
Abstract
Objective
To examine associations between the contract and ownership type of general practices and patient experience in England.
Design
Multilevel linear regression analysis of a national cross-sectional patient survey (General Practice Patient Survey).
Setting
All general practices in England in 2013–2014 (n = 8017).
Participants
903,357 survey respondents aged 18 years or over and registered with a general practice for six months or more (34.3% of 2,631,209 questionnaires sent).
Main outcome measures
Patient reports of experience across five measures: frequency of consulting a preferred doctor; ability to get a convenient appointment; rating of doctor communication skills; ease of contacting the practice by telephone; and overall experience (measured on four- or five-level interval scales from 0 to 100). Models adjusted for demographic and socioeconomic characteristics of respondents and general practice populations and a random intercept for each general practice.
Results
Most practices had a centrally negotiated contract with the UK government (‘General Medical Services’ 54.6%; 4337/7949). Few practices were limited companies with locally negotiated ‘Alternative Provider Medical Services’ contracts (1.2%; 98/7949); these practices provided worse overall experiences than General Medical Services practices (adjusted mean difference −3.04, 95% CI −4.15 to −1.94). Associations were consistent in direction across outcomes and largest in magnitude for frequency of consulting a preferred doctor (−12.78, 95% CI −15.17 to −10.39). Results were similar for practices owned by large organisations (defined as having ≥20 practices) which were uncommon (2.2%; 176/7949).
Conclusions
Patients registered to general practices owned by limited companies, including large organisations, reported worse experiences of their care than other patients in 2013–2014.
Keywords
Introduction
General practices in England are independent businesses contracted to provide primary care for specified populations. Most are owned by general practitioners, but many types of organisation are now eligible to deliver these services. For the first 50 years of the National Health Service, a general practice typically comprised one or more general practitioners working in common premises under a standard contract with the UK government. New types of contract were introduced in 1998 and 2004 that are locally negotiated and allow commercial, voluntary sector and other new providers to offer general practice services (online supplementary material – Appendix 1). 1 Several governments have attempted to increase the role of non-traditional providers across many parts of the National Health Service over the past 17 years.2–4 Limited companies – businesses with a separate legal identity to their owners – currently own less than 5% of general practices; 5 their likely share of the market in the future is unclear.
Other countries have experienced changes in the ownership of primary care providers. In Sweden, patient choice of primary care provider and free establishment of accredited ‘private’ providers became mandatory in 2010; large national corporations, including those owned by venture capitalists, now run around one-third of private providers. 6 In Australia, primary care has been increasingly corporatised since the 1990s when publicly listed companies first entered the market; three national or international companies received around 12% of market revenue in 2011. 7 Opponents argue that the profit motive of these organisations could lead them to compromise patient care, while those in favour suggest they will bring greater innovation. 8 A national cross-sectional time series analysis of general practices in England suggested, using aggregate data, that non-traditional providers performed worse across 15 of 17 quality indicators studied from 2008 to 2013. 1
Patient experience is a key domain of performance in the English National Health Service. Measures of patient satisfaction with general practice services are monitored nationally 9 and presented to patients for each practice on an information website. 10 These measures are derived from an annual national survey of patients registered with a general practitioner – the General Practice Patient Survey. 11 Questionnaires include items on practice organisation, appointment experiences and patient characteristics. 12 Previous multilevel analysis of the survey suggests that commercial providers of out-of-hours primary care (weekends and 18:30 to 08:00 on weekdays) provided a worse experience of these services than National Health Service and not-for-profit providers in 2012–2013. 13 No studies had conducted a similar analysis, using the multilevel structure of the data, for in-hours general practice services.
We examined the association between patient experience and the contract type of general practices in England, distinguishing limited companies from other practices. We also examined the performance of organisations that owned 20 or more practices, using five measures from the General Practice Patient Survey 2013–2014: continuity of care; appointment convenience; doctor communication; ease of telephone contact; and overall experience.
Methods
Patient survey questionnaires
We analysed data from the English General Practice Patient Survey 2013–2014 (July to September 2013 and January to March 2014). Patients were eligible for inclusion in the survey if they had a valid National Health Service number, had been registered with a general practice for six months or more, and were aged 18 years or over. 14 All general practices in England with eligible patients were included in the survey (n = 8017). 14 Postal questionnaires were sent to stratified random samples of patients from each practice, with 903,357 responses for 8005 practices (34.3% of 2,631,209 questionnaires sent). 14 This provided 113 responses per practice on average (standard deviation 18.5) which allows most measures to have good (≥0.8) or excellent (≥0.9) practice level reliability. 15
We used five patient experience measures as outcomes: the frequency of consulting a preferred doctor; ability to get a convenient appointment; rating of doctor communication skills; ease of contacting the practice by telephone; and the overall experience. These were assessed using four- or five-point response scales, ranging, for example, from ‘very good’ to ‘very poor’ for overall experience (online supplementary material – Appendix 2). The measure of doctor communication was a composite of five questions. 16 We chose these outcome measures because they are important to patients, will be affected by organisational characteristics, have sufficient practice level reliability and are policy-relevant.15,17,18 All outcomes relate to in-hours, rather than out-of-hours, services.
We included five patient characteristics from the questionnaires in analyses: age (eight ordinal categories); gender; ethnicity (White, mixed, Asian, Black, other); confidence in managing own health (four ordinal categories); and the ability to take time off work to see a general practitioner (no, yes, not working). Socioeconomic status was measured as fifths of the Index of Multiple Deprivation rank for the small geographic areas (lower layer super output areas with a mean population of 1500) in which patients lived. 19 Similar case mix adjustors have been used in analysing the General Practice Patient Survey previously.13,20
General practice ownership
We obtained routine contract data for 7949 general practices included in the General Practice Patient Survey; these data were taken from general practice computer systems in September 2013. 21 The four types of contract were: ‘General’, ‘Personal’, ‘Alternative Provider’, and ‘Primary Care Trust’ – all suffixed with ‘Medical Services’ (online supplementary material – Appendix 1). Limited companies operate under the first three types, giving seven categories of contract in total. In our first analysis, we compared patient experience across these seven categories, distinguishing limited companies from other ownership forms. We refer to practices with each contract by the differentiating first part of the contract name in the remainder of the article (e.g. Alternative Provider practices).
In our second analysis, we identified general practices owned by large organisations (defined as having 20 or more practices) from existing literature, published data and provider websites.3,22–26 We thought that each large organisation would list a representative sample, if not all, of its practices on its website; in case not, we searched for additional practices using National Health Service and regulator datasets that gave organisation names.23,25,26 We then compared the patient experience measures between practices owned by large organisations and practices operating under a General contract (typically small general practitioner partnerships working in a single practice). Each large organisation was registered as a limited company. However, some practices owned by large organisations were not recorded as limited companies in the contract data, possibly due to separate legal identities in complex business structures. Some practices registered as limited companies were not owned by large organisations.
We included four characteristics of each general practice’s registered population in analyses: population size; 21 age–gender profile (percentages in six age categories for male and female patients); 21 ethnicity profile (percentages White, mixed, Asian, Black, other); 27 and the Index of Multiple Deprivation 2010 rank for the practice population. 28 Population sizes and age–gender profiles were extracted from general practice computer systems in September 2013. 21 Ethnicity data were taken from the 2011 census. 27
Statistical methods
Descriptive statistics for patient characteristics and outcome measures included all survey respondents. We excluded uninformative questionnaire responses (such as ‘Can’t remember’) from all analyses, 13 which accounted for small percentages of responses for each outcome measure (3% for ease of telephone contact, for example). When estimating associations between patient experience measures and explanatory variables, we excluded observations with missing data for any of the variables included in the estimation. We further excluded patients registered to general practices with fewer than 1000 patients or fewer than 50 responses to the General Practice Patient Survey (2% of practices);1,29,30 this omitted practices serving atypical populations or those with unreliable practice level scores for the outcomes.
We linearly rescaled each outcome measure to a 0–100 scale to help compare scores across measures (online supplementary material – Appendix 2). 31 We first estimated the associations between patient experience (measured at the patient level) and the contract type of general practices using linear mixed-effects regression models that included random practice-level intercepts and adjusted (at the patient level) for the six patient characteristics given above. We then extended these models to include the population size, age–gender, ethnicity and deprivation profiles of each general practice as covariates. These characteristics vary across practices with different contract types 1 and are associated with patient experience independent of the corresponding patient characteristics. 32 These models are therefore better adjusted for confounding variables and we present them in the subsequent main text; the results unadjusted for population characteristics are given in the online supplementary material. We repeated this analysis to estimate the association between patient experience and practice ownership by a large organisation.
We present the mean differences in each outcome measure between practices with General contracts (the reference category) and practices in other categories. We also provide standardised mean differences, calculated by dividing the mean difference by the standard deviation between general practices derived from the multilevel regression models, to indicate the strength of associations. Results for practices with Primary Care Trust contracts are presented in the online supplementary material, since these trusts (responsible for commissioning primary care and other services) were abolished in March 2013 and this contract type is no longer recorded. 33 We also restrict detailed results for practices recorded as limited companies with General or Personal contracts in the contract data to the online supplementary material, as there were only 18 of these practices.
In a sensitivity analysis, we used propensity-score matching to compare outcome measures between practices identified as Alternative Provider limited companies and those with General contracts. We used logistic regression to estimate the propensity score based on the patient and practice characteristics given above. Each respondent whose practice was an Alternative Provider limited company was then compared to 100 other respondents with similar propensity scores whose practices had General contracts (nearest neighbours matching with replacement).20,34 We excluded respondents without a suitable match (due to non-overlapping propensity scores). We used standardised mean differences in patient and practice characteristics to assess the quality of matching between the two types of practices. This sensitivity analysis was then repeated comparing practices owned by a large organisation to practices with General contracts. All analyses were conducted using Stata MP v.13 (StataCorp, College Station, TX, USA).
Results
Characteristics of respondents to the General Practice Patient Survey 2013–2014.

GP: general practitioner. 903,357 responses in total from patients registered to 8005 general practices in England.
Based on the Index of Multiple Deprivation rank for a patient’s area of residence.
Not in paid work (e.g. retired, in full-time education, unemployed).
Responses describing patient experience of general practice across five measures: overall experience; consulting a preferred doctor; getting a convenient appointment; doctor communication skills; and ease of telephone contact.

GP: general practitioner. 903,357 responses in total from patients registered to 8005 general practices in England.
Responses are for patients who report having a particular GP they usually prefer to see or speak to.
Relates to the last time a respondent wanted to see or speak to a GP or nurse from their GP surgery. ‘No appointment’ was determined from a preceding question ‘Were you able to get an appointment to see or speak to someone?’
Question asked for five communication skills from the last time a respondent saw or spoke to a GP from their GP surgery: giving you enough time; listening to you; explaining tests and treatments; involving you in decisions about your care; and treating you with care and concern. The categories given are defined using the mean score (x) over the five questions: ‘very poor’ (x<12.5); ‘poor’ (12.5≤x<37.5); ‘neither good nor poor’ (37.5≤x<62.5); ‘good’ (62.5≤x<87.5); and ‘very good’ (x≥87.5).
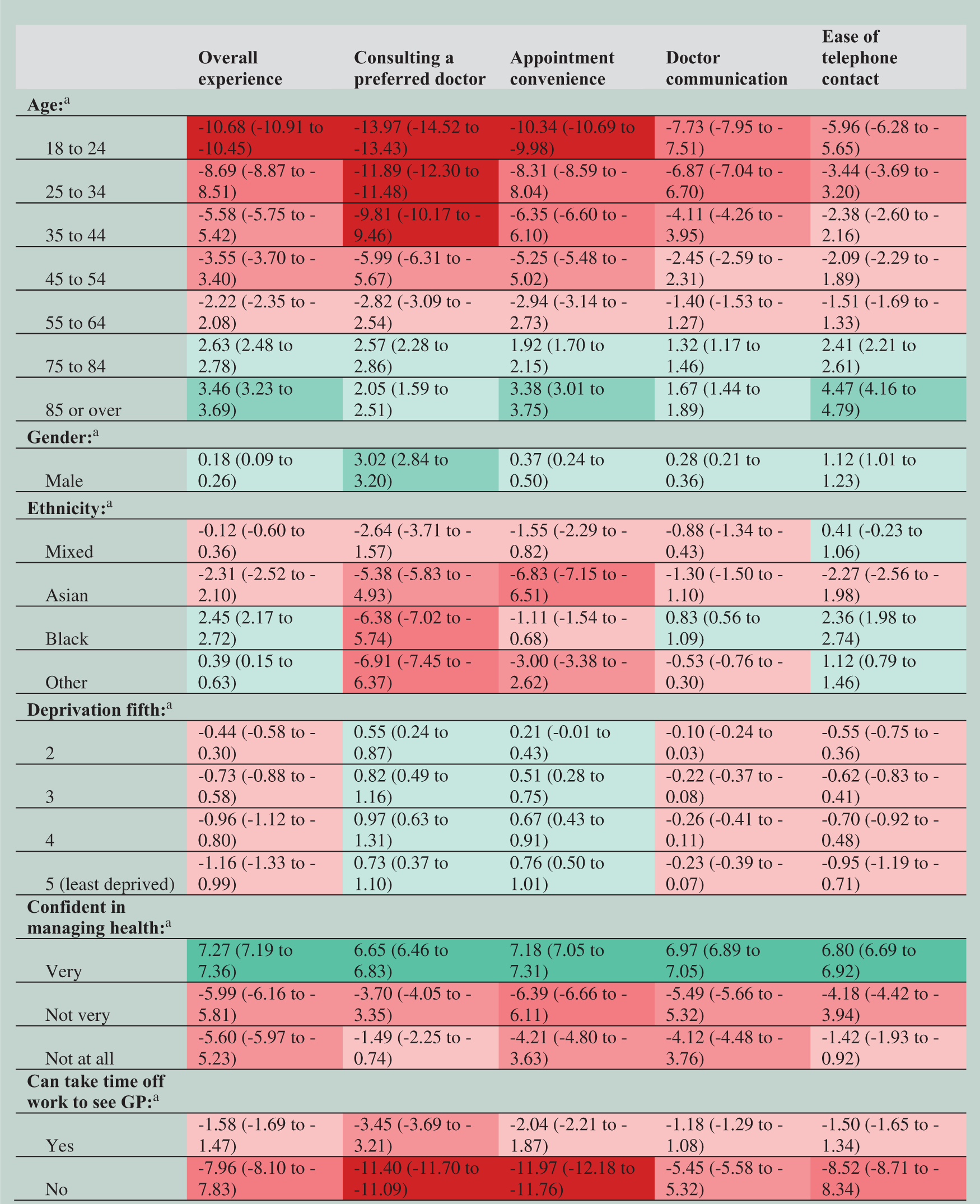
Adjusted associations between patient experience and characteristics of survey respondents, derived from a multilevel linear regression model.
Contracts held by general practices.
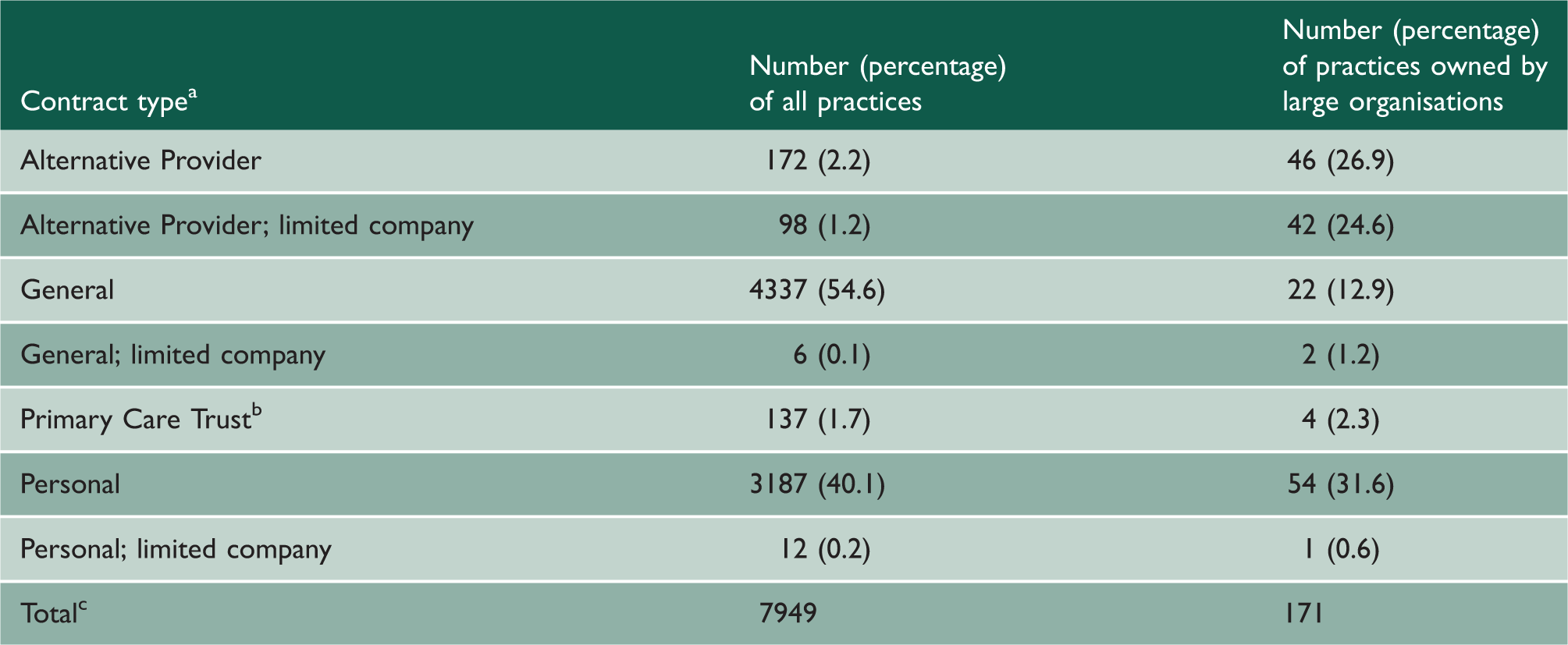
All contract types suffixed with ‘Medical Services’ (e.g. General Medical Services).
Large organisations defined as organisations that own ≥20 general practices.
Limited companies are identified in the contract data under three categories as given.
Primary Care Trusts were abolished in March 2013 under new legislation; this contract is not recorded in 2014−2015 data. 33
Contract data were unavailable for 56 general practices included in the General Practice Patient Survey and five practices identified as being owned by a large organisation.
Practices with Alternative Provider contracts, both limited and non-limited forms, had greater percentages of respondents in younger, non-White and more deprived categories than other practices (online supplementary material – Appendix 3). This reflected differences in the registered populations of these practices (online supplementary material – Appendix 4). Alternative Provider practices and Personal limited companies had the smallest registered populations on average, while other Personal practices had the largest mean population (online supplementary material – Appendix 4).
Adjusted associations between patient experience and type of general practice contract, derived from a multilevel linear regression model.
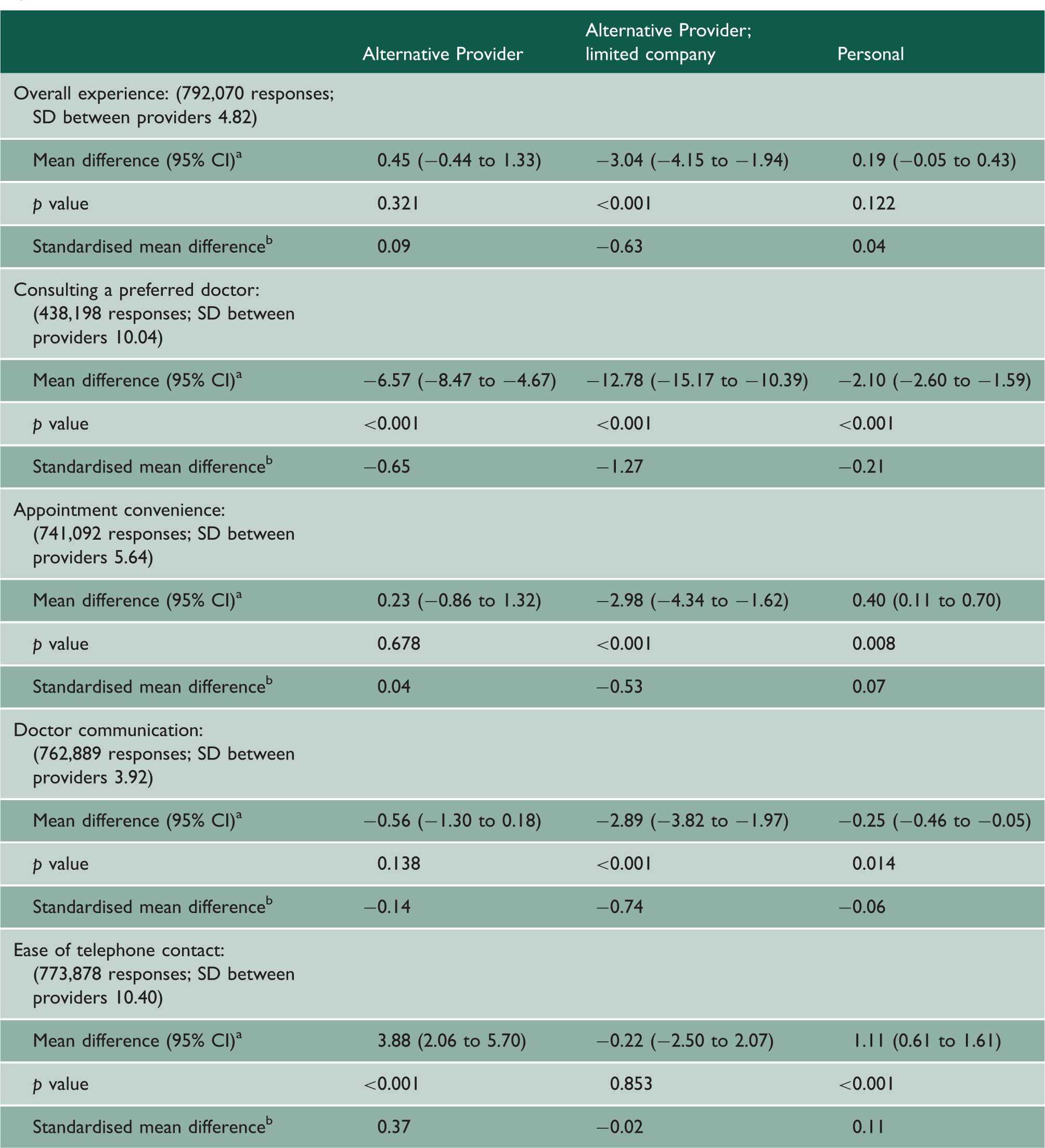
Note: Figures are presented as mean differences relative to practices with General contracts.
SD: standard deviation. 7835 general practices are included in each analysis.
All contract types suffixed with ‘Medical Services’ (e.g. General Medical Services).
Regression model adjusted for respondent age, gender, ethnicity, socioeconomic status, confidence in managing own health and ability to take time off work to see a general practitioner; general practice population size, age–gender, ethnicity and deprivation profiles; and included a random intercept for general practice.
All mean differences are relative to the means for general practices with General contracts.
Standardised mean differences are equal to the mean difference divided by the between provider standard deviation for a given outcome measure estimated for the regression models.
Where Alternative Provider limited practices did score lower, the standardised mean differences were −0.63, −1.27, −0.53 and −0.74 for overall experience, consulting a preferred doctor, getting a convenient appointment and doctor communication skills, respectively (Table 5). This indicates moderate (appointment convenience) to large (preferred doctor) effect sizes of being an Alternative Provider limited practice.
Differences between practices with Personal contracts and those with General contracts were small (modulus of standardised mean differences ≤0.21) and inconsistent in direction across measures (Table 5). Practices recorded as limited companies with Personal contracts performed worse on four of five measures; however, with similar standardised mean differences as for Alternative Provider limited practices (online supplementary material – Appendix 3). Alternative Provider practices not identified as limited companies in the contract data were easier to contact by telephone than practices with General contracts (standardised mean difference 0.37; Table 5). Patient experience in Primary Care Trust practices did not differ consistently across measures to that in practices with General contracts (online supplementary material – Appendix 5).
Adjusted associations between patient experience and large organisation ownership of a general practice, derived from a multilevel linear regression model.
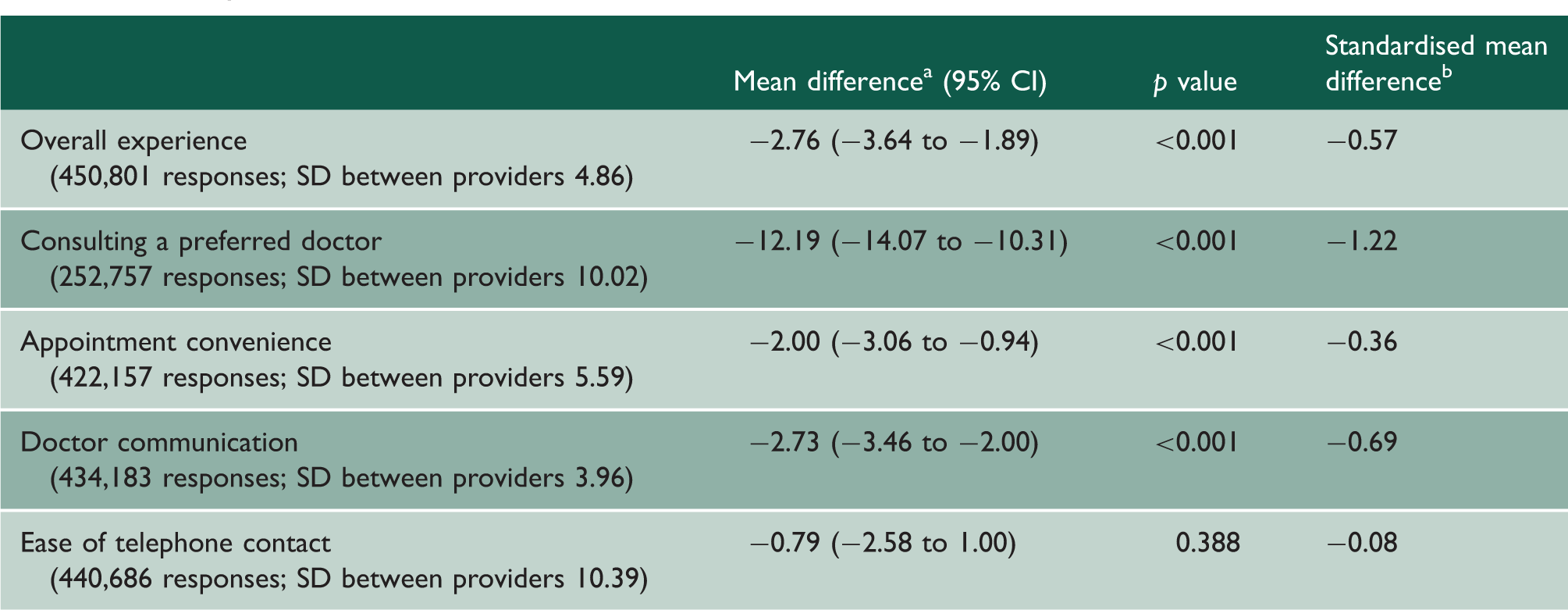
Note: Figures are presented as mean differences relative to practices with General contracts.
SD: standard deviation. 4432 general practices are included in each analysis: 163 owned by a large organisation; 4269 with a General contract.
Regression model adjusted for respondent age, gender, ethnicity, socioeconomic status, confidence in managing own health and ability to take time off work to see a general practitioner; general practice population size, age–gender, ethnicity and deprivation profiles; and included a random intercept for general practice.
All mean differences compare means for general practices owned by large organisations with means for practices with General contracts (typically small GP partnerships working in a single practice).
Standardised mean differences are equal to the mean difference divided by the between provider standard deviation for a given outcome measure estimated for the regression models.
The results in both analyses were similar to those given above when characteristics of each general practice’s population were not adjusted for (online supplementary material – Appendix 6). In the sensitivity analysis using propensity-score matching, the estimated associations were similar in direction and magnitude to the results from regression modelling (online supplementary material – Appendix 7).
Discussion
Patients registered to general practices owned by limited companies reported worse experiences of their care than patients registered to other practices on average. This applied to practices recorded as limited companies in routine contract data and to practices owned by large organisations. The sizes of the differences in experience varied from moderate to large across four outcome measures and were largest for the frequency of consulting a preferred doctor. Limited company ownership of general practices is uncommon in England. Patient experience was not consistently associated with the contract type for practices not recorded as limited companies. Across all contract and ownership types, patients generally reported positive experiences of their general practices.
Relation to existing literature
A national ecological analysis of general practices in England found that Alternative Provider practices performed worse across 15 of 17 outcome measures studied from 2008–2009 to 2012–2013. 1 Most of these practices (53%; 185/347) were newly established, but the practices that changed to an Alternative Provider contract did not appear to worsen care on average. 1 A relative strength of the analysis presented here is that we adjusted for patient level variables that confound the relationship between contract type and patient experience. Our results suggest that Alternative Provider practices consistently provided a worse experience for patients only when owned by limited companies. This contrasts with the previous analysis which observed the association for all Alternative Provider practices. 1 We additionally found that practices owned by large organisations (≥20 practices) provided worse experiences on average than practices with a General contract which are typically small general practitioner partnerships. Therefore, our findings highlight limited companies as providing worse experiences of primary care, rather than practices with the Alternative Provider contract collectively.
Commercial providers of out-of-hours primary care in England provided a worse experience of care across three outcome measures than National Health Service or not-for-profit providers in 2012–2013; 13 the effect sizes were large for two outcomes (overall experience, confidence and trust in the out-of-hours clinician) and moderate for the other (timeliness of care). This analysis used a similar design – multilevel analysis of the General Practice Patient Survey – to that reported here. Analysis of the 2007–2008 version of the survey found no substantial differences in patient experience between General and Personal practices, 32 which is consistent with our results.
The results are also consistent with several articles that report associations between survey respondent characteristics and reported experiences.13,16,31,32,35 Respondents from younger age groups, who were not very confident in managing their own health or who could not take time off work to see a general practitioner, reported substantially worse experiences across outcome measures.
Strengths and limitations
The General Practice Patient Survey is a large nationally representative survey providing sufficient numbers of responses per practice to create reliable practice-level measures. 15 We examined policy-relevant measures of patient experience such as the convenience of appointments 17 and overall experience which is monitored in the National Health Service Outcomes Framework. 9 We used the multilevel data structure to estimate associations while adjusting for key characteristics of survey respondents and practice populations.
Given the observational cross-sectional design of the analysis, residual confounding may account for some or all of the differences observed between ownership types. We did not determine whether changes in practice contract type and ownership over time are associated with changes in patient experience. This was because relatively few practices change contract type each year and there is much random variation in changes in the patient experience measures within practices between years. An alternative explanation for the results is that limited companies may often take over practices that already provide a poor experience of care; it may then be difficult to improve patient experience to the average levels of other practices. However, we may also expect this of Primary Care Trust practices or Alternative Provider practices not owned by limited companies, and these practices provided similar patient experiences to practices with General contracts. Moreover, past poor performance may not be a reasonable justification of current poor performance. Of the 98 Alternative Provider limited companies in 2013, 71 had the same contract and ownership status in 2012, 65 in 2011 and 59 in 2010.
Patient reports of experience may be affected by perception of the organisation providing care in addition to the service itself. This depends on patients being aware of the ownership of their general practice which may be atypical. In addition, it is patient perception of experience, regardless of the organisational characteristics that might affect it, that is ultimately important. Patients may recall previous experiences of their general practice inaccurately. This error would have to be systematically associated with the organisation type independent of measured patient characteristics to bias the observed associations, however, which we feel is unlikely. This is also necessary for other sources of response bias. The survey response rate of 34.3% could have biased outcome measures at the practice level, although previous work suggests only a weak inconsistent association between the response rate and two measures of access (partial correlation coefficients of 0.04 and −0.07). 36 Response rates for Alternative Provider limited companies and other Alternative Provider practices were similar (1% difference), so response rates cannot explain differences in associations between these two groups at least.
Most practices owned by large organisations were not recorded as limited companies in the contract data, probably because of complex ownership and legal structures. This supports reclassifying practices using data sources other than those made routinely available when examining practice ownership. However, it may be difficult to identify a representative sample of practices owned by smaller limited companies from Internet searching. We therefore restricted our second analysis to large provider organisations.
Implications for research and policy
Researchers could pursue the explanation for patients reporting worse experiences of care in general practices owned by limited companies. Traditional practices, in which the owners (GP Principals) also provide clinical services, may be more responsive to patient need than practices with more corporate ownership structures. Future research could examine differences in practice staffing and other organisational characteristics that might explain our findings, in addition to using other quality indicators as outcome measures. The performance of corporate providers in other parts of the National Health Service, such as elective surgery, may be worth investigating. Similar research is warranted internationally given the increased role of these providers in several countries.6,7
Limited company ownership of general practices remains uncommon in England. Although our results suggest that limited companies provide worse patient experiences on average, some practices owned by these companies provide a good experience; others provide the opposite. It is the responsibility of commissioners, regulators, clinicians and owners to guarantee that individual practices meet expected standards while ensuring that care quality is not systematically associated with the ownership. Commissioners also need to ensure that contracts offer good value for money, more so at a time when the National Health Service is very financially challenged. 37
Footnotes
Declarations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.