
Abstract

On 1 April 2019, the National Institute for Health and Care Excellence was 20 years old. This is an anniversary worth noting, if for no other reason than how remarkable it is for a National Health Service quango (quasi-autonomous non-governmental organisation) to be still standing two decades after its inception. There are more reasons for marking and celebrating the National Institute for Health and Care Excellence’s 20-year run. In the intervening years, the Institute has done much to advance the health of the UK population. It has achieved an international reputation for robust and fair healthcare prioritisation that is widely viewed as setting the global standard. The National Institute for Health and Care Excellence built this reputation not only through the rigorous development and application of scientific methods to guide its work but also through its efforts to articulate the underpinning social and ethical values that provide its decisions with robust justification. The National Institute for Health and Care Excellence’s reputation also rests on its commitment to transparency, accountability and inclusiveness in facilitating public and patient input in its deliberations.
From the start, the National Institute for Health and Care Excellence developed a distinctive approach to its work. The Institute took a robust view on the need to provide evidence for the value of healthcare interventions. In a publicly funded but cash-limited system, citizens (and politicians) needed to be assured that the National Health Service would only fund interventions that provided good value for money. Yet, the National Institute for Health and Care Excellence went beyond these generalities to specify how value for money would be assessed. The National Institute for Health and Care Excellence considered whether the opportunity costs of investing in new interventions could be justified by the health gains they could offer. A threshold was set – a range of £20,000 to £30,000 per additional quality-adjusted life-year – above which a new intervention would not normally be considered a ‘good buy’ for the National Health Service and rejected because its adoption would likely displace more health than it offered. As a way of publicly justifying its decision-making processes, the National Institute for Health and Care Excellence developed a statement of what it termed its ‘Social Value Judgements’ in 2005.
1
This document was updated in 2008, in response to the National Institute for Health and Care Excellence acquiring responsibilities for public health. Both editions focused on value for money as a foundational consideration for ensuring fairness to National Health Service patients in the context of limited resources. As a testimony to Social Value Judgements’ importance, the document was cited in the first judicial review of a National Institute for Health and Care Excellence decision: The key principle underlying NICE’s approach to appraisals is that the NHS’s limited resources should be targeted on those treatments which provide best value for money. The principle is to be found at paragraph 4.1 of NICE’s “Social Value Judgments – principles for the development of NICE Guidelines”. (8 December 2005)
2
Although the Social Value Judgements clearly conveyed the National Institute for Health and Care Excellence’s commitment to securing value for money, they also recognised the critical importance of other social and ethical values. Reducing health inequalities, preventing discrimination and addressing disabled people’s needs figured prominently in both Social Value Judgement documents. So, when the National Institute for Health and Care Excellence announced in November 2018 that it was updating Social Value Judgements, there was considerable interest in whether any changes would ensue – perhaps reflecting the increasing personalisation of medicine or how the National Institute for Health and Care Excellence was adapting to the addition of social care to its remit, within a global environment of healthcare austerity, scepticism of expertise and, of course, Brexit (the UK referendum decision to leave the European Union). 3
Comparison of social values in 3 editions of principles underpinning NICE Guidance.
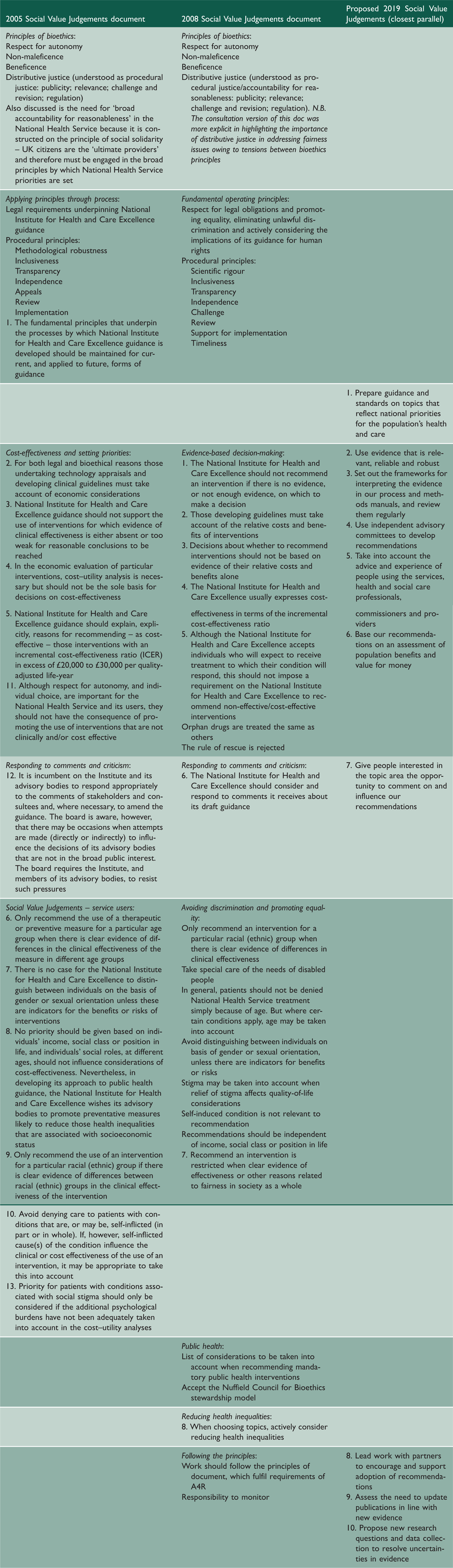
Both the 2005 and 2008 versions of Social Value Judgements begin with a discussion of the substantive bioethical and procedural operating principles which govern the National Institute for Health and Care Excellence decision-making. This is absent in the proposed revision. Substantive values present in the earlier versions – notably fairness, equality and respect for autonomy – have now dropped out altogether.
The National Institute for Health and Care Excellence’s rationale for this dramatic change is that all the values relevant to the National Institute for Health and Care Excellence are available in other documents. These documents include the National Institute for Health and Care Excellence Charter, its process and methods manuals, and legal and establishment materials – in total, many hundreds of pages whose content is, for the most part, highly technical. The National Institute for Health and Care Excellence’s social and ethical values may be implicit in these documents, but they are by no means explicit, and they certainly require interpretation. The National Institute for Health and Care Excellence also claims, questionably, that its values are ‘after almost 2 decades, well understood and accepted’. 3
This change raises two questions. First, what is lost when substantive ethical and social values, like those endorsed in both prior Social Value Judgements, are no longer explicitly put forward as guiding principles for the National Institute for Health and Care Excellence? Second, what is the impetus for and objective of this dramatic change – could it be heralding a shift in the way the National Institute for Health and Care Excellence thinks or works?
Considering the first question, the main casualties of this new approach are likely to be accountability, transparency, consistency, and public, political and professional understanding of the reasons for the National Institute for Health and Care Excellence’s decisions. The move away from substantive ethical values towards procedural principles enables the detail of decision-making procedures and the content of recommendations to remain almost entirely unspecified. Patients who are being denied treatment on the basis of the National Institute for Health and Care Excellence’s decisions will particularly struggle to make sense of their situation, as will clinicians who need to explain such decisions to them. Equally, the National Institute for Health and Care Excellence’s decisions are left open to a wide range of professional, financial, political and other interests without providing a basis for scrutinising them. For these reasons, the move towards procedural principles sends a worrying signal to other countries who are establishing priority-setting processes for Universal Health Coverage. Universal Health Coverage is about the values and principles that countries could embrace in expanding health benefits for their populations. With the proposed Social Value Judgements, the National Institute for Health and Care Excellence risks losing its status as a leading example from which others might learn how to combine procedural and substantive values in decision-making.
While goals such as reducing health inequalities are embedded in National Health Service legislation, to be meaningful and actually addressed, they must be enacted in the day-to-day functioning of the National Institute for Health and Care Excellence and other health and care organisations. Furthermore, although the historical divide between health and social care is becoming more blurred, this should not lead to an assumption that challenges in both areas are similar. Rather, analysis of the challenges and opportunities in the two areas working in a more integrated fashion is required. The National Institute for Health and Care Excellence has been responsible for developing social care guidance since 2013 but, according to the proposed Social Value Judgements, this does not seem to have prompted reconsideration of the way it might function in the future, even though a National Institute for Health and Care Excellence Citizens Council discussion in 2013 suggested there could be some differences, in emphasis at least, in the areas of dignity and respect for autonomy. 4 Applying a consistent set of principles to both sectors together with clearly identified research priorities for the National Institute for Health Research (NIHR) would enhance both the way the National Institute for Health and Care Excellence approaches these interrelated decisions and the availability of empirical data, especially relating to outcome measurement, valuation, costing and inequity reduction.
Other flagships of the National Institute for Health and Care Excellence’s methods, for example how ‘evidence’ is defined and assessed, are also given little attention. While its invocation of the use of ‘relevant, reliable and robust evidence’ seems uncontroversial, it says nothing about how the National Institute for Health and Care Excellence will approach the contestable nature of the interpretation of these attributes. Simply signposting interested parties to the technical and process manuals might be considered efficient, but it is analogous to inviting people to read the New Testament in order to identify key Christian values.
With regard to the second question – what is the impetus for and objective of this dramatic change in guiding principles for the National Institute for Health and Care Excellence? – the Institute is no longer the dominant provider of National Health Service guidance – National Health Service England is increasingly issuing clinical guidance either directly or in collaboration with the National Institute for Health and Care Excellence, for example, in the case of the Cancer Drugs Fund. 5 Public health guidance is now frequently developed by Public Health England. Within this crowded space, there are hints that the National Institute for Health and Care Excellence’s methodology is changing to accommodate broader goals. 6 The previous emphasis on cost-effectiveness as a social and ethical value and the use of an explicit cost-effectiveness threshold are watered down to the somewhat inexact ‘assessment of population benefits and value for money’ (Principle 6 in the new document). This vagueness may be mere drafting for a general audience or it could represent a drift towards greater managerial discretion and control. Specifically, this could reflect a weakening of the application of the threshold – either upwards to the benefit of industry or downwards for the sake of expenditure control. Both have consequences for the fair distribution of people’s health. 7
So what is the way forward? The National Institute for Health and Care Excellence has a responsibility not only to ensure that its social and ethical values are explicit and aligned with the goals of the National Health Service, public health and social care,8,9 but how they are made a day-to-day reality. This new document does little to achieve this: it would be better to withdraw it and start work on a thorough revision of Social Value Judgements. Alternatively, the National Institute for Health and Care Excellence published a Charter in 2017 10 that has a short section on social and ethical values. This could be expanded.
As a group of observers and admirers of the National Institute for Health and Care Excellence, we are disappointed that the proposed Social Value Judgements document departs from many of the values that made the National Institute for Health and Care Excellence such an innovative and widely admired organisation. The National Institute for Health and Care Excellence and the National Health Service are currently under immense pressure, but now is not the time for retreat from substantive values. This is the time for the National Institute for Health and Care Excellence to reaffirm these values and seize again its global leadership role as an institution that brings accountability, transparency and legitimacy to decisions that are among the most ethically and politically challenging in any society.
Footnotes
Declarations
Acknowledgements
The views expressed are those of the authors and not necessarily those of the National Health Service, the NIHR or the Department of Health and Social Care. This work was completed as part of Annette Rid’s official duties as an employee of the NIH Clinical Centre. However, the opinions expressed are the authors’ own. They do not represent any position or policy of the National Institutes of Health, Public Health Service or Department of Health and Human Services.
Provenance
Not commissioned; editorial review.