
Abstract
Primary care services in England may be reaching saturation point. Demands to see a general practitioner or practice nurse have increased substantially. Clinical complexity has also increased; patients are living longer, but with more multimorbidity. 1 These demands are mirrored by a decline in the General Practice workforce, despite political pledges to reverse this. 2
New strategies are needed to tackle the current pressures in general practice and reduce the risks of harm to patients. The NHS England GP Forward View advocates investing and developing new models of care, including expansion of a multidisciplinary, integrated primary care team. 3 These recommendations reflect the findings of the Primary Care Workforce Commission, who highlighted the potential roles for clinical pharmacists, physician associates, healthcare assistants and physiotherapists, which many general practices are now making greater use of.4–6
The Commission also recommended that general practices should consider more opportunities to use the skills of paramedics in primary care. Specific roles may include running clinics, triaging and managing minor illnesses, as well as provide continuity for patients with complex health needs. Further roles may include assessment and management of requests for same-day urgent home visits, as well as regular visits to homebound patients with long-term conditions. The commission highlighted that these innovative roles should be subject to further evaluation. Nevertheless, historical and current perspectives allow us to model how the role could be fully used.
Paramedics as primary-care generalists
Paramedics have a track record in providing flexible and innovative ways of delivering extended clinical care. Such developments have predominantly centred around enhancing practice in the ambulance service, such as using specialist paramedics to attend to patients calling 999 with apparent minor injuries or illness following call-taker triage. But innovations by paramedics are increasingly being recognised in other arenas. This is partly because of the expectation that a paramedic can provide generalist care as an autonomous allied healthcare professional, for which several advantageous have been identified, including reduced conveyance to emergency departments, increased patient satisfaction with paramedic care and efficiency benefits. 7
Paramedic skill mix.

Adapted from Post-Reg Career Framework. 10
Other names for this group of paramedics have emerged through different healthcare providers; they include emergency care practitioner, community paramedic, enhanced paramedic, paramedic practitioner and specialist practitioner. We adopt the term Specialist Paramedic, as advocated by the College of Paramedics.
The generalist skill mix of the modern day paramedic creates possibilities for them to work in a range of domains. Primary care is one domain in which additional capacity is desperately needed. Both specialist and advanced paramedics can work in primary care with differing degrees of autonomy, decision-making and treatment options within their scope of practice. Early review pointed to paramedics being deployed into primary care roles that included centralised telephone triage, on-scene acute care delivery and intermediate community care support schemes. 11 However, there is now growing recognition that the generalist skills of the paramedic should be deployed into in-hours general practices.
Current and future implementation
The General Practice Forward View made a commitment to grow the wider workforce in general practice by a minimum of 5000 staff. However, there was no formal requirement that this workforce should include paramedics. Although absolute numbers remain small, between September 2016 and March 2017, the number of paramedics working in general practice doubled, increasing from 75 to 150. 12
The NHS England GP Access Fund (formerly the Prime Minister's Challenge Fund) served as a platform to test, and to some degree, evaluate how paramedics can be deployed in primary care. The scheme was specifically introduced to help improve access to general practice and increase innovation in primary care. The first evaluation report highlighted at least four sites, among the 20 awarded funding, who piloted a range of models in primary care working with the ambulance service and paramedics. 13 In the South Kent Coast, specialist paramedics provided home visit support and dispensed some acute medications to community-based patients. The service reportedly saved 720 general practitioner appointments. In Workington, Specialist Paramedics were deployed into Accident & Emergency departments to determine whether patients could have been more appropriately treated in a Primary Care Centre.
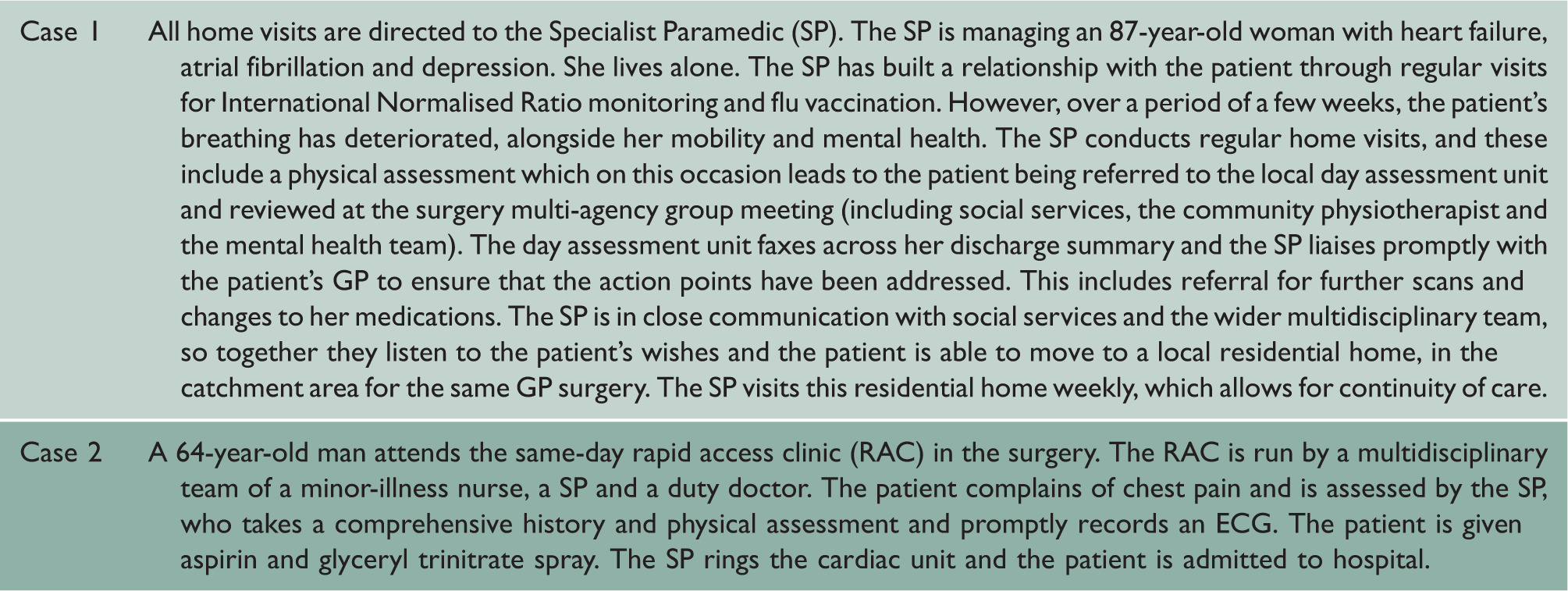
Case studies of care provided by paramedics in general practice.
Conclusions
The NHS GP Forward View and the Primary Care Workforce Commission have both recommended the development of a multidisciplinary primary workforce that includes general practice-based paramedics. The NHS has already had a positive public response to proposals to introduce independent prescribing by paramedics, facilitating new roles in primary care. 14 However, the empirical evidence base to support these roles is currently weak, and implementation is largely based on innovative case studies. The current opportunities for employment in NHS general practices still require careful evaluation for context-specific clinical outcomes, value and satisfaction. 15 Empirical data from other countries, e.g. North America, may not be directly transferable to England due to contrasting healthcare systems. There will also need to be a significant expansion in the overall number of paramedics for there to be real impact on NHS primary care. This potential expansion would need to be considered in the context of any impact on current ambulance services. Nevertheless, the scene is set for the general practice paramedic, a setting that is desperate for extra capacity, and integrated multidisciplinary teams of the future.