
Abstract

Insanity is doing the same thing over and over again and expecting different results (Albert Einstein)
Mosquito mesh for hernia repair and Operation Hernia.
To what extent do healthcare professionals and decision-makers look to other industries and other countries to find those innovative low-cost models of care that benefit the system without compromising on quality? Where do people on the frontline of healthcare look for innovative solutions to the clinical and organisational problems that they and their patients face? This is important, because what you find depends on where you look. 9
The Global Diffusion of Healthcare Innovation study10,11 recently explored which are the dominant sources of ideas for Frontline Healthcare Workers in the health systems of six countries (USA, England, Brazil, Tanzania, Qatar and India). 12 The study drew on quantitative surveys of more than 1350 Frontline Healthcare Workers and asked them where, in terms of industry, media and country, did their main idea to improve clinical practice in their health system in the last 12 months come from. The study found that the majority of Frontline Healthcare Workers (ranging from 91% in India to 82% in the US) stated that their ideas to improve healthcare practice or delivery were derived from their own clinical specialty. Only 5% of Frontline Healthcare Workers report that their idea was influenced by sectors unrelated to healthcare. Only 11% of Frontline Healthcare Workers reported that their ideas were influenced by practice in other countries, although higher proportions do so in Brazil (18%), Tanzania (12%) and, to a lesser extent, India (10%). Organisations that have the useful function of curating under-the-radar innovations from around the world (such as the Center for Health Market Innovations, the US Commonwealth Fund, in India the Centre for Innovations in Public Systems, in England the NHS Health and Care Innovation Expo) were noted by only 10%.
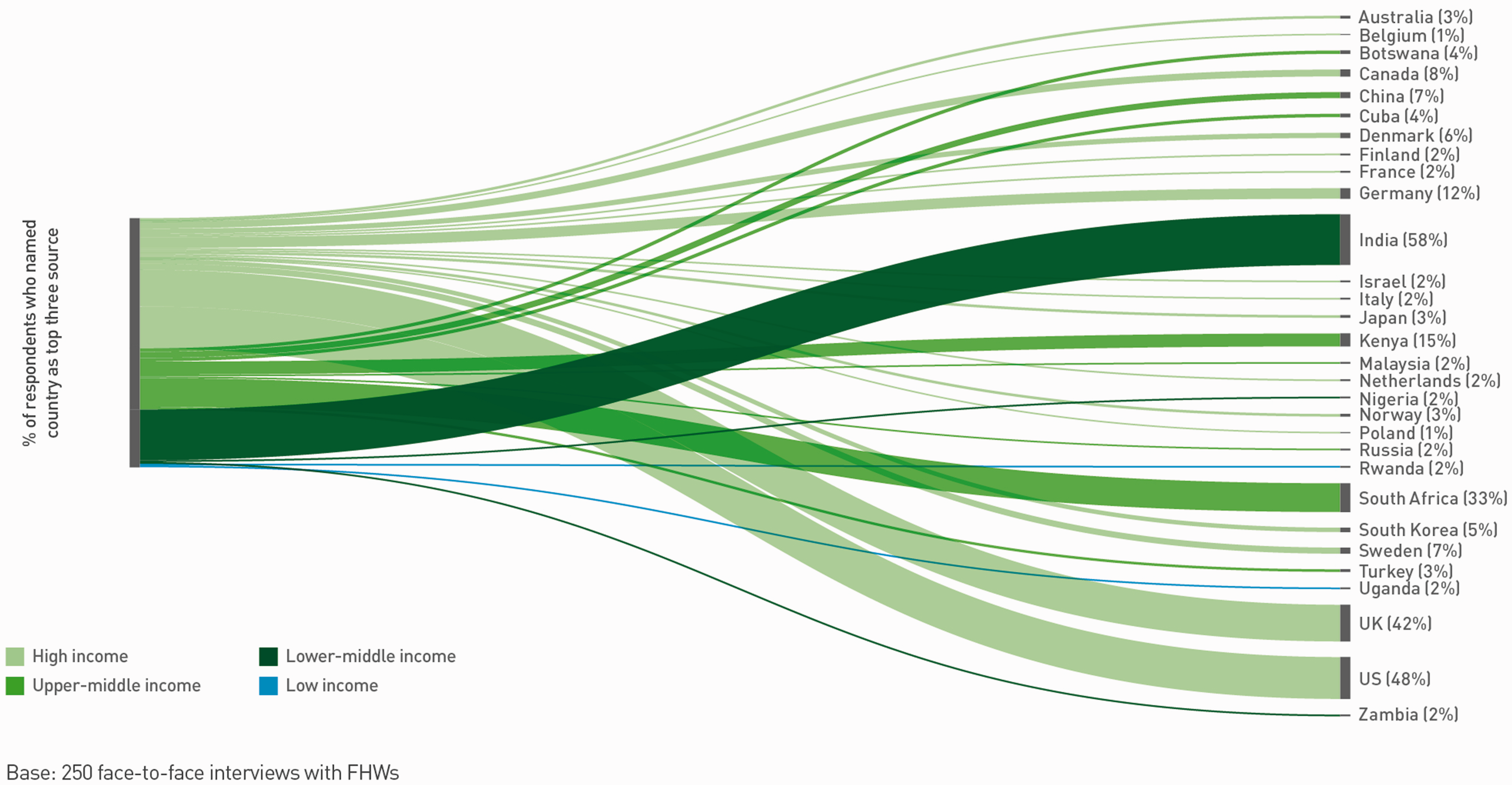
The Global Diffusion of Healthcare Innovation study also asked respondents which three countries are most important as a source of useful ideas for their healthcare system. The USA and UK rank as the two most important sources of innovation across the six countries studied, with two-thirds of Frontline Healthcare Workers mentioning the USA and almost half mentioning England or the countries of the UK. Beyond these two countries, Canada (23%), Germany (20%), India (16%), France (13%) and Australia (12%) are the highest ranked. However, there were significant differences in the patterns between country-level responses, with healthcare workers from the UK tending to focus on high-income, OECD countries (Figure 1) and healthcare workers from Tanzania demonstrating a far richer diversity of influential sources (Figure 2).
Countries most frequently cited as useful sources of innovation by Frontline Healthcare Workers in the United Kingdom (reproduced with permission from the Global Diffusion of Healthcare Innovation report 2016). Countries most frequently cited as useful sources of innovation by Frontline Healthcare Workers in Tanzania (reproduced with permission from the Global Diffusion of Healthcare Innovation report 2016).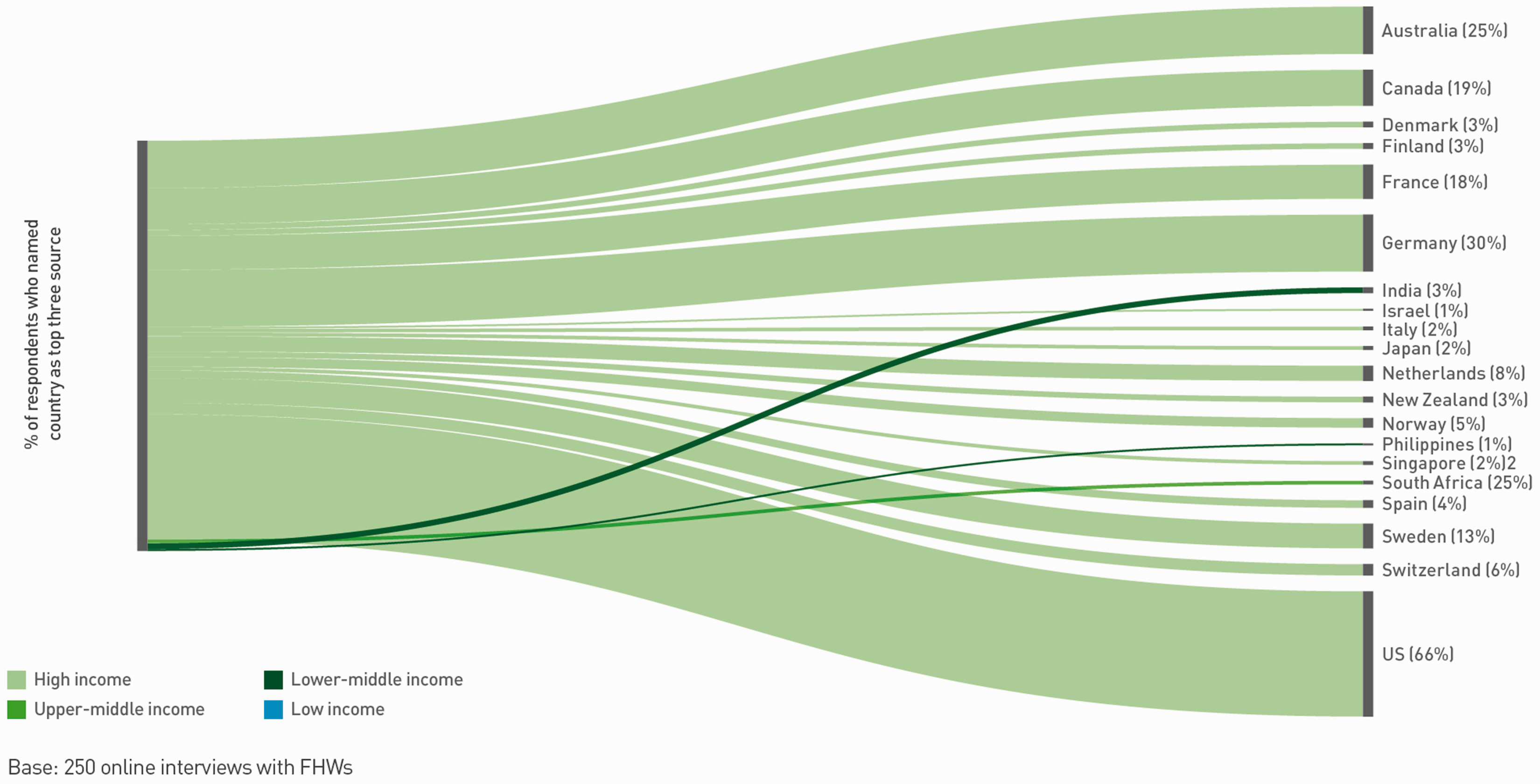
The findings from this study set a benchmark but there are clear tendencies and trends, first that Frontline Healthcare Workers are not looking far afield, and are not being influenced by sources beyond their own intellectual and physical locale, but also that there are only a handful of countries, predictably perhaps, that are noted to be influential. It is unlikely that connections will be made between the diverse perspectives of different disciplines, and some contexts are perhaps discounted too early on. Little is known about what drives Frontline Healthcare Workers to consider knowledge from one context or industry to be relevant or useful, but certainly low- and middle-income countries are not an influential source in the developed economies that were included in this study. Perhaps this is a missed opportunity?
This focus on the demand or ‘pull’ for innovation, rather than the supply of innovation, is a novel perspective for the literature about diffusion of innovation, which traditionally emphasises how to ‘push’ innovations out into wider practice. However, if we do not understand clinicians’ appetite for knowledge and what constitutes legitimate sources of new knowledge, then we will not understand how to leverage new innovation from new sources.
Making connections and looking beyond one’s usual sphere of influence, wherever it may be from, is important to identify and capture the opportunities of low-cost innovation for the benefit of improved patient experience and improved quality of care. Reverse innovation occurs when models of care, technologies, procedures and products, developed by and for low- and middle-income countries, are implemented in high-income country health systems and, albeit a term that can appear paradoxical, 13 challenges the assumption that high-income countries are best at innovating. Low- and middle-income countries can offer high-income countries simple and cost-effective, but potentially disruptive, healthcare delivery models and technologies for better health outcomes. In any country where resources are scarce, leaner, more efficient models are needed, wherever they are from. Sectors unrelated to healthcare, such as retail or transportation industries, can provide comparable lessons for improved management of healthcare supply and patient safety.
Health workers and leaders should welcome unusual sources of innovation. However, searching is time-consuming. A critical enabler to finding low-cost innovation is the extent to which clinicians and health policy-makers are able to, or have the tendency to, look further afield than their own specific area of expertise or trusted knowledge network. How do people do things in other hospitals, other regions, other countries and other industries? New knowledge, new techniques, new ideas and new processes will be generated by not looking at usual sources. Important strategies for healthcare organisations include: first, to develop and communicate a strategy for innovation, including sourcing, where healthcare workers are encouraged to look as far afield as possible for inspiration. Second, to purposefully draw on the services of organisations that offer an innovation curator service (such as the Center for Health Market Innovations, the US Commonwealth Fund, in India the Centre for Innovations in Public Systems, in England the NHS Health and Care Innovation Expo) collating case studies of innovations from a diverse array of industries and countries and serving as valuable repositories of information of under-the-radar technologies and solutions. Third, to develop international health partnerships with hospitals and other clinical services in low- and middle-income countries and beyond. These partnerships should ensure that clinicians and managers are engaged in a genuine learning process with the partner organisation and actively seek to pilot innovations from other countries. Recent research has shown many benefits, particularly at the individual level, of international placements, 14 but more work needs to be done to explicitly bring learning back to the UK and other high-income health systems. 15 Finally, to address issues of clinical homophily, medical schools should consider education and training for innovative thinking, and to promote wider searching for innovation and deliberate lateral thinking.
Conclusion
In the UK, as in the USA, growing demands on care necessitate an open-mindedness to look to low-income countries as well as other industries. For the truly breakthrough opportunities in healthcare to emerge, Frontline Healthcare Workers will need to boldly go where they do not usually go to harness the power that linking disciplines or industry sectors has to create disruptive innovations.