 and 2018, using the RCGP R&SC database. In the time window considered, simvastatin and atorvastatin were the most frequently prescribed among the five statins, representing approximately 96% of all initial prescriptions. The dominance of these two drugs in treating cardiovascular diseases resulted in the evolution of their shares following mirror image patterns.
Trends in the statins prescribed for drug treatment initiation.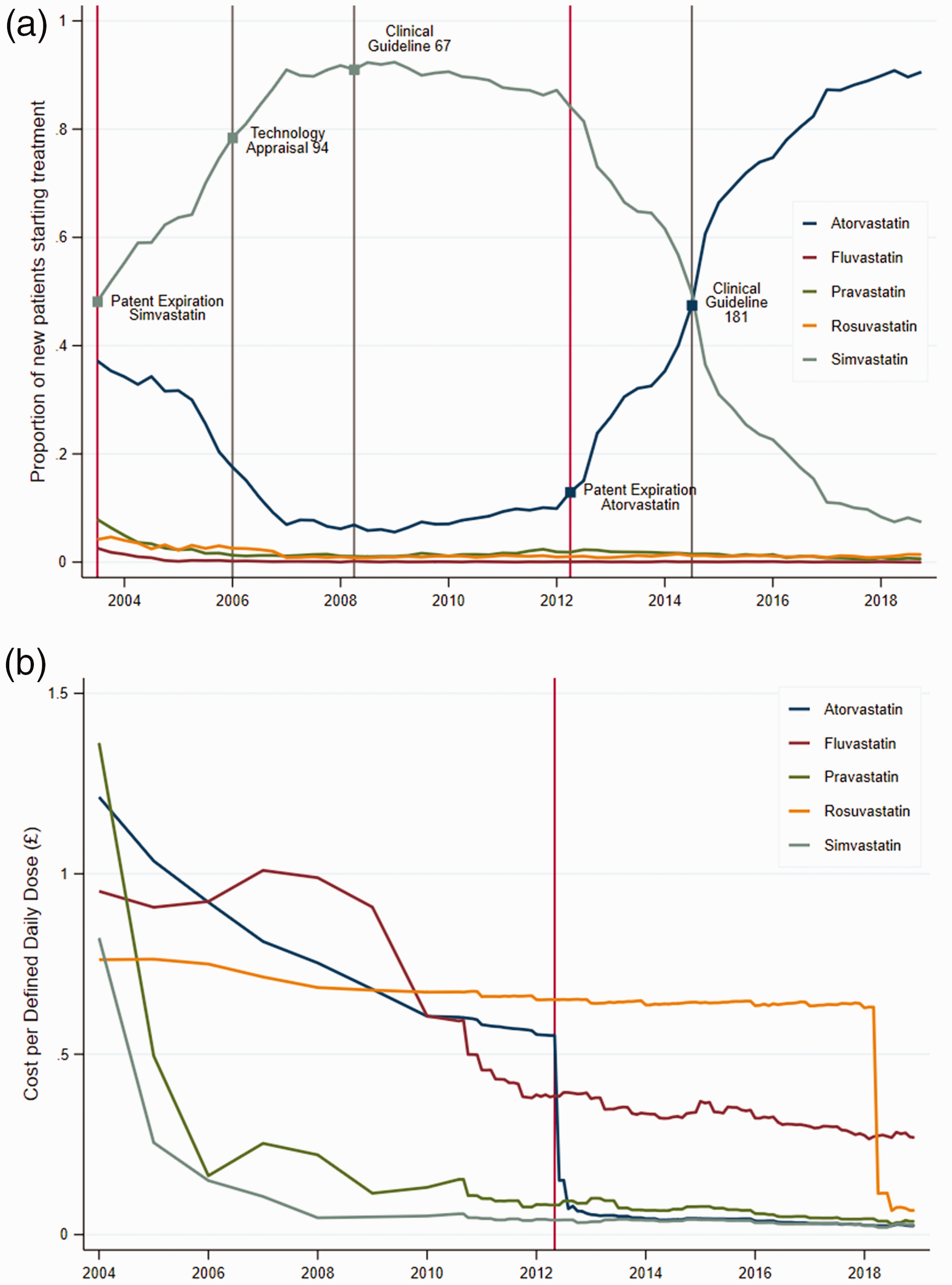
The share of simvastatin increased rapidly after its patent expiration in 2003, from around 50% to more than 90% in May 2008, when NICE published CG-67. While this guideline explicitly recommended simvastatin for treatment initiation, the percentage of new patients prescribed simvastatin stayed constant over the next four years up to May 2012, and, if anything, slightly decreased. We also note that the introduction of TA-94 in 2006 failed to accelerate the uptake of simvastatin. Upon atorvastatin’s patent protection expiration in May 2012, simvastatin’s share started decreasing steadily from around 85% in 2012 to around 10% in 2018. Once again, publication of CG-181 in 2014, updating the recommendation for treatment initiation to atorvastatin, had minimal effect in speeding up the declining trend of simvastatin.
Figure 1(b) shows the average acquisition costs per daily defined dose of each statin over time. The figure makes apparent the large drop in the acquisition cost of simvastatin soon after patent expiration of Zocor. 21 Similarly, a sharp drop in acquisition cost for atorvastatin (virtually similar to simvastatin) was observed shortly after Lipitor patent expiration.
Heterogeneity in prescriptions across general practices
Figure 2(a) presents average shares of new patients treated with simvastatin for each of the five quintiles of the general practices' prescription distribution. The figure reveals significant heterogeneity in prescribing choices across general practices during the time window of our study. When the simvastatin patent expired in May 2003, the proportion of patients treated with simvastatin ranged from less than 20% for general practices in the bottom quintile to more than 80% for the top quintile. The period up to 2006 saw an increase in the proportion of new patients treated with simvastatin across all general practices. At the time of the TA-94 introduction (January 2006), the difference between the second and fifth quintiles was around 20 percentage points, while the difference between first and fifth quintiles was still more than 50 percentage points. Following the introduction of CG-67 in May 2006, differences across practices fluctuated around 25 percentage points with most compliant with the NICE guideline practices treating almost all of their new patients with simvastatin, while least compliant practices prescribed simvastatin to less than 80% of their patients. Heterogeneity in prescription increased again following atorvastatin patent expiration in May 2012, when the difference in the share of new patients being prescribed simvastatin between the top and bottom quintiles reached about 50 percentage points. The subsequent CG-181 further reduced the overall levels of simvastatin prescriptions across the distribution but did little to reduce heterogeneity in the share of patients treated with simvastatin in the following years, with the difference between the top and bottom quintiles remaining at about 25 percentage points.
Figure 2(b) tracks the evolution of prescription for five quintiles of general practitioners as constructed in Q3-2003. The dynamics up to 2006 suggest the uptake of cost-effective prescribing for general practitioners in the lower quintiles is rather slow. However, the disappearance of major differences in prescribing among the five groups from 2007 onwards indicates that any given general practice does not systematically deviate from prescribing the cost-effective statin. These dynamics suggest that the overall heterogeneity observed in panel (a) is due to slow learning and fluctuation between cost-effective and non-cost-effective prescribing.
Heterogeneity in initial prescriptions at the general practice level.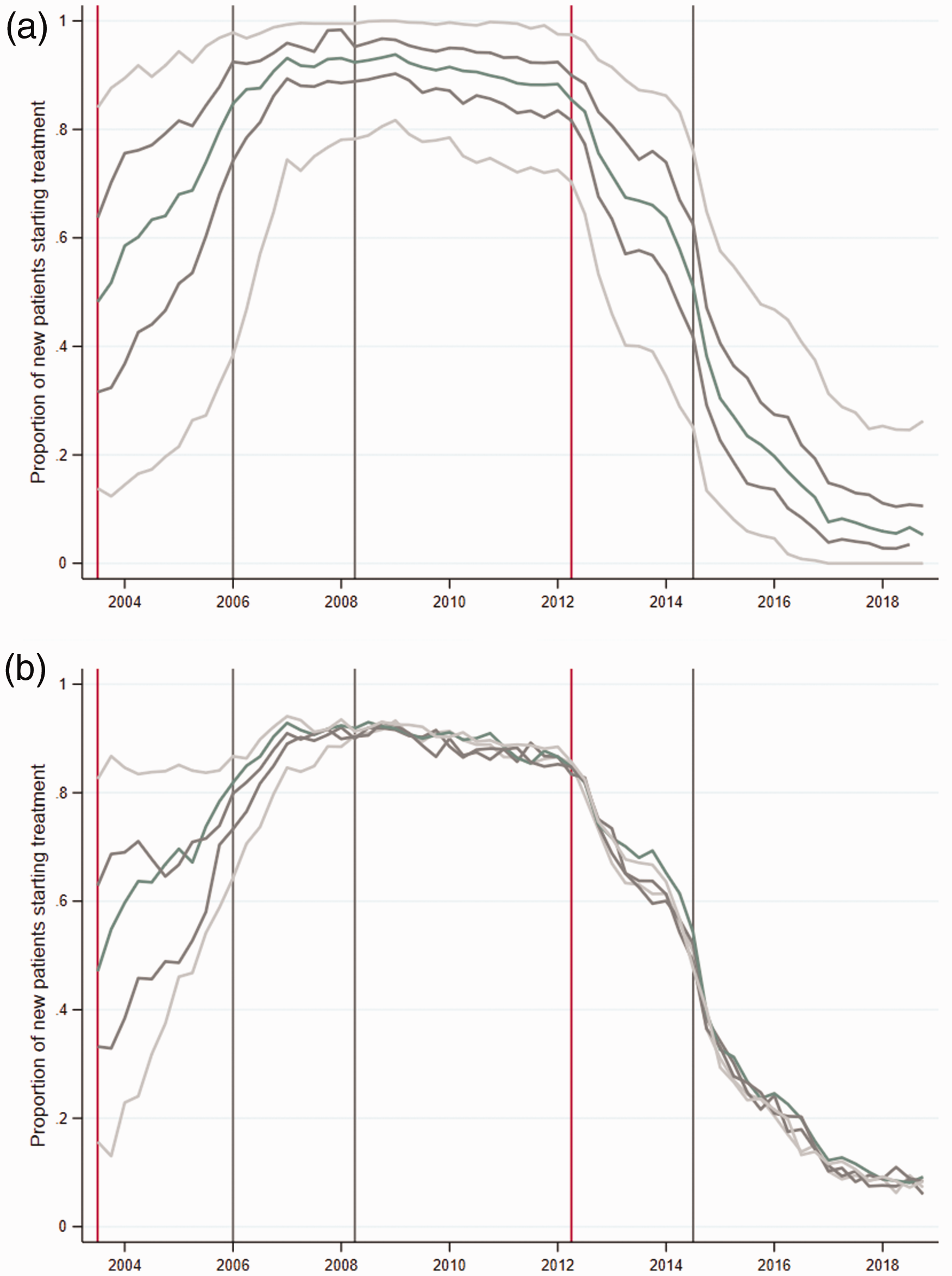
Spending simulations
Spending simulation exercise.
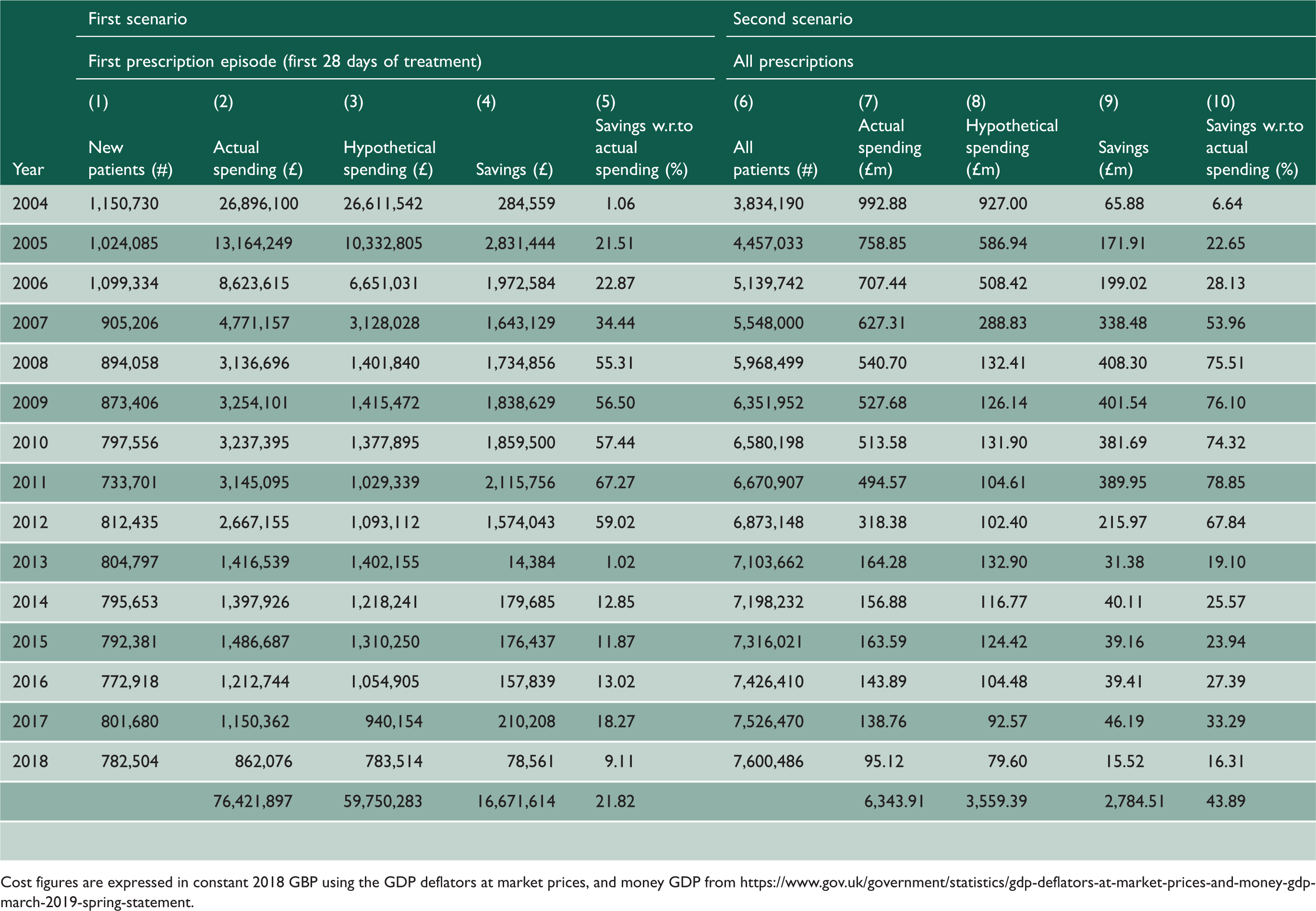
Cost figures are expressed in constant 2018 GBP using the GDP deflators at market prices, and money GDP from https://www.gov.uk/government/statistics/gdp-deflators-at-market-prices-and-money-gdp-march-2019-spring-statement.
Overall, a saving of £16.67 million, or 21.8% of the total actual cost could have been realised for the first 28 days of treatment alone if general practitioners had prescribed simvastatin as initial drug treatment before May 2012 and atorvastatin after May 2012. Most of the hypothetical savings accrued over the period 2008–2012 when cheap generic versions of simvastatin became available and atorvastatin was still under patent protection. After May 2012, once generics of atorvastatin also entered the market, hypothetical savings on first prescription episodes were mainly accredited to switching from rosuvastatin to atorvastatin. However, the implied savings were not large as rosuvastatin only held a small share of the market.
Results for the ‘Second Scenario’ regarding total prescriptions for all existing patients are presented in the right-hand side panel of Table 1. The total number of patients on treatment every year increased from 3.8 million in 2004 to 7.6 million in 2018. However, the significant drop in price due to generic entries led to a drastic drop in spending over the same period: from just under £1 billion in 2004 to £95 million in 2018, a 90-percentage decrease. Cumulate spending on statins over the period 2004–2018 totalled £6.3 billion and estimated potential savings were £2.8 billion, or 43.9% of the actual spending on statins. As previously, large savings could have been obtained in the period 2004–2012 by switching patients from atorvastatin, which was available only as a branded drug, to simvastatin, that was generic.
Discussion
In resource-constrained healthcare systems, promoting cost-effective prescribing behaviour is an important component of their cost-containment strategy. Using data on statins, we investigated how general practitioners' prescription choice in England changed in the face of (i) a large reduction in the cost of available treatments and (ii) the introduction of specific clinical guidelines. We demonstrated substantial increases in market shares for simvastatin and atorvastatin as their patents expired and generics entered the market, but well before the introduction of NICE guidelines recommending their use.
Those trends suggest that practitioners in primary care are sensitive to the price of alternative treatments, and that their choices even anticipate the recommendation of future clinical guidelines. Indeed, it took four years from the generic availability of simvastatin for NICE to explicitly recommend it for treatment initiation, by which point the share of new patients being prescribed the drug was already at 90%. Similarly, migration from simvastatin to atorvastatin started soon after a generic became available in May 2012, despite the fact that atorvastatin was only recommended as the preferred treatment in the updated NICE guideline two years afterwards.
Previous studies have shown that medicine management teams from CCGs do play a role in informing and influencing practices’ and practitioners’ prescription choices.3–5 Whether prescriptions are autonomously chosen by general practitioners or are influenced by the different actors within the primary care sector, our results suggest that ultimately prescribing decisions are more responsive to the acquisition cost of alternative treatments than clinical guidelines.
Although our analysis shows that, on average, practitioners treating patients at risk of cardiovascular events prescribed cost-effectively, we also identified substantial heterogeneity in prescription across practices, which remained even after the publication of official guidelines. Our descriptive analysis indicates some general practitioners took longer to adopt cost-effective prescribing and some switched in and out of cost-effective prescribing throughout the study period, generating large overall heterogeneity. A number of explanations can be offered for such behaviours. For example, medicolegally, general practitioners may have felt inhibited to change prescribing habits simply on the basis of cost, without having had guidelines to justify the decision. 22 Equally, general practitioners' and patients’ characteristics, practices’ characteristics, geo-social conditions, as well as local CCG prescribing guidelines and monitoring activities may influence prescribing decisions. 23 Moreover, statins have been widely perceived as causing side effects such as muscle pains (with intermittent media coverage influencing prescribing behaviour). 24 General practitioners and patients may have been reluctant to switch statins for fear of inducing adverse events. 25
Under the plausible assumption that general practitioners cannot consistently anticipate whether a new patient would benefit from taking a drug other than the one recommended by NICE, we evaluated prescription choices in this market according to a cost-minimisation criterion where choosing statins other than simvastatin (before May 2012) or atorvastatin (after May 2012) can be considered suboptimal. Our cost-savings simulation analysis suggested that low responsiveness comes at a high price for the NHS. Namely, if all new patients had received the most cost-effective treatment (as later recommended in the guidelines), the NHS could have saved around 22% of the actual spending on initial prescriptions. Looking at all prescriptions for new and on going patients, we compute savings of £2.7bn, mainly between 2004 and 2012, representing roughly 44% of total spending on statins during this period. We acknowledge that this figure is an upper bound of potential savings, based on the strong assumption that all existing patients on drug treatment could be seamlessly switched to other statins, without considering side effects (e.g. myopathy) or other practicalities (e.g. planned-patient reviews) . Looking at the data, we found that around 7% and 12% of patients were switched to simvastatin and then switched away from it in the next 4 and 12 months, respectively. Although these numbers suggest that simvastatin cannot be used by a non-insignificant proportion of patients, there is no doubt that there were still large savings to be made by prescribing the most cost-effective statins.
We anticipate that the experience of statins would be similarly observed in other therapeutic areas where treatments have similar modes of action and comparable levels of efficacy, for instance angiotensin-converting enzyme (ACE) inhibitors and proton pump inhibitors. Looking ahead, our analysis suggests that cost-conscious centralised public health systems could save substantial sums if new and, whenever possible, on going patients are promptly switched to cost-effective alternatives, in particular when the first medicine in a therapeutic class loses patent protection. The observed heterogeneity in prescribing behaviour suggests that an important step forward towards achieving this goal would be a timely dissemination of best practices, with the aim of promoting cost-conscious prescribing behaviour. In the UK, where general practices are grouping into Primary Care Networks and there is growing co-working and co-location with pharmacists, such collaborative efforts are likely to drive future prescribing. Given general practitioners' limited time available to acquire information on market developments (e.g. new medicines coming into the market or brand-name medicines losing patent protection) across all drug classes they prescribe, there is an important role for academic detailing as well as online/computerised systems and prompts such as ScriptSwitch, rather than paper-based (e.g. Prescribing Outlook), to educate and offer updated advice on cost-effective medicines while preserving physicians’ freedoms to prescribe and patients’ ability to discuss their preferred choice of treatment. 26 It is of note that the recently announced NICE strategy for 2021 to 2026 aims to ‘provide dynamic, living guideline recommendations that are useful, useable and rapidly updated’ (p. 19). 27
Strengths and limitations
We study prescription dynamics of statins, a class of drugs widely prescribed in primary care, using a representative dataset of English practices for the period 2004–2018, a time window that includes patent expiration of brand-name statins and publications of new NICE guidelines. There is no reason to believe that the large forsaken savings we have identified would not generalise to other important therapeutic areas of the English NHS or to other healthcare systems. Admittedly, the extent of the savings is an empirical matter and crucially depends on the structure of healthcare systems, the penetration of generics within them and the incentives of different players in prescribing, dispensing, and reimbursing pharmaceutical treatments.
We acknowledge a few limitations for this study. We only observe a first prescription issued to patients treated in primary care, without being able to account for prescribing influences coming from other settings. For example, patients experiencing a first cardiovascular event may have received their first statin prescription in secondary care, and such decision might have influenced ongoing prescribing in primary care. However, it is unlikely that this would explain all of the heterogeneity in prescribing choices and the large forsaken savings shown in Table 1. Further, we had access only to limited data on general practitioner characteristics to examine factors associated with the observed heterogeneity, while analysis of free text from clinical records to explore documented decisions related to statin prescription choice was beyond the scope of this project.
Conclusions
Percentage reduction in low-density lipoprotein cholesterol.
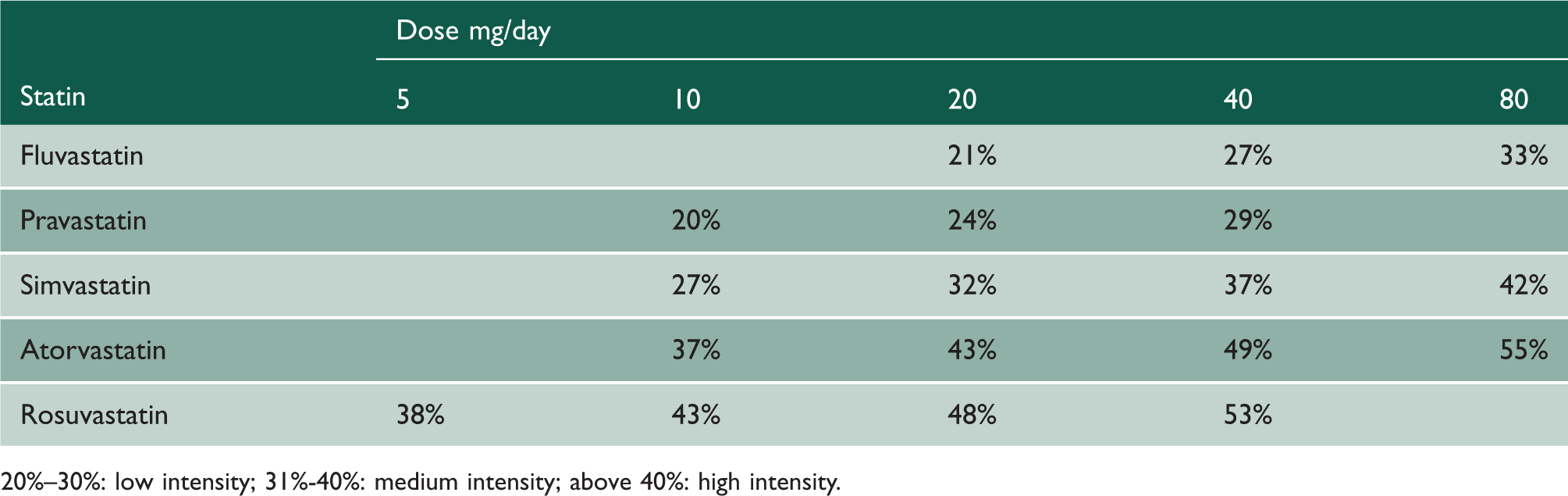
20%–30%: low intensity; 31%-40%: medium intensity; above 40%: high intensity.
Correspondence between all statins’ treatments based on low-density lipoprotein cholesterol reduction.
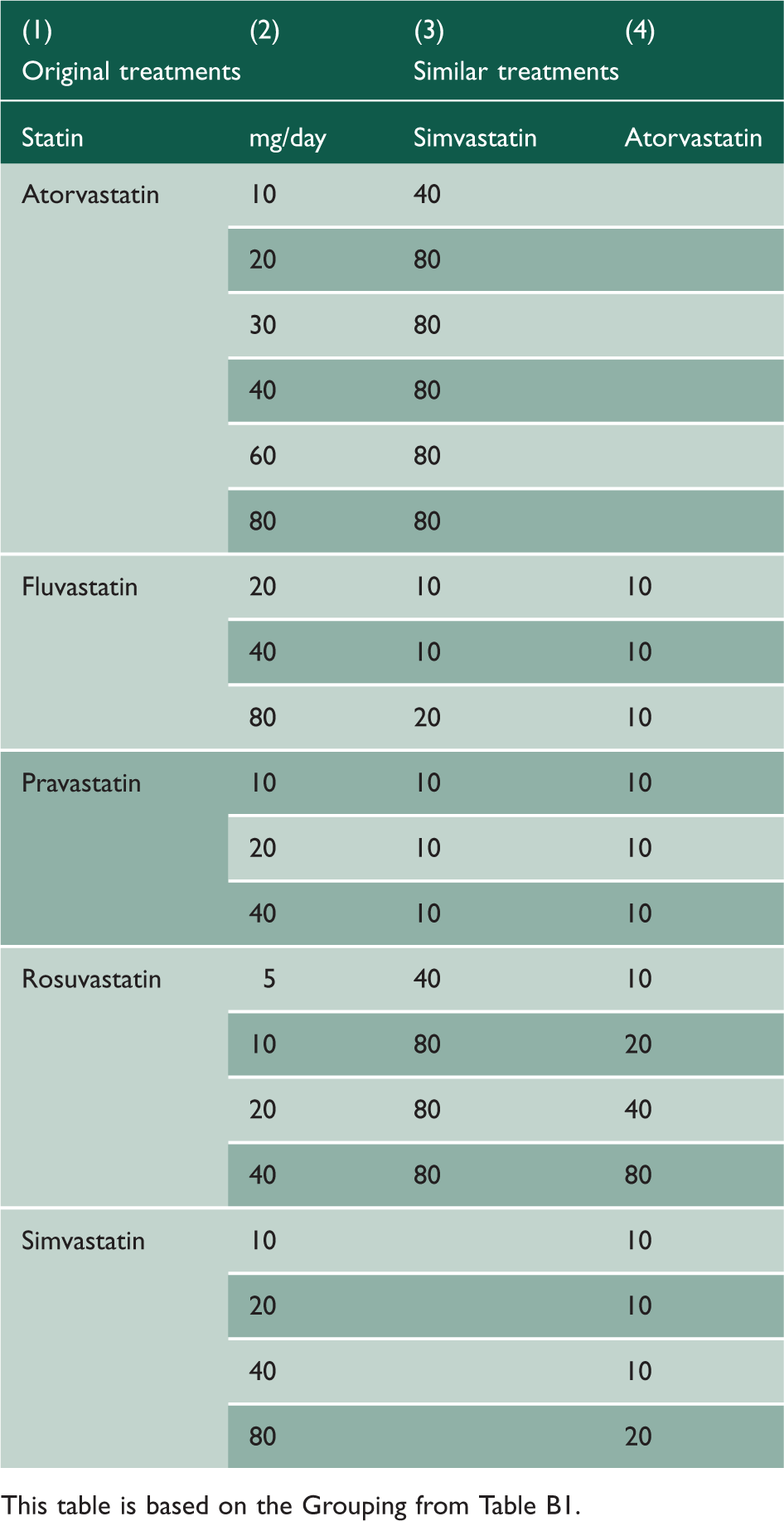
This table is based on the Grouping from Table B1.
Supplemental Material
sj-pdf-1-jrs-10.1177_01410768211051713 - Supplemental material for Price versus clinical guidelines in primary care statin prescribing: a retrospective cohort study and cost simulation model
Supplemental material, sj-pdf-1-jrs-10.1177_01410768211051713 for Price versus clinical guidelines in primary care statin prescribing: a retrospective cohort study and cost simulation model by Matias Ortiz De Zarate, Emmanouil Mentzakis, Simon DS Fraser, Paul Roderick, Paul Rutter and Carmine Ornaghi in Journal of the Royal Society of Medicine
Footnotes
Declarations
Acknowledgements
We would like to thank the patients for allowing their data to be used for surveillance and research. Practices who have agreed to be part of the Oxford RCGP RSC and allow us to extract and used health data for surveillance and research. Filipa Ferreira (Senior Project Manager) from RCGP and from University of Surrey. Apollo Medical Systems for data extraction. Collaboration with EMIS, TPP, In-Practice and Micro-test CMR supplier for facilitating data extraction. Colleagues at Public Health England.
Provenance
Not commissioned; peer-reviewed by Julie Morris.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.