
Abstract

This article is in our series on social prescribing
The task of the economy is to deliver and to enable prosperity […] our ability to flourish: physically, psychologically and socially.
1
Societies that enable all citizens to play a full and useful role in the social, economic and cultural life of their society will be healthier than those where people face insecurity, exclusion and deprivation.
2
Investing resources to promote population health
Investment embodies one of the most vital relationships in economics – namely, the relationship between the present and the future […] Engaging in projects that last over time embodies our commitment to the future and is the basis for prosperity of any kind […] Investment is the vehicle through which we build, protect and maintain the assets on which tomorrow’s prosperity depends. 1
All investment decisions made by those responsible for allocating health and care resources have an impact. Some of the impact is intended and some unintended; some positive, some negative (Figure 1).
Impacts of investments.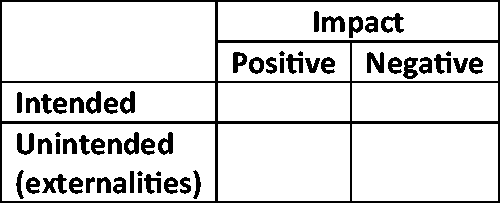
Layered onto investment decisions are also considerations of opportunity cost and creation of value – resources are limited by definition and if we invest them on things that do not deliver the highest value possible, with value in healthcare defined as delivering the best patient and population level outcomes while optimising resource utilisation,
4
we are not fulfilling our duty as stewards of the resource: The stewardship concept demands that we constantly ask the question: Will the resource be in better shape after my stewardship?
5
Why have we allowed this to happen? Two underlying reasons are because of healthcare’s over-reliance on the biomedical model and our, oftentimes, misguided views on Return on Investment.
First, the focus on just the biological aspects of illness begins upstream with research agencies who allocate far greater resources into basic science, translational and clinical/healthcare services research relative to understanding how to prevent disease, promote health and address social factors (for example, of the ∼£2 billion distributed by the UK’s two largest health funding agencies, public health and prevention only account for ∼2% of the UK National Institute for Health Research’s Research and Infrastructure budget 7 and ∼4% of the UK Medical Research Council’s budget, 8 respectively). There is much rhetorical weight given to statements like ‘an ounce of prevention is worth a pound of cure’, but disease prevention, health promotion and addressing social factors is complicated and requires that we take account of qualitative and contextual factors which is a contrast to the prevailing reductionist biomedical approach. Further to this are considerations around timeframes to impact and attribution. Because the biomedical model often time focuses mostly on symptom treatment, timeframes to impact are shorter and attribution is much more straightforward relative to helping an individual manage their condition or supporting them to prevent disease, improve their health and/or address social factors.
Second, there is the larger issue of return on investment. The major focus of investments, whether public or private, has been to generate financial return on investment and this drives investors to hold themselves accountable only to financial targets – indeed looking at the annual reports of two of UK largest health research funders attests to the importance of this.7,8 For research funders, researchers, innovators, investors and healthcare payers, the prevailing ideology is that biomedical based interventions are the easiest means to a healthy financial return on investment and savings. This misdirected pursuit of financial return on investment leads to dangerous and unsustainable market distortions because of Intellectual Property Rights, Value Based Pricing and financial engineering 9 all at the opportunity cost of addressing important issues related to social factors of illness.
Investing resources to promote population health: the essential role of social prescribing
Social prescriptions provide ‘a way of linking patients in primary care with sources of support within the community to help improve their health and well-being’. 10 Social prescriptions can address mental and physical health through activities such as sports and leisure/arts and can address social factors through activities more focused on social issues (housing, food, etc.), education or skills development. 11 If utilised properly, social prescriptions can deliver several benefits including addressing social factors, promoting self-care and improving management of long-term conditions, all while optimising resource utilisation and contributing to better patient experience, satisfaction and outcomes. 4
Though there has been a push to support the use of social prescriptions in the English NHS through the Universal Personalised Care Plan, 12 the uptake and spread by commissioners, clinicians and patients have been limited and heterogeneous as evidenced by a recent analysis that shows that in London alone, there were approximately 250,000 patients who could have benefited from a social prescription but did not receive one – something that could have resulted in £90 million in savings to the NHS. 13
A rate-limiting step in the more active use of social prescriptions is the availability of resources throughout the life cycle of social prescriptions, including research and evaluation to explore the design and delivery of more effective models as well as an assessment of their impact; private investment to facilitate the growth of social prescription providers and the creation of new technology to augment social prescriptions; and public/private/philanthropic funding models to support the social prescribing ecosystem. 4
Research and evaluation
The evidence base around social prescriptions is steadily growing but is not yet very robust. This is a challenge that could be readily addressed if research agencies allocated more funding to support the design and assessment of social prescriptions. Further to this, research agencies will likely need to adopt more flexibility in the types of studies they fund because social prescriptions often need a process of continuous development, adjusting and testing. This could actually be advantageous because unlike pharmaceutical and biotech interventions, social prescriptions can be rapidly modified so they can be tested through models such as pragmatic control trials which are usually much less resource-intensive, with regard to both time and money, than traditional randomised controlled trials. 14
Another advantage for social prescriptions is their ability to be easily augmented through technology. Leveraging Information Technology (Artificial Intelligence, machine learning, Internet of Things and living services strategies) and Big Data (including the integration of -omics data) could see the agile development of technology-augmented social prescriptions that could disrupt the paradigm of how health and care are delivered. 14
Investment to grow innovations
There is a significant opportunity for private investment into social prescriptions, particularly the technologies which can augment them. Solow’s work has shown that 80% of economic growth can be explained through improvements in the use of technology, 9 which provides a powerful justification for more public research funding going towards the development and use of Information Technology-augmented social prescriptions as well as for a greater proportion of private equity funding in healthcare to be allocated to this domain.
Funding models to support the social prescribing ecosystem
The English NHS allocates approximately £16 billion annually for pharmaceuticals. Compare this to £44 million, a generous estimate of how much Clinical Commissioning Groups in England may have invested in social prescriptions from 2017 to 2018 if we extrapolate the results of a survey of 55 Clinical Commissioning Groups. 15
There are some obvious reasons for this massive 350-fold greater investment in pharmaceuticals relative to social prescriptions: pharmaceuticals are the incumbent; there is more evidence for them; and they fit into workflows which have been designed around their use. But this does not mean that we should simply accept the status quo because social prescribing, as highlighted above, has the potential to address many health-related issues that pharmaceuticals and other biomedical interventions will never be able to address.
Different funding models that could be used to support the social prescribing ecosystem.

Social Px: social prescriptions; CCG: Clinical Commissioning Group.
aModels which could theoretically be used to support the social prescribing ecosystem.
Below we give some examples of how some of these schemes have been put into practice:
Public funding
The Rotherham Clinical Commissioning Group directly funds the voluntary sector, which has led to major benefits for the local authority in relation to public health and social care services. 16
The Newham Clinical Commissioning Group paid £4 per patient per class to providers to deliver a range of physical activity classes (gym sessions, Bollywood dance, Zumba, Quadro, yoga, Tai Chi, swimming, chair-based exercises, African dance, Line dance, Salsa and Quadrille) in locations, such as libraries, that were accessible to local residents. 16
Shared investment
Clinical Commissioning Group + Local Authority: Exeter and East Riding in Yorkshire tested models that combine funding from Clinical Commissioning Groups and funding from community development, as well as adult and social care within local authorities.
Combo investment
Public + private + philanthropic: Ways to Wellness in Newcastle is a Social Impact Bond that has 22 full-time equivalents targeting 14,000 people with specific long-term conditions which has demonstrated positive balance and generating savings for the NHS. 17
The way forward
Our current models of investment for health and care services leave much to be desired as highlighted by rising inequalities and decreasing life expectancies in high-income countries including the UK.
4
Social prescribing offer a promising solution to address many of the challenges we currently face and although recent commitments from the English NHS to increase investments in social prescribing are promising,
4
the scale of the challenge we face means that more thought, work, resources and risk-taking will be needed in the investments we make if we hope to address the unmet needs in our society and, more importantly, to tap into the potential we have as a wider health and care community to improve population health. Prosperity today means little if it undermines prosperity tomorrow. Investment is the vehicle through which we build, protect and maintain the assets on which tomorrow’s prosperity depends.
1