
Abstract

Humanity has but 3 great enemies: fever, famine and war: of these by far the greatest, by far the most terrible, is fever
Sir William Osler (1896)
In 2020, global civil aviation came to a near-complete stop when it was realised that aeroplanes and airports serve as major routes for the spread of COVID-19. 1 Governments, the general public and the air-travel industry must now rethink the trade-off between public safety and the cost of screening all passengers for contagious diseases. My purpose is to demonstrate how these concerns were raised 81 years ago by Dr John Robert Draper, medical officer at Britain’s first major international gateway via air, Croydon Airport. Draper’s report, published on 7 January 1939 in the Supplement of the British Medical Journal, drew scant notice and his concerns were dismissed by authorities.2,3 We cannot afford to do likewise.
Recent events in historical context
On 22 January 2020, in response to increasing cases of COVID-19 in China and its spread beyond its borders, it was announced that the UK’s main international airport, Heathrow, would implement enhanced surveillance and set aside an isolated area of its Terminal 4, for receiving direct flights from Wuhan, Hubei Province, China. British epidemiologist Neil Ferguson cautioned that would ‘only identify people who have symptoms as they come off the plane’. 4 It took less than a week to prove him correct. 5
On 23 January 2020, unknown at the time to be in the incubation phase of her illness and infectious to others, an asymptomatic woman arrived in the UK on a long-haul flight from Hubei Province and developed fever three days later. She became the first laboratory-confirmed case of COVID-19 in Britain on 31 January. 5 Shortly thereafter, a British man who had begun his journey in Singapore, but who arrived at Heathrow on one of many short-distance flights from France, became the UK’s third confirmed case. 6 Clearly, surveillance confined to a few direct flights from countries affected by COVID-19 would not suffice. Ferguson subsequently stated ‘that approximately two-thirds of cases in travellers from China have not yet been detected. It is highly likely that some of these undetected cases will have started chains of transmission within the countries they entered’. 7
The year 2020 marks the centenary of Croydon Aerodrome (also known as the Airport of London). Officials in the 1930s grappled with the issue of how best to protect the public from contagious diseases. Answerable to Croydon Council’s Medical Officer of Health, Oscar M. Holden, Draper determined that efforts in this regard were wholly ‘inadequate’. His concerns were remarkably similar to Ferguson’s, and he may have lost his job for speaking out too strongly.3,8
Dr John Robert Draper: the devolution of a job description
Little is known about Draper. A graduate of Cambridge, he entered the Medical Register in 1907. On 1 January 1931, as a consequence of the expansion of global air travel, he was appointed to Croydon Airport as the medical officer under the Aliens Acts. He described his duties as including ‘among other things: (1) inspection of passengers in order to prevent the admission of cases of infectious disease; (2) physical examination of certain aliens; (3) examination of foodstuffs; and (4) examination of birds of the parrot tribe under the Psittacosis Order’. The latter activity took up much of his time, and he reported that ‘during my eight years at the aerodrome I have only been specially called to see passengers on three occasions, because the immigration officer would never risk the delay unless he was certain that the passenger would be refused permission to land for medical reasons’.3,8
Draper’s job description can be traced to the Aliens Order of 1920, which required inspecting ‘foreigners’ to prevent medically unfit ‘undesirables’ entering the country. Such inspection did not usually require a medical officer, being largely in the domain of immigration. He was employed in the wake of a 1930 report issued by the International Sanitary Convention for Aerial navigation by the Office International d’Hygiene in Paris.9,10 The final text of that report was opened for signature in 1933 in The Hague and it went into force two years later, in August 1935. It contained 67 Articles comprising the ‘maximum measures’ to prevent the spread of cholera, plague, louse-borne typhus, smallpox and yellow fever, and left ‘their actual application to each country concerned’, with the resulting Public Health (Aircraft) Regulations of 1938 for the UK.9,11
The years 1935–1938 brought heightened recognition to the role of air travel in the spread of infectious diseases. By 1936, it became possible to fly between London and its various Empire destinations, all within the incubation time of smallpox.12,13 In 1936, Draper’s entry on the risks of yellow fever with air travel appeared in the journal Medical Officer.14,15 In 1938, Air Commodore H.E. Whittington summarised these dangers in an address to the Royal Society of Medicine, where he reminded his audience that air travel ‘brought various parts of the world closer together as regards time… [and]… is so rapid that an aeroplane departing from the yellow-fever zones of West Africa reaches the Sudan in two days, Mozambique in four days, Durban in five days and, by another route, Karachi in five, Calcutta in six’. 12 The fear of yellow fever entering India had the consequence of both stringent exit screening in Africa and strict precautions on arrival in India.12,15
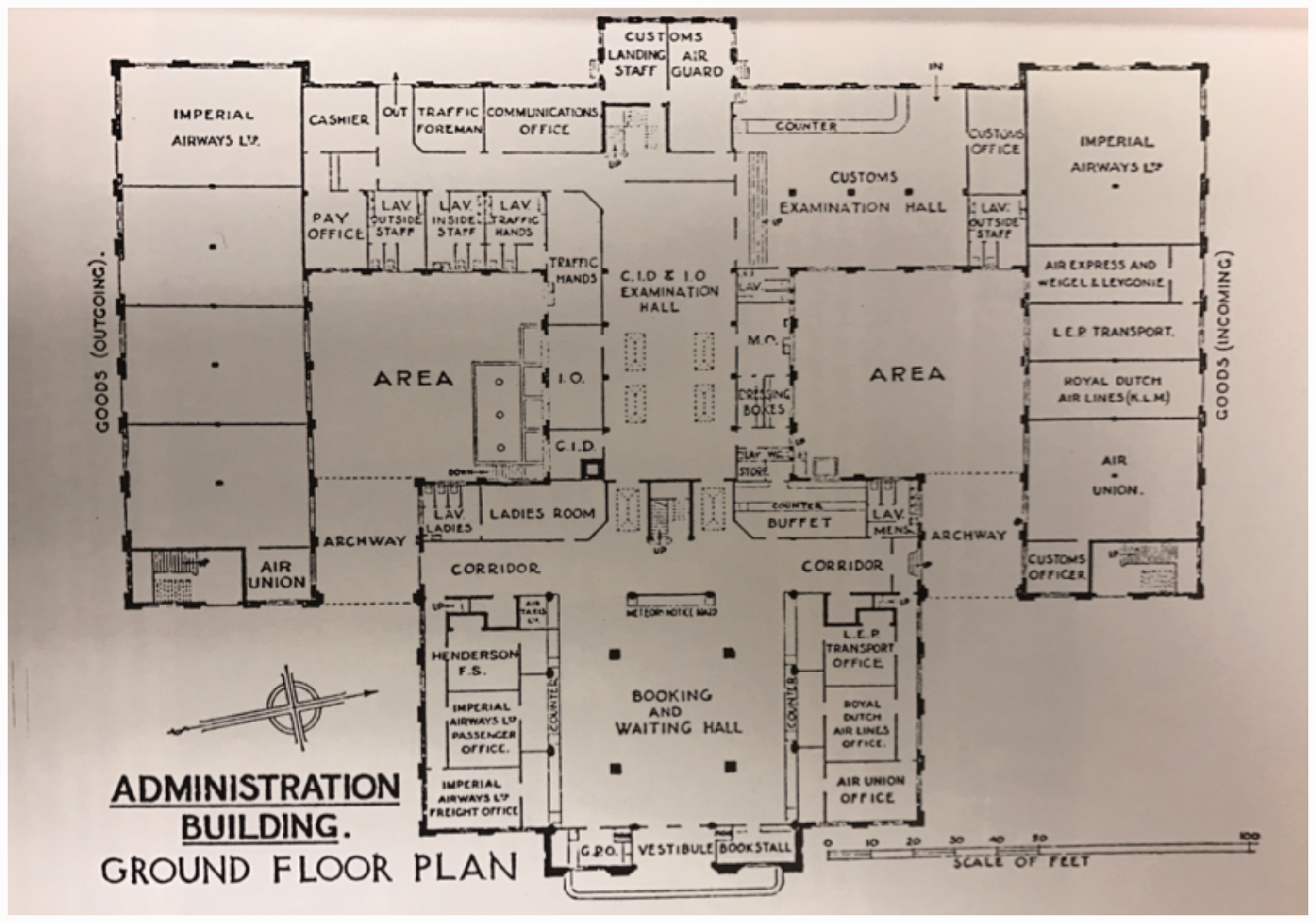
The years 1935–1938 also brought modifications to Draper’s job description, with his hours of duty increasing significantly from December 1935, as passenger numbers increased. The importance given to carrying illegal documents, prohibited items or an infection is reflected by observing the obvious passenger route as seen in the Airport floor plans. While immigration and customs occupied large main forefront halls, the medical officer remained in the confines of a small private room. Dialogues published regularly in Flight Magazine add to the sense that there was little interest in the medical officer, despite a lurking threat of fever by flight.3,16
In late 1938, ‘a new arrangement between the Ministry of Health and the Croydon Corporation’, as a result of the Public Health (Aircraft) Regulations 1938, stipulated that the medical officer would be present ‘for only two to three hours a day for six days a week’. Draper’s role had been marginalised. Whether he was fired or resigned in protest over the reduced work hours is unclear, but he was no longer the medical officer when he prepared his report in 1939.
3
Airport of London, Croydon. HCAT.
8
Children arriving at Croydon Airport from Prague, 11 January 1939, four days after Draper’s paper. HCAT.
8
Croydon Airport, ground floor plans. HCAT.
8

Dr John Robert Draper: the whistle-blower’s report
Draper observed that while it was the policy at Croydon to screen select passengers from countries where smallpox was prevalent (for example, Egypt, the Sudan, Central Africa, India, Malaya, and Southeast Asia), such flights were few or ‘practically non-existent’. The greater danger pertained to passengers who began their journeys in countries where infectious diseases were prevalent but arrived at Croydon on the many flights from Amsterdam, Brussels or Paris, places with their own Empire routes. Therefore, It follows that any aeroplane arriving at Croydon may bring passengers from infected places as well as those from the nearer European capitals, and there is at present no means at Croydon of distinguishing which passengers come from infected and which from uninfected countries …. This country is therefore wide open for the admission of cases of small-pox or any other infectious disease all the time for those in the incubation period, and all the time except for the two or three hours a day when the medical officer is on duty for those in the eruptive stage. Surely this is a most appalling state of affairs.
3
I am informed that the objection to any proper control at Croydon is its cost …. But regarded as an insurance premium against a very grave risk the cost would not, I venture to think, be found excessive, and the prevention of an epidemic would be well worth the price. 3
Aftermath
Draper’s article triggered a mere handful of responses in the press. Although a few headlines screamed ‘Croydon, wide open to smallpox’, the media chose to focus on other problems such as unemployment and unease about the Nazi regime in Germany. A box in the Croydon archives bears witness to tensions within interwar Europe, including passports withheld by immigration between 1938 and 1939. Four days after Draper’s report was published, a group of children arrived at Croydon from Prague as part of the Kindertransport. Any political action was in response to fear of war, not fever. 8
Later that month, Holden responded to Draper in a letter to the British Medical Journal. He said Draper had a ‘relatively minor post’, proposed optimistic futile suggestions and was ‘misleading’. Holden held that any possible loopholes were closed by the new 1938 regulations and challenged whether Draper knew of any other country that did it better. As to the well-known ‘problem of long-distance passengers who break their journey once or more en-route’, everyone would need to be questioned and any health declaration documents would importantly rely on honesty.
10
In February 1939, Draper’s concerns were presented at the House of Commons. The Minister of Health appeared satisfied and reassured by government regulations and annual medical reports from Croydon’s Council.
2
The last comments on the issue were in July of that year. In September 1939, Croydon as a civilian airport closed, not because of contagious disease but because of the outbreak of World War II. How vital Draper’s role was considered is further reflected in his relative absence from the Airport Archives and history books about the Airport.8 The more things change, the more they stay the same
Jean-Baptiste Alphonse Karr (1848)
Past as prologue
Perhaps things will turn out differently this time around. On 26 February 2020, at a House of Commons sitting, enquiring about precautionary measures for COVID-19 at Heathrow, surgeon and MP Philippa Whitford indicated ‘we can no longer think that this only involves people who come from a few countries—people follow different routes, and almost everyone coming in would need to be screened’. 18
Lessons already gleaned from COVID-19, along with those from previous outbreaks, epidemics and pandemics spread by air travel (smallpox, influenza, yellow fever, SARS and Ebola, to name just a few) should prompt concerted attempts to screen all passengers for contagious diseases and support an expanded role for the field of Travel Medicine.
19
After all, and as evinced by the warnings of William Osler (1896) cited above and Michael Osterholm (2017) cited below, contagious diseases can be even more dangerous than concealed weapons, for which high-technology screening is already in place. We live in a world where it's a just-in-time delivery system, where we've eliminated oceans, mountain ranges, political boundaries, any kind of way of stopping infectious diseases from moving from one part of the world to another.
Micheal T. Osterholm (2017)
Footnotes
Declarations
Competing interests None declared.
Funding
None declared.
Ethics approval
NA.
Guarantor
AH.
Contributorship
Sole authorship.
Acknowledgements
This work would not have been possible without the insight and support of late Peter Skinner of the Historic Croydon Airport Trust. I am especially indebted to Charles S. Bryan, Professor Emeritus of Internal Medicine and world authority on Sir William Osler and Dr. Christopher Gardner-Thorpe, neurologist and Lecturer and Examiner in History.
Provenance
Not commissioned; peer-reviewed by Yuri Zagvazdin.