
Abstract
Objectives
To describe serious incidents occurring in the management of patient remains after their death.
Design
Incidents occurring after patient deaths were analysed using content analysis to determine what happened, why it happened and the outcome.
Setting
The Strategic Executive Information System database of serious incidents requiring investigation occurring in the National Health Service in England.
Participants
All cases describing an incident that occurred following death, regardless of the age of the patient.
Main outcome measures
The nature of the incident, the underlying cause or causes of the incident and the outcome of the incident.
Results
One hundred and thirty-two incidents were analysed; these related to the storage, management or disposal of deceased patient remains. Fifty-four incidents concerned problems with the storage of bodies or body parts. Forty-three incidents concerned problems with the management of bodies, including 25 errors in postmortem examination, or postmortems on the wrong body. Thirty-one incidents related to the disposal of bodies, 25 bodies were released from the mortuary to undertakers in error; of these, nine were buried or cremated by the wrong family. The reported underlying causes were similar to those known to be associated with safety incidents occurring before death and included weaknesses in or failures to follow protocol and procedure, poor communication and informal working practices.
Conclusions
Serious incidents in the management of deceased patient remains have significant implications for families, hospitals and the health service more broadly. Safe mortuary care may be improved by applying lessons learned from existing patient safety work.
Introduction
Hospitals have a clear responsibility to ensure the safety of the patients that they care for 1 and this duty of care continues even after death.2,3 Strictly speaking, a dead person cannot be harmed but civilised society expects that, after death, someone’s body will be accorded the same dignity and respect as during life. In the United Kingdom, the societal mores that guide such expectations have led to public anger when it was judged that healthcare institutions have failed to respect the dead. Prominent examples of this are the removal and retention of children’s organs at Alder Hey Hospital in Liverpool, keeping patients’ brains in Manchester and the storage of bodies on the floor of a hospital chapel in Bedford.4–6 Indeed, mistreatment of bodies has been given media coverage equal to, or greater than, harm before death in some instances.7,8 When discovered, these events have led to extensive enquiries and even changes to the law.2,4,5,9
Patient safety research studies have demonstrated that the burden of harm caused by unsafe care is substantial.10,11 Much work has been done in the field of healthcare to improve patient safety, including attempts to learn from reports of safety incidents to re-engineer and improve systems. 12 The prevention of incidents following death has, by contrast, received little or no attention in the scientific literature. We could find no published systematic study of errors following death, their impact, underlying causes and potential remedies.
We used a large national database of serious incidents to identify those that occurred after the death of a patient and determine what happened, underlying causes and the outcomes, using the WHO International Classification for Patient Safety (WHO ICPS) 13 to provide a conceptual framework, as has been used previously in both primary and secondary level care to characterise safety incidents.14,15
Methods
Since 2002, hospitals and other NHS organisations in England have been required to record, report and investigate any serious incident requiring investigation (SIRI). These are defined as
– Unexpected or avoidable death of patients, staff, visitors or members of the public – Serious harm to patients, staff, visitors or members of the public – A scenario that prevents or threatens to prevent a provider organisation's ability to continue to deliver healthcare services – Allegations of abuse – Adverse media coverage or public concern about the organisation or the wider NHS
The resulting database, the Strategic Executive Information System (STEIS), is the source of our study population. It had accumulated over 120,000 reports of serious incidents by April 2014. The system is separate from the more widely researched National Reporting and Learning System (NRLS). The latter database records incidents of lower degrees of harm (as well as serious harm) and is therefore a larger repository of incidents. It has been extensively used to study the nature of harm reported from frontline patient care.14,17,18 The STEIS system has the advantage that reporting of serious incidents is a requirement placed on all providers of NHS care by NHS headquarters. Also, the reporting organisation is required to formally investigate, account for what happened and set out action taken as a result.
Each recorded incident contains categorical information and free-text commentary. The categorical information (some captured through drop-down menus) covers the administrative data, the care sector and clinical area involved, the location of the incident, the basic demographic data of the patient involved and the type of incident. Free-text fields completed at the time of initially reporting the incident record information on what occurred, what immediate action was taken and a summary of the case. The reporting organisation is later required to complete further free-text fields detailing the investigation carried out, root causes identified and lessons learned following the incident.
We interrogated the database in October 2014. The process by which reports are compiled in STEIS means that it can be many months, often over a year, before the full details of an incident are available. To ensure completeness of reports analysed, the period studied included incidents occurring between 1 April 2002 and 31 March 2013. Incident reports where the field ‘location of incident’ was entered as ‘Mortuary’, the field ‘clinical area’ was entered as ‘Histopathology’ or ‘General pathology’ and/or the field ‘incident type’ was entered as ‘Post mortem’ were extracted and the full reports independently scrutinised by two authors to ensure they met the following inclusion and exclusion criteria: only incidents involving bodies or body parts (regardless of age or completed gestation) were included. Incidents not relating to a deceased patient or involving events before death were excluded.
The categorical data were used to provide contextual variables while the free-text information within the incident report was subjected to content analysis. Content analysis 19 was used to deconstruct the narrative content included in reports into a series of codes which represent and retain the meaning of the report in order to identify, for each incident, three major concepts from WHO ICPS: the type of incident (what happened); contributory factors (the circumstances, actions or influences that led to the incident) and the outcome. An inductive approach was taken whereby all reports were repeatedly read and reread to familiarise the researchers with the data. During this familiarisation process, open coding was performed and themes present in the data noted. These themes were then collated into a coding framework that was applied to all reports. New codes were added in an iterative manner and the new framework reapplied to previous cases to ensure the consistency and completeness of the analysis. At the conclusion of the analysis, each report was allocated a single code to describe the type of incident, and either none, one or multiple contributory factors. Reports were grouped by outcome and reread to identify themes common to these groups and potential learning opportunities from the incidents reported.
Results
Outcome of the incidents by incident type (PM, postmortem examination) N = 128 as four incidents were not coded with an outcome.
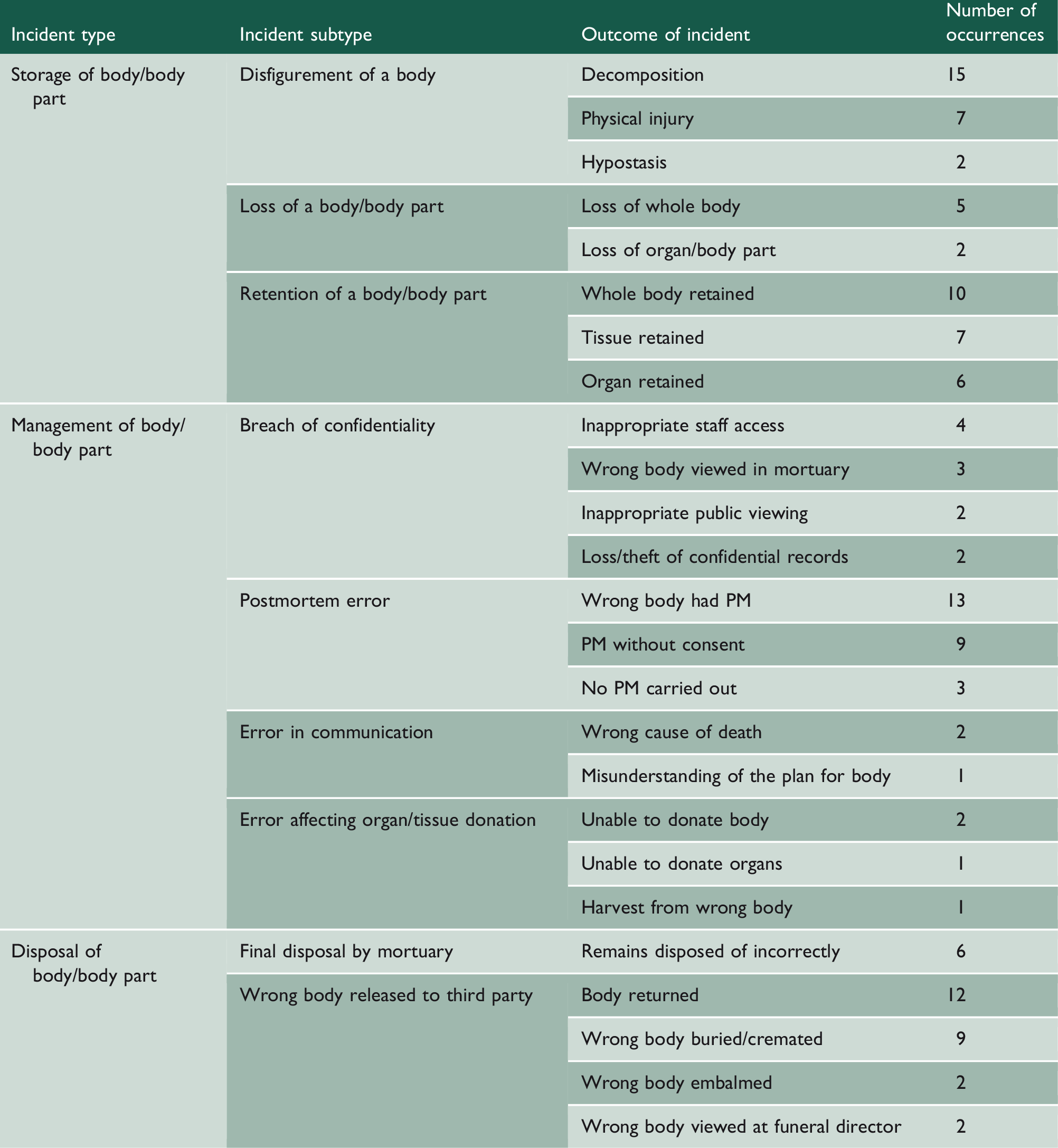
Outcome of the incidents
Storage
Incidents were grouped under the theme ‘Storage’ where they involved a failure to look after remains in the custody of the mortuary. This included physical damage to bodies and failures to monitor storage leading to the loss, or inadvertent retention, of bodies or body parts.
Disfiguring of bodies was the adverse outcome described in 24 incident reports. For example: ‘Patient’s body was not refrigerated over weekend rendering body unsuitable for viewing by relatives.’ Decomposition resulting from storing bodies for too long or at too high a temperature was the commonest reported cause, occurring in 15 incidents. In two, the bodies decomposed before postmortem examination, and in the third, the coroner ordered a second postmortem that could not be undertaken due to the state of the body. The other cases of decomposition caused distress to bereaved relatives; they were either unable to view the body or saw it in a mutilated state. Seven reports described bodies that were disfigured due to being accidentally dropped or struck while being moved around the mortuary. Two reports of disfigurement were caused by hypostasis from incorrect storage.
Ten incident reports concerned bodies wrongly kept in the mortuary for longer than intended. These were mainly fetuses but two were adults with no known next of kin. Where there was a family connected to the body, they were unaware that their relative’s remains were still in the mortuary. This was because the family had received and disposed of what they understood were the complete remains but were later told there was further tissue (e.g. the placenta being released instead of the body in the case of neonatal deaths).
In all, 13 incident reports involved retained tissue. The incidents then necessitated contacting families and releasing further body parts. None of the incident reports suggested that the retention of tissue had been intentional. All had occurred due to separation of the organs or tissue from the rest of the body for storage and then a failure to reunite these at the point of disposal.
Management
Incidents were grouped under the theme ‘Management’ where the required actions to be undertaken on a body were either not carried out or carried out in a substandard manner.
In 25 cases, the incident occurred during postmortem examination. For example: [A postmortem was commenced] It was quickly recognised that the early findings were not compatible with the history. The identity of the body was re-checked and it was then apparent that the body had been misidentified and removed from the refrigerator in error.
Four incidents related to the donation of organs or bodies following death. One patient wished to donate corneas and two patients intended to donate their whole bodies to medical science but this was not possible due to mismanagement of their bodies. In the fourth case, corneas were harvested from the wrong body.
Disposal
Incidents were grouped under the theme ‘Disposal’ where the outcome involved the way that the body left the mortuary. In 25 cases, the wrong body was released to the undertaker and in nine of them the body was cremated or buried, necessitating exhumation and a further funeral. For two families, the mistake was discovered when they were shown the wrong body at the funeral director’s premises. A further two bodies were embalmed but not viewed before rectification. In the remaining 12 cases, the mistake was noticed before either viewing or a funeral and the deceased was exchanged for the correct body.
The mortuary disposed of six bodies incorrectly. All were fetuses where the parents’ requested means of disposal was not carried out. This was either cremation rather than burial or vice versa, or that the remains were disposed of without the parents being made aware, preventing them from attending.
Reaction of relatives
Although not coded as an outcome of incidents, 74 of the reports referred to the reaction of the next of kin to these adverse outcomes. Commonly used descriptions were ‘emotional upset’ and ‘devastated’. In almost all incidents reports, the hospital authorities were recorded as having informed the family of the deceased of the incident. In the remaining few reports, it was not clear if the family were informed.
Contributory causes
Contributory factors identified in incident reports; each incident could have none, one or several contributory factors.
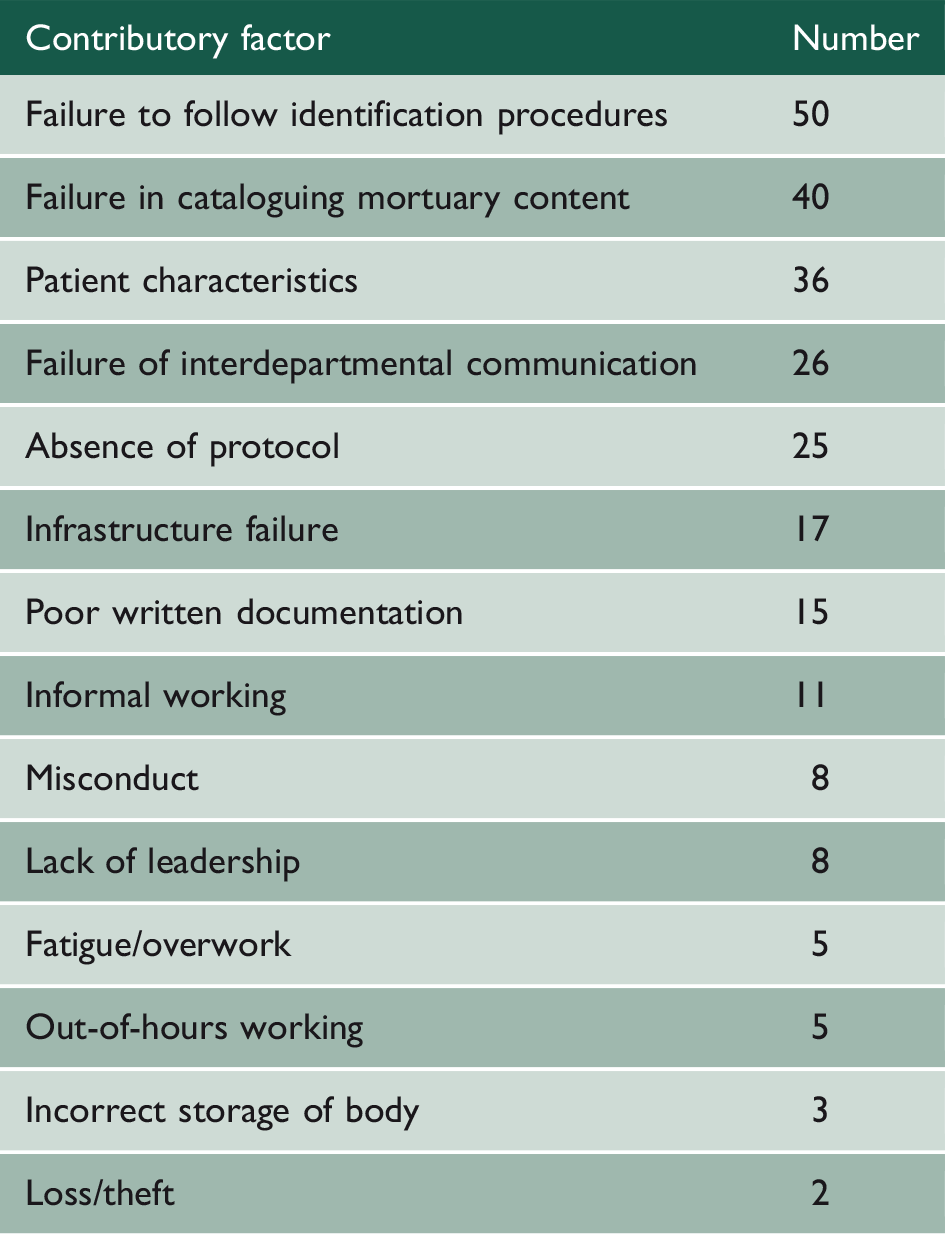
Misidentification
As might be expected, the commonest contributory factor (n = 50) was failure to follow standard identification procedures. In these incidents, the reports stated that a protocol for identification of bodies was in place but it had not been followed. For example: It was common practice for one member of staff to check the paperwork and one to check the patient, and at no time did either check the other as per instructions in the protocol. Both deceased had names in common.
In 25 reports, absent or inadequate standard operating procedures or protocols were described. For example: ‘The root cause was identified as an absence of a robust system to ensure that consent forms are checked thoroughly at the start of each postmortem investigation.’ These shortcomings resulted in postmortem examinations not being carried out, bodies being retained for prolonged periods and bodies being disposed of incorrectly. Weak identification protocols were mentioned in several reports, including those only requiring one member of staff to check a body’s identity, or relying on just one patient identifier (usually their name) instead of the two or three (name plus date of birth and hospital number or address) that is standard in clinical practice. Other descriptions in incident reports of absent standard operating procedures included a lack of instructions to staff on actions to be taken on discovering refrigerator failure out of hours, rules for allowing viewings of a body and the process to be adopted when an obese body will not fit in the refrigerator.
Failures in cataloguing mortuary content were described in 40 reports. This was most commonly a failure to link bodies with body parts that were stored separately. This led either to the body being released while organs were retained inappropriately or only body parts being released, while the body remained in the mortuary. Other failures of cataloguing procedures caused processing delays with bodies retained for unacceptable periods of time.
Infrastructure failure
Infrastructure failures were responsible for 17 incidents, 14 of which involved refrigerator malfunction. In three, there was no adverse outcome as alarm systems were triggered and remedial action taken. The other 11 led to decomposition of bodies. The remaining three infrastructure failures were of equipment used to move bodies, causing damage to the body.
Miscommunication
Twenty-six incidents were underlain by failures in communication between the mortuary and other departments. Handover between the maternity department and the mortuary for fetal remains was the interdepartmental relationship mentioned most frequently. One report noted that 12 possibilities were routinely considered when deciding on the handling of the fetus following intrauterine death, depending on gestational age and parental choices. Failure in the communication of these options and the lack of a standard operating procedure for handovers between the two departments contributed to all seven cases of incorrect disposal of remains. Errors in communication with the coroner contributed to a further seven cases, leading to postmortem examinations being carried out incorrectly.
Poor written documentation was an element of causation in 15 incidents. This included consent for postmortem examinations or disposal being incomplete or filed incorrectly, findings of postmortem examinations being recorded inaccurately or late and decisions or information arrived at during telephone conversations with other departments (including the Coroner’s Office) not being recorded. These underlying factors resulted in postmortems not being carried or being undertaken without consent.
Misconduct and informality of practice
Misconduct of staff was the direct cause of seven confidentiality incidents where hospital workers accessed bodies in an inappropriate and unauthorised manner. There was also an isolated case of theft from bodies by mortuary staff.
The negative influence of informal working practices within the mortuary was evident in 11 reports. For example: ‘The undertaker should have been accompanied and supervised at all times by the mortuary technician while in the mortuary…. In this instance, however, the undertaker was allowed to locate the body he had come to collect unaccompanied.’ This most often concerned interactions with funeral directors. Reports commonly described mortuaries allowing funeral directors unsupervised access to body stores, having no appointment or queuing system for collections, dealing with more than one collection at a time, overlooking omissions or discrepancies in the paperwork required to collect bodies. Such informality contributed to identification errors, leading to incidents where the wrong body was released.
Patient characteristics
Patient remains at either end of the extreme of body size were found to be a contributory cause of several storage incidents. In four incidents, obesity contributed to adverse outcomes. As the bodies did not fit into standard refrigerators they were left outside a temperature-controlled environment contributing to both decomposition and misidentification in communal areas. Conversely, physically small fetal remains lent themselves to storage in communal areas leading to them being overlooked and retained incorrectly.
Discussion
Serious incidents involving a dead body are uncommon. We found a reported rate of less than one per month although the true frequency may be higher because some degree of under-reporting is likely. However, such occurrences harm families, lead to loss of clinical and forensic information, and can damage trust in healthcare organisations. Some high-profile healthcare incidents involving the living, for example wrong site surgery, are also uncommon but considered unacceptable. 20 Just as wrong site surgery should never be acceptable, so the release of the wrong body to an undertaker should be unacceptable.
We believe that our study is the first to systematically examine serious incidents of this nature. The ability to access a national database of serious incidents, governed by mandatory reporting, has enabled an analysis that goes beyond case reports of isolated instances and explores underlying patterns of error. There is the possibility that the mortuaries in which the incident reports included in our study arose from are unrepresentative of mortuaries in general and are only the extreme end of poor practice. However, the consistency of the types of incidents and the contributing factors underlying them are conspicuous.
We found a systemic pattern of error that transcended individual localities. These involved the management of bodies, both across the period of the study and between organisations. Misidentification of bodies, and failures to catalogue and monitor the contents of mortuaries, repeatedly led to the retention or loss of human remains and the wrong bodies undergoing postmortem examination, being buried or being cremated. Nearly one-quarter of all reported incidents in our study involved fetuses. This remains a deeply sensitive and contentious area that is a rigorous test of the quality of patient-centred care. A hospital board and its senior executives cannot promote their values in this regard if they fail parents by presiding over incidents in the management of the bodies of their precious children. The handling of such cases is complex because of the statutory elements governing procedures and the importance of observing the wishes of the parents. It is true that the small size of the fetuses leads to them often being stored in communal clinical and mortuary areas, predisposing to misidentification. However, this is the very reason that a very high standard of procedure is needed.
What is striking in this study of a novel field of healthcare risk is how the findings resembled those incidents occurring before death. ‘Patient accident’, ‘Documentation (including identification)’, ‘Infrastructure’, ‘Consent, communication and confidentiality’ and ‘Treatment, procedure’ are all included in the ten most frequent incident types reported to the NHS. 21 If disfigured or decomposing bodies are considered analogous with ‘patient accident’, and postmortem examination is equivalent to a ‘procedure’, then these five incident types account for well over half of the incidents included in our study. We also found similarities in causal factors. Poor communication is a well-known hazard in clinical care, particularly at points of handover between providers.22,23 We found problems in interdepartmental working were a key factor in many of the incidents in our study, particularly the transfer of fetal remains from maternity departments to the mortuary. Misidentification of patients is a common cause of wrong site surgery 24 and other patient safety incidents. 21 Likewise, misidentification of bodies underlay many incidents with well-known risks such as same or similar names contributing. Misconduct by staff is generally viewed as an exceptional cause of patient safety incidents. 25 This was reflected in our study with only eight incidents due to alleged staff misconduct.
These similarities in causation point to the opportunity for hospitals, their pathologists and their mortuaries to learn from successful solutions in other fields of patient safety. For example, standardisation of workflows has been shown to improve outcomes in other settings12,26–28 and could be applied to the management of bodies arriving in the mortuary. Automation of procedures, including a greater use of information technology, also has the potential to help prevent errors, for example it could be used to highlight same-name dangers automatically and ensure that bodies are linked to associated body parts reliably.
Another fundamental aspect of safety in all sectors, not just healthcare, is human factors. 12 They have been shown to form a vital part in both understanding incidents and in devising solutions. For example, we found that working relationships with funeral directors were important in potentially reducing the risk of harmful events. Good cooperation can avoid adverse outcomes, shown in willingness of funeral directors to collect bodies at short notice following refrigerator failures. On the other hand, we found undue informality, such as allowing the unsupervised collection of bodies, can produce mistakes. Informality in the management and governance of the mortuary is a human factors element that can be detrimental to patient safety. We found that extensive delegation of tasks to mortuary workers contributed to poor standards of practice and subsequent errors. A case in point was our finding of misidentification errors due to processing several bodies at once or setting bodies out for simultaneous postmortem examinations.
The findings of our study serve as a warning to those responsible for the management of mortuary services of the significant risks inherent in such services and the potentially devastating incidents that can occur if these risks are not mitigated and errors allowed to go unchecked. It also highlights areas that system improvement efforts can usefully be targeted in and approaches that have been shown to be successful in other areas of healthcare.