
Abstract
As the English National Health Service (NHS) approaches its 70th year, its founding principles of universal coverage and being free at the point of access may be challenging to sustain. These principles are now under threat. The NHS is experiencing its deepest ever budget crunch. Under current spending plans, annual real-term growth will average 1% this decade; this is compared to a historical growth of 4%.
1
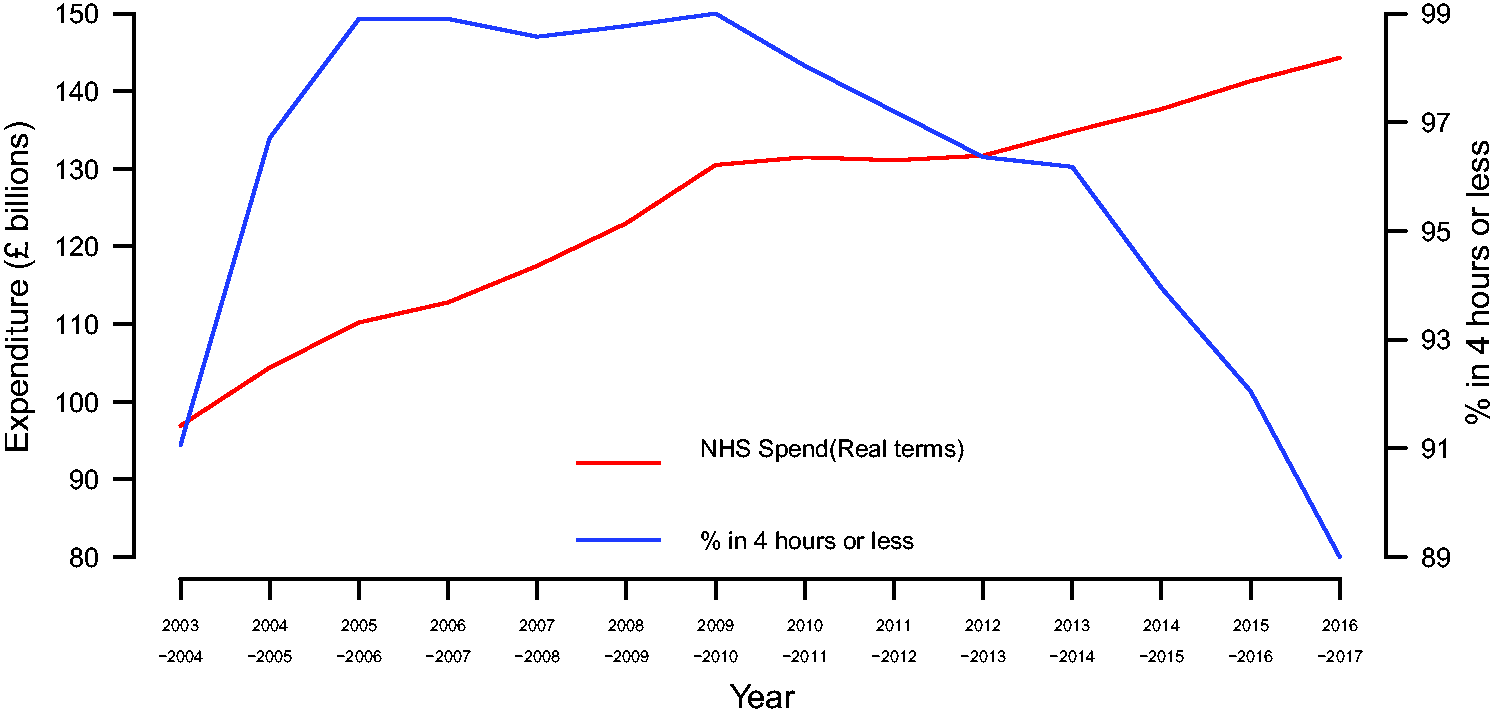
The system is concurrently facing unprecedented pressure (Figure 1), due to England’s ageing, growing population, with more long-term-conditions, and more expensive treatments. These demands are increasing costs by 4% annually.
2
The result has been record deficits and performance deterioration. In 2015/2016, 80% of England's acute hospitals were in financial deficit, compared with 5% three years ago, while the number of patients being seen outside of A&E waiting-time targets increased (Figure 2). Further, long waits for emergency admission, ‘trolley waits’, increased by 45% in 2016/2017.
3
The waiting list for elective surgery has increased by 5% in the last year (now 3.78 million) and delayed discharges from hospital due to waits for home care increased by 45% over the same period.
3
This ‘crisis’ occurs in the context of relatively low funding when compared with other Western European nations; international figures speak for themselves, with the UK committing 9.7% of its GDP to health, whereas Germany spends 11.3%, Switzerland 12.4%, France 11.0% and the Netherlands 12.9%.
4
NHS spending and A&E attendances 2003/2004–2016/2017. NHS spending and A&E waiting times (percentage meeting 4-h target) 2003/2004–2016/2017.
Many raise the question of what options exist for funding the health system going forward. 5 NHS funding and its consequential performance oscillate between scarcity and abundance. The former triggers the latter, with unpalatable system performance leading to sharp political intervention, as was the case in 1951, 1968, 1976, 1987–1988 and 1999. Given our current trajectory, NHS performance will likely be sufficiently attenuated in coming years, possibly following last years’ election, to necessitate significant intervention. This analysis aims to discuss the most viable options to consider, while noting that several others exist. We see three broad themes for managing funding in the short term: a managed deterioration; additional public funding from increased taxation or reallocation; and increased private funding from individuals and businesses.
‘No money’: managed deterioration
Justifying additional NHS funding is complex.It consumes more of the government’s budget than any other public service and since the economic crisis has received the largest increases of any department. Amid finite resources, further investments in the NHS may entail funding reductions of other public services; this can be difficult to negotiate.
There is rising demand for healthcare with greater numbers of chronically ill and elderly patients with increased utilisation and referrals from primary care. 6 This is in the context of a decrease in the National Tariff Payment System. 7 Should there be no long-term commitment to additional NHS funding, it seems unlikely that the NHS will sustainably halt erosions in performance let alone reverse them. In this scenario, the £22 billion of efficiency savings outlined in the Five Year Forward View will need to be delivered by 2020 to maintain sustainability. 8 The NHS was challenged to make £20bn of efficiency savings between 2010 and 2015 and £5.8 billion was saved between 2011 and 2012. 9 However, it is unclear and unlikely that all of the remaining £20 billion in savings were achieved by 2015. 10 This would suggest that significant additional efficiency gains without appropriate infrastructure investments will be challenging, especially given current pressures. If trusts are to instead meet targets, they will be required to make a 4.3% reduction in operating costs and receive £1.8 billion in additional funding. 11 If temporary funding is excluded, NHS providers recorded a deficit of £4.3 billion and £3.7 billion in the years 2015/2016 and 2016/2017, respectively. 11 Rationalisation may fast become rationing: in 2016, Chris Hopson, Chief Executive of NHS Providers, said that without urgent funding, hospitals will either have to cut staff, introduce charges or implement ‘draconian rationing’. This is evidenced by NHS Clinical Commissioning Groups who have imposed additional criteria for elective surgery, including delaying procedures for smokers. 12 The difference between rationalisation and rationing is a grey line, but if Clinical Commissioning Groups instigate additional barriers to effective treatments for the purpose of saving costs, then, arguably, this could represent rationing.
Looking forward, these health system changes could be managed actively or passively: planned rationing could take place with greater restrictions over services. Alternatively, performance changes could occur passively, as occurred in the early 1990s where waiting times gradually extended and public satisfaction decreased leading patients to seek care elsewhere. 13
‘Public Money' - Additional public funding
Our current trajectory mirrors past experiences when the NHS has suffered prolonged capital constraint. Public dissatisfaction will serve as a powerful motivator for political intervention – the questions that remain are when and in what form. There are several avenues for additional public financing, some of which have been used previously. For example, in 2001, the government committed to a 35% real-term rise in NHS funding, partly financed by increasing National Insurance. 14 While a similarly large settlement is unlikely, a long-term package to stabilise the NHS could be possible.
Reallocation of funds
The first option is reallocation of current funds from other government departments. For the aforementioned reasons, this can be difficult to negotiate, but could be eased by increasing general taxation.
An option creating better alignment between the source and spend of health funding is the pension ‘triple lock’. Seniors consume up to half of NHS resources. The triple lock was introduced by government in 2010, providing a guarantee to increase the state pension annually by the higher of inflation, average earnings or 2.5%. It is not irrelevant that a higher proportion of pensioners vote compared to other age groups. At present, the triple lock costs approximately £6 billion a year. There is some consensus that this guarantee is not sustainable. Moving from a triple to a double/single lock could release expenditure for diversion with, for example, a guarantee over social care funding. A previous report addresses this subject in more detail arguing that if pensions were instead uprated in line with incomes, this would provide a 1% saving of GDP by 2060. These savings may provide funds for a more generous uprating of public spending in health and social care. 15 It is also of note that, on average, pensioners may no longer be the poorest members of society. 16 Changes to pensions, however, would be politically divisive and may have limited financial impact on health system funding.
Raising National Insurance or a hypothecated tax
There appears to be growing public support for increased taxation for the purposes of funding healthcare. A YouGov survey indicated that the public would be in support of increasing basic income tax from 20% to 21%. 17 This is supported by the recent British Social Attitudes Survey providing evidence that the government has space to increase taxation. 18 Alternatively, National Insurance could be raised. Currently, British taxation is divided into income tax and a National Insurance tax. National Insurance contributions are also paid by employers and are theoretically ring-fenced for use to fund the NHS, unemployment benefits, sickness and disability allowance, and state pensions. However, the government is able to borrow from National Insurance and it is broadly perceived to be part of general taxation. A poll showed that 48% of the public would support an increase in National Insurance directed towards the NHS, compared with 34% for an increase in the basic rate of tax. 19 An increase of 1 p in taxation on all income to be collected for the purpose of funding the NHS has been suggested by many different politicians and featured in the manifesto of the Liberal Democrats. However, there are concerns; National Insurance applies to employees and employers and its use to fund health may disproportionately shift this burden onto the working population, even though the largest portion of health resource is spent on older people. Another disadvantage of increasing National Insurance is that it is currently not separated from general taxation and it can be difficult to openly determine how much of it is directed towards the NHS.
Extrapolating this, Norman Lamb, former Minister of State for Care, proposed a hypothecated tax: a conversion of National Insurance contributions into a separate tax earmarked for funding health and social care. As argued by Julian Le Grand, hypothecated taxes can draw public support due to their transparency – stated plainly, the electorate knows what they are paying for. 20 Her Majesty's Treasury has been resistant to hypothecated taxes – compared to general taxation they entail higher transaction costs, a smaller base of payers and preclude more flexible allocation of funds. Further, funding from a hypothecated tax would be likely unpredictable and when directly asked in the British Social Attitudes survey in 2015, only 24% supported a dedicated NHS tax. 21 Recently however, there have been a number of calls from senior politicians for the introduction of an 'NHS' tax, which could coincide with the NHS' 70th birthday. 33 A more detailed discussion of a hypothecated tax for the NHS is discussed elsewhere. 22
Localised funding
Local funding options also exist. There is growing realisation that in healthcare, one size does not fit all. As demonstrated by the sustainability and transformation planning process, local health economies vary in their requirements – from the case-mix they serve to the state of their health services. The ability for health economies to have their own funding mechanisms permits local need, funding and delivery to be better aligned. In 2015, the Chancellor introduced the capability for councils to raise taxes by up to 2% to increase funding of social care. Similar local mechanisms for raising capital for NHS systems could be created. In Sweden, for example, county councils and municipalities are able to set user-fees and co-payments on healthcare services, in accordance with the volume of capital generation needed. 23 NHS England is exploring the possibility of local areas retaining the proceeds from selling surplus land to invest in new services. This could be property from NHS trusts or, alternatively, could be garnered from groups of general practices aiming to consolidate to a single centre, with the remaining land being sold to finance development. Selling assets to raise cash, however, can only be conducted once, rather than serving as a long-term solution. A crucial limitation of a localised funding approach is the variability in local governments’ ability to raise funding. Further, it is often the case that areas which need funding the most have the least ability to raise funds.
‘Private money’: co-payments and health insurance
Co-payments
Over half of Organisation for Economic Co-operation and Development nations require payments for visiting a general practitioner or for hospital services. NHS patients pay for optical and dental treatment, lending scope to expand services financed this way. These could be selected actively in a national process, based on need, utilisation or cost-effectiveness; or it could occur passively. Mini-markets are forming due to supply–demand mismatches, as with physiotherapy and osteopathy, where in some localities tighter eligibility criteria lead patients to seek care elsewhere and pay out-of-pocket. 24
Several commentators have proposed charging for general practitioner appointments or DNAs (‘did not attend’). This generates revenue while altering behaviour – reducing demands on primary care by dissuading less urgent cases to attend, or disincentivising missed appointments. 25 A number of European countries already implement general practitioner charges, ranging from 85 pence in France to £17 in Sweden per appointment. There are around 300 million consultations in primary care a year, two-thirds of which are with a doctor. 26 A £10 charge with no exemptions could raise £2 billion before administrative costs. 26 Figures have also suggested that more than 12 million GP appointments and 7 million outpatient hospital appointments are missed each year in the UK. 27 A 2013 survey found the majority of surveyed general practitioners supported charging a small fee for appointments. 28 Charges, however, challenge the progressive nature of NHS funding, limiting access, discouraging people in seeking prompt medical attention, leading to later-stage intervention and possibly higher costs, in addition to penalising patients with multiple long-term conditions who require more frequent appointments. 25 A systematic review indicates that a strategy of co-payments does not reduce inappropriate hospitalisation and further reduces use of effective treatments as much as ineffective treatments. 29 Further, the effects were disproportionate on individuals and families with low incomes particularly in reducing healthcare utilisation among low income children. 29 The administrative cost of a co-payment strategy is also significant, particularly if equity is to be maintained. Politically, this veers on the less palatable while entailing significant administrative burdens.
For some of the population, prescriptions already entail charges. Around 1 billion are dispensed annually in the NHS, with only 9.4% being paid for, generating around £450 million revenue. 30 This low proportion is due to exemptions that apply to the over 60s, children and those with specified medical conditions, i.e. the heaviest users of prescription medicines. As identified in the Barker review, if exemptions were removed, and the charge of all prescriptions decreased to £2.50, this could raise around £2 billion annually, and £1 billion more for every additional £1 charged per prescription. 31
Incentivising private health insurance
An alternative would be to incentivise private health insurance uptake, such as via a tax relief. This was considered by Margaret Thatcher’s government, in particular for over-65s to reduce NHS waiting times. In Australia, means-tested tax rebates exist for private health insurance cover, with tax-based incentives and disincentives that shift high earners from the public to private system. While this can relieve pressures on public services, it risks creating a ‘poor service for the poor’. Detracting populations from the NHS may destabilise its pooling and economies of scale, with for-profit insurers recruiting wealthier and healthier patients. Further, an analysis by the Institute for Fiscal Studies has suggested that the subsidy would be most beneficial to individuals who already have insurance and the savings from a decrease in NHS demands resulting from such a subsidy would be insufficient to cover the cost of such a policy. 32
Conclusions
The NHS is experiencing its greatest mismatch of operational demand and funding supply. Several options exist for instilling financial stability. As public dissatisfaction increases, it seems a matter of time until political intervention occurs, or public expectations recalibrate. Opponents to the current government have argued that austerity is a choice, and there have been calls from both sides for a softening of the cuts to public services. However, with Brexit set to dominate British politics for the foreseeable future, and its predicted economic implications, the NHS may fail to become a political priority in the short term.
The most feasible avenue could be a combination: an increase in NHS productivity with a more constrained spectrum of services; combined with increased taxation or potentially a hypothecated tax. These interventions must be accompanied by regular assessments of England’s health and care needs, as seen with the Five Year Forward View. 8 Former Health Ministers have called for a cross-party commission to review health and care; this is likely the clearest next step in robustly determining the future of our health system’s funding.
Footnotes
Declarations
Acknowledgements
None
Provenance
Not commissioned; peer-reviewed by Nigel Edwards.