
Abstract
Summary
A significant loss of bone mineral density and the appearance of multiple vertebral fractures after discontinuation of denosumab treatment have been described. To date, no hip fractures have been reported. We present three cases of patients who suffered femoral fractures after denosumab suppression.
Introduction
Denosumab is a drug approved in Europe for the treatment of post-menopausal osteoporosis. 1 However, it has recently been described that, when denosumab is suspended, a damaging rebound effect is observed with a sharp decrease in previously gained bone mineral density, and spontaneous vertebral fractures occurring in up to 25% of these patients, which tend to be multiple.2–7
To date, only vertebral fractures have been described. In this paper, we present the cases of three patients who suffered hip fractures after denosumab treatment was discontinued.
Case 1
The first case is an 85-year-old woman, diagnosed with osteoporosis in May 2010 by densitometry (bone mineral density at the femoral neck: 0.481 g/cm2; T-score: −3.3). She had not previously suffered fragility fractures. She was treated with alendronate from May 2010 to December 2013. She started treatment with denosumab, calcium and vitamin D in January 2014, which she maintained until January 2018. In April 2016, an increase of bone mineral density of 22.8% was observed at the femoral neck (bone mineral density: 0.573 g/cm2; T-score: −2.4) compared with the densitometric value carried out in April 2012 (bone mineral density: 0.467 g/cm2; T-score: −3.4). In the month of July 2018, she forgot to administer her dose. On the same date (July 2018), a densitometry was carried out, which indicated a loss of 13.8% in bone mineral density of the femoral neck (bone mineral density: 0.495 g/cm2; T-score: −3.2) compared to the densitometry carried out in April 2016. At 8 months after the last dose (September 2018), she suffered a fall fracturing the proximal extremity of the femur. She was intervened initially by placing nails, and underwent another surgery on November 29 to implant a complete prosthesis.
Bone turnover markers were analysed and measured three months after the fracture (December 2018): P1NP (procollagen type I N-propeptide, bone formation marker) was extremely increased (637.4 ng/mL) and TRAP (Tartrate-resistant acid phosphatase, bone resorption marker) had values above normal (4.4 ng/mL). Beta-crosslaps (CTX or carboxy-terminal collagen crosslinks, resorption marker) and osteocalcin (OC, formation marker) were within normal values, as were PTH and vitamin D.
Case 2
The second case is a 60-year-old woman diagnosed with osteoporosis due to a densitometry performed in January 2014 (bone mineral density at femoral neck: 0.550 g/cm2, T-score: −2.7), and treated with calcium, vitamin D and denosumab since then. In February 2015, densitometry was performed, and an increase in femoral neck bone mineral density of 14% was observed (bone mineral density: 0.627 g/cm2, T-score: −2) with respect to the densitometry performed one year before.
In October 2016, she presented opacification of both lenses (bilateral cataracts), a secondary effect described after the use of denosumab. 8 Thus, that drug was withdrawn. In December 2017, after a fall, she suffered a fracture of the left femur, which required surgical intervention.
In a densitometry performed in January 2017, about three months after denosumab suspension, a decrease in bone mineral density at the femoral neck of 5% (bone mineral density: 596 g/cm2; T-score: −2.2) was noted compared to the densitometry performed in 2015.
In March 2018, bone turnover markers were analysed and measured, showing a very high P1NP value (272.4 ng/mL). TRAP was also above normal (4.3 ng/mL) although the other markers, CTX and OC, were normal. PTH and vitamin D also showed normal values.
Case 3
The third case is a 74-year-old woman, self-employed and with no relevant medical history, diagnosed with osteoporosis in September 2016 after having densitometry (bone mineral density at femoral neck: 0.609 g/cm2; T-score: −2.2) and who had not presented previous fragility fractures. She was prescribed denosumab to commence on that same date. After the second dose, in March 2017, her dentist suspended antiresorptive treatment to carry out programed dental surgery afterwards. In April 2018, 13 months after the suspension, she suffered a fall from her height producing a subcapital fracture of the left femur, undergoing surgery to place a prosthesis.
Densitometry carried out in February 2019 showed a decrease of bone mineral density at the femoral neck of 6.7% (bone mineral density: 0.568 g/cm2; T-score: −2.5). An analysis performed then showed high levels of both P1NP (77.4 ng/mL) and beta-crosslaps (0.64 ng/mL). OC and TRAP were not measured. Both PTH and vitamin D showed normal values.
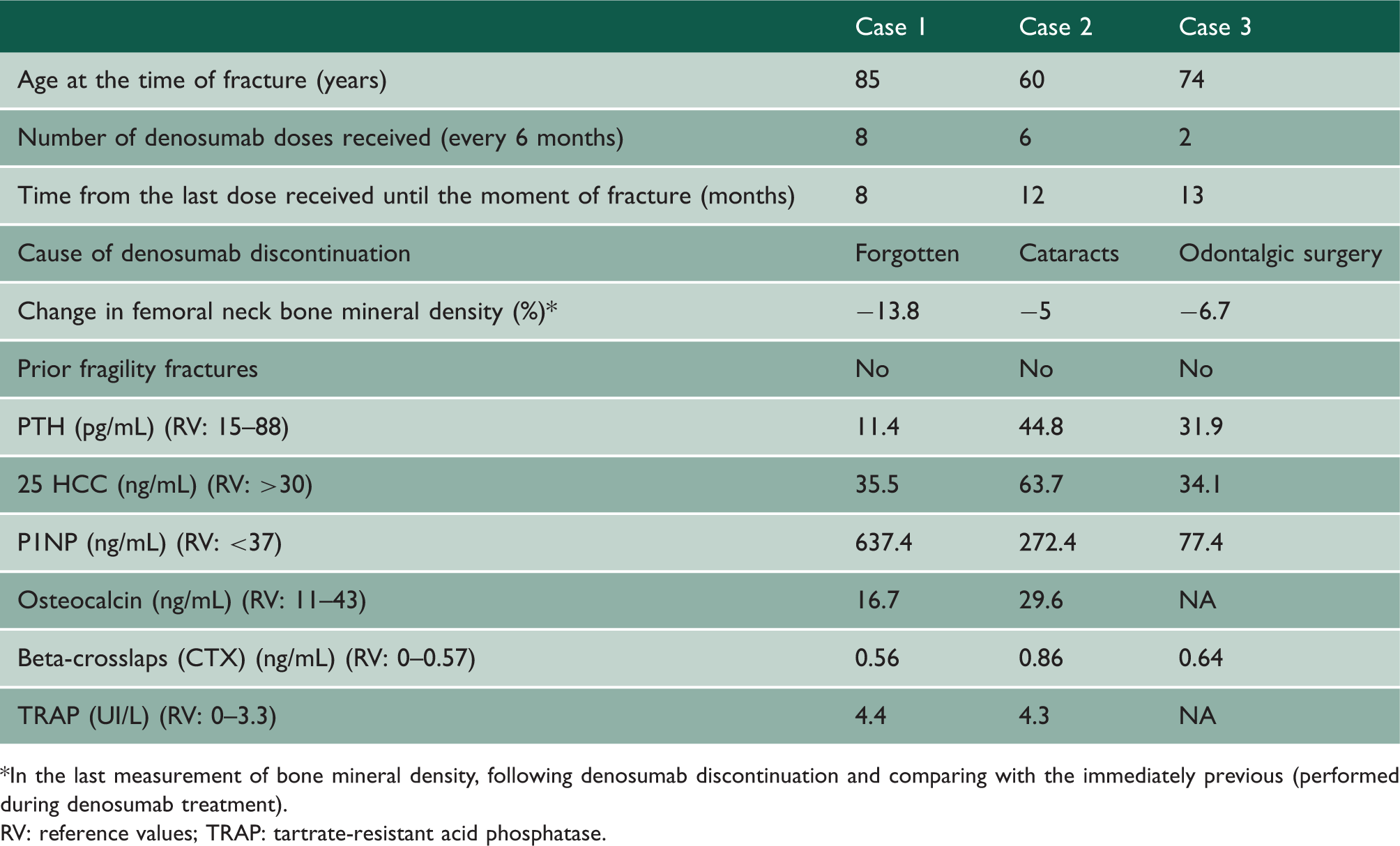
Table 1 shows clinical characteristics and biochemical data of all our patients and densitometry changes. Figure 1 shows femoral neck bone mineral density evolution of all the cases expressed as T-score. All bone mineral density measurements were performed in a densitometry Hologic QDR 4500 Discovery whose coefficients of variation are 1% at lumbar spine and 1.6% at femoral neck.
Femoral neck bone mineral density evolution in all the cases, expressed as T-score (before, during and after treatment with denosumab). Clinical characteristics, biochemical data and bone mineral density changes of the patients. *In the last measurement of bone mineral density, following denosumab discontinuation and comparing with the immediately previous (performed during denosumab treatment). RV: reference values; TRAP: tartrate-resistant acid phosphatase.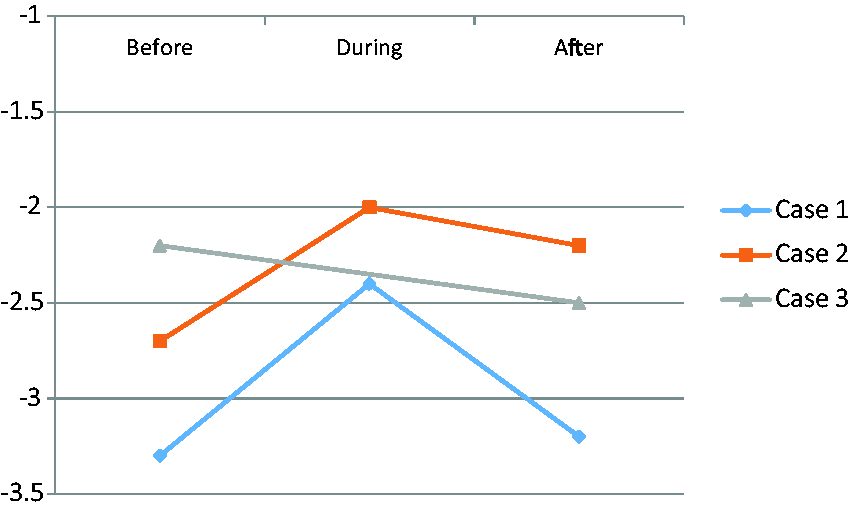
Discussion
A study by Modi et al. in 2017 reported that 48.8% of patients treated with denosumab discontinued the treatment in the first year and 64% in the second year. 9 Rapid and high changes in bone mineral density and bone turnover markers related to denosumab treatment and its discontinuation have been proved long time ago. 10 Biochemical data together with bone mineral density changes observed in our patients raise the suspicion that denosumab was the underlying cause of the fractures produced. The very high levels of P1NP indicate an exalted osteoblastic activity that could be a rebound effect produced when the drug is suspended: denosumab causes a powerful inhibition of RANKL that keeps the osteoclast activity low (almost nullified) and thereby a low bone resorption; when the drug is discontinued, osteoblasts may respond with increased activity to reactivate inhibited osteoclasts intensely, leading to an increased reabsorption that, hypothetically, weakens the bone, a hypothesis of rebound previously suggested by other authors. 5
In conclusion, we present the cases of three patients affected with osteoporosis without previous fragility fractures, who were receiving treatment with denosumab and who, after suspending the drug, suffered fragility hip fractures, a type of fracture that has not been described until now in this circumstance. We consider it of vital importance to carry out directed studies to verify the mechanisms by which this dramatic increase in bone fragility occurs after the discontinuation of denosumab treatment, in addition to the need to warn patients receiving the drug of the consequences of discontinuation.
Footnotes
Declarations
Acknowledgements
None.
Provenance
Not commissioned; peer-reviewed by Robin Ferner.